Concussion 2.0
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
concussion
a (mild) traumatic injury that affects the brain, induced by biomechanical forces transmitted to the head by a direct blow to, or forces exerted on, the body (indirect), but that does not result in an extended period of unconsciousness, amnesia or significant neurological signs indicative of a more severe brain injury
*functional, not a structural injury
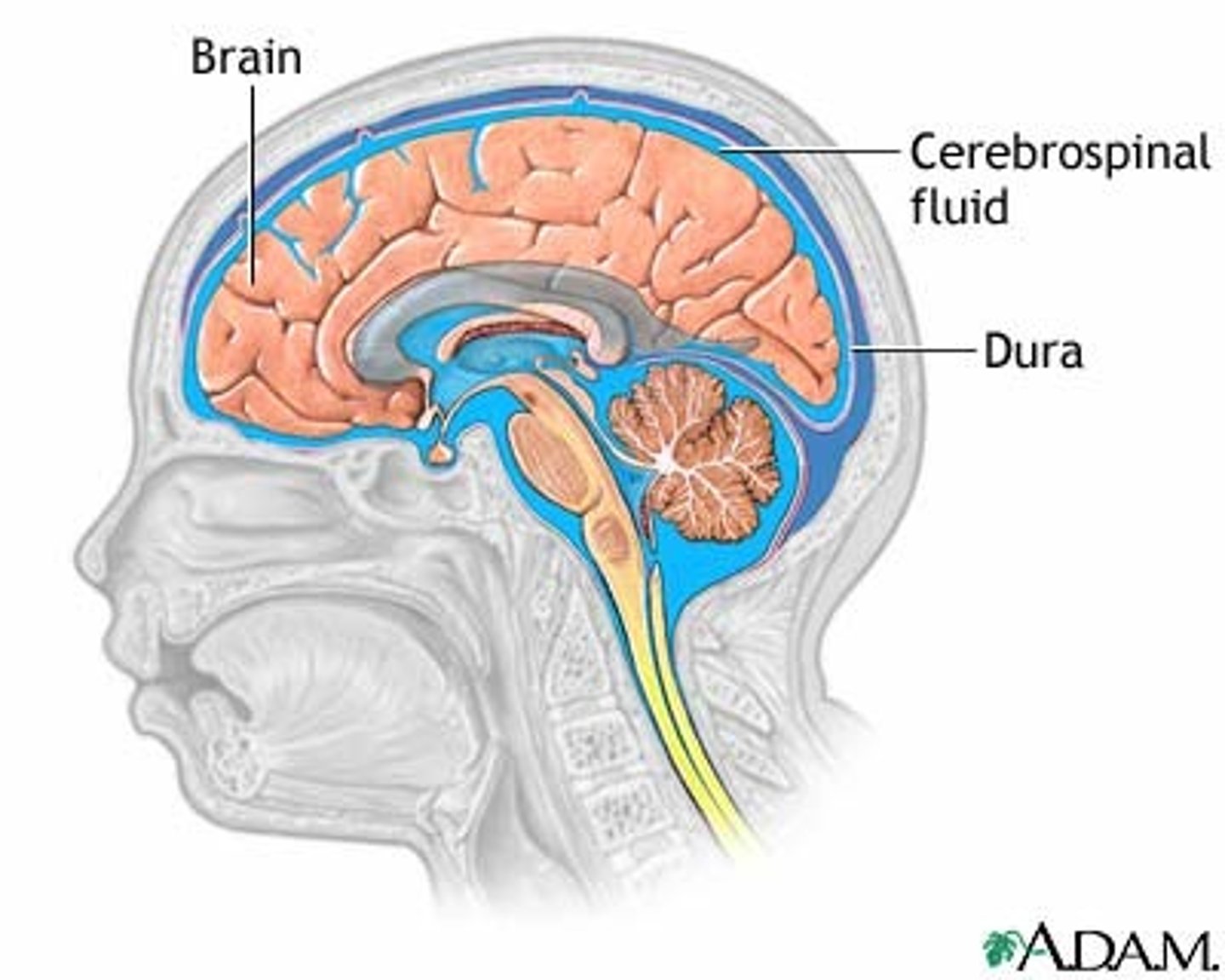
cerebrospinal fluid (CSF)
What fluid surrounds the brain?
damage visible on imaging, significant neurological signs
What makes a TBI considered "severe"?
leading causes of TBI
1. falls (47%)
2. struck by or against (15%)
3. traffic incidents (14%)
4. assault (9%)
5. unknown (8%)
6. other (7%)
sports related concussion (SRC)
15% of students (approx. 2.5 million) reported having at least one concussion during the 12 months
HIGHEST INCIDENCE:
- football
- hockey
- rugby
- soccer
- basketball
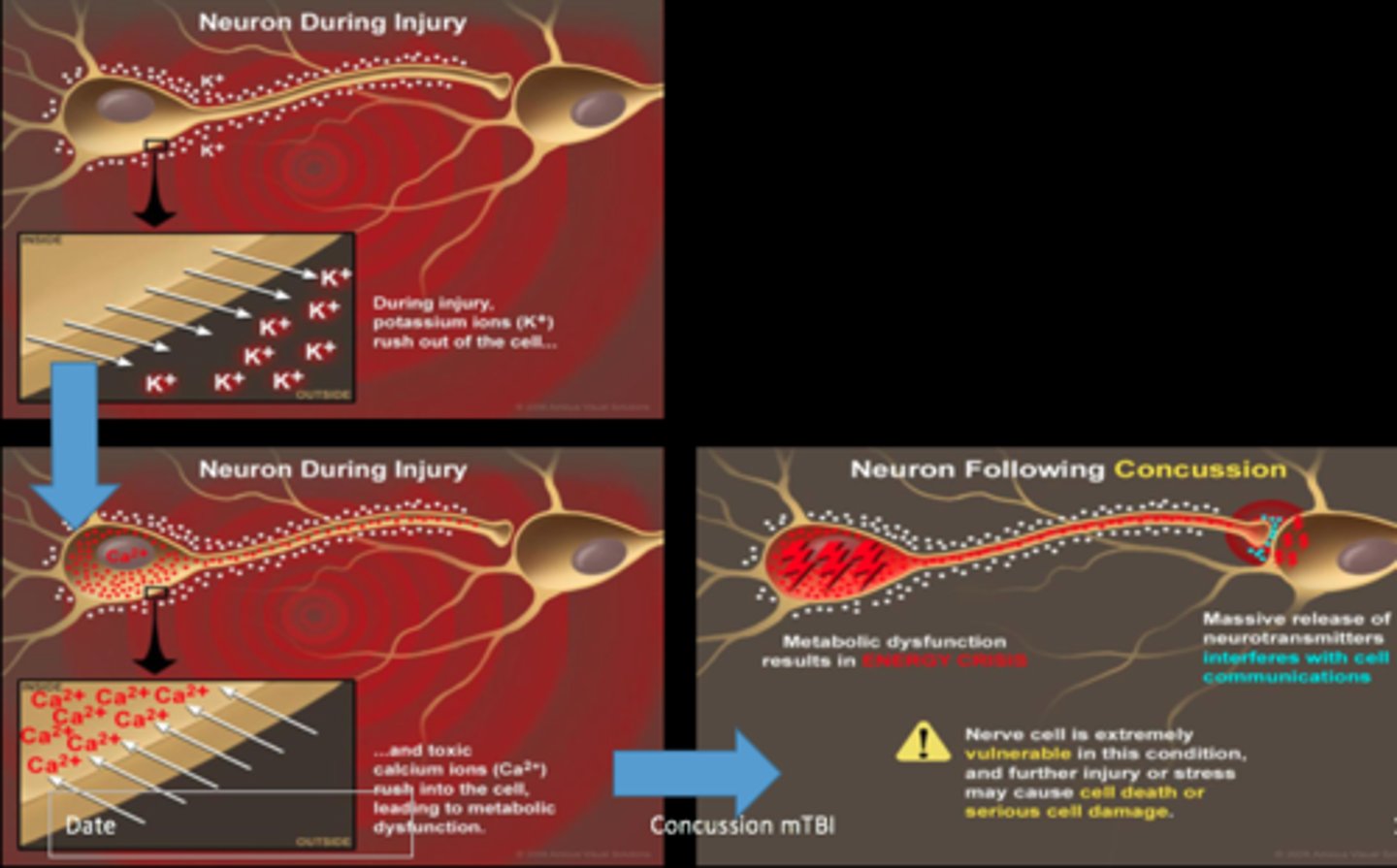
concussion pathophysiology
nerve cells under stress:
- increase glutamate release
- ion imbalance (influx of Ca+, efflux of K+)
- increase in energy demand (up-regulation of ATP pumps)
- decrease blood flow
= ENERGY CRISIS
post concussive syndrome (PCS)
CHRONIC MANAGEMENT
*majority recover within 7-10/14 days
(some cases = prolonged recovery)
1. pre-injury risk factors
2. injury-related risk factors
3. post-injury factors
pre-injury risk factors
AFFECT PCS
- migraine
- learning disability
- ADHD
- sex (females)
- age (younger)
- previous concussion
- genetics
injury-related risk factors
AFFECT PCS
- loss of consciousness
- anterograde/retrograde amnesia
- delayed removal from sports participation
post-injury risk factors
AFFECT PCS
- migraine
- dizziness
- headache
- depressive symptoms (mindset)
- psychosocial factors (perceived competence, tenacity, tolerance of negative affect, and positive acceptance of change)
- early concussive management strategies
(strict rest vs relative rest vs active rehab)
red flags, review symptoms, determine if +/- concussion
What are the 3 steps in PT screening of a concussion?
red flags
SCREENING STEP 1
1. neuro signs
(pupillary asymmetry, declined mental status, repeated vomiting, severely worsening headache)
2. cervical injury
(vertebral artery dissection, fracture, ligamentous instability)
arterial, venous
An epidural hematoma is an ______________ injury, while a subdural hematoma is a ______________ injury.
head shape deformity
What is the primary sign of a skull fracture?
review symptoms
SCREENING STEP 2
1. physical
- headache, nausea, vomiting, balance problems, dizziness, visual problems, fatigue, sensitivity to light and noise, numbness/tingling, dazed or stunned
2. cognitive
- mental "fog", feeling slowed down, difficulty concentrating/remembering, forgetful of recent information or conversations, confused about recent events, answers questions slowly, repeats questions
3. emotional
- irritability, sadness, more emotional, nervousness
4. sleep
- drowsiness, sleeping less than usual, trouble falling asleep
determine +/- concussion
SCREENING STEP 3
diagnosis--> triangulation of data
- Pt/family/witness
- medical history
- observation/exam
- symptom checklist
"intake interview" = history
IMPAIRMENTS:
- MSX
- vestibulo
- autonomic dysfunction/exertional intolerance
- motor function
MSX (cervical), vestibulo-occular, vestibular, autonomic dysfunction, motor function (postural control0
What are the 4 concussion trajectories?
PT exam subjective (concussion)
1. cervical (and thoracic)
- neck pain, headache, dizziness, fatigue, balance problems, difficulty focusing on a visual target
2. vestibular/ocular
dizziness, HA, vertigo, nausea, fatigue, balance problems, visual motion sensitivity, blurred vision, difficulty focusing on stable or moving targets
3. autonomic dysfunction
- exertional intolerance, dizziness, HA, desire to return to high-level exertional activities
4. motor function (postural control)
- feeling off balance, recent falls
contextual factors
PSYCHOLOGICAL/SOCIOLOGICAL FACTORS:
- self-efficacy
- self-management
- expression and demonstration of good, healthy coping strategies in response to stressful situations
- type of support system
- number of potential risk factors
- understanding and attitude toward recovery
- access to resources and equipment that may facilitate recovery
*IMPACT PROGNOSIS
PT exam objective (concussion)
1. cervical (and thoracic)
- ROM, strength and endurance (cervical spine ms), palpation, joint mobility, joint position error test
2. vestibular/ocular
- VOMS
- ocular alignment (cross cover)
- head impulse testing
- positional testing (BPPV)
3. autonomic dysfunction
- orthostatic hypotension (HR & BP in supine, sit, and stand)
- graded exertional test
(TM, bike, marching)
4. motor function (postural control)
- static/dynamic balance
- motor coordination and control
- dual task
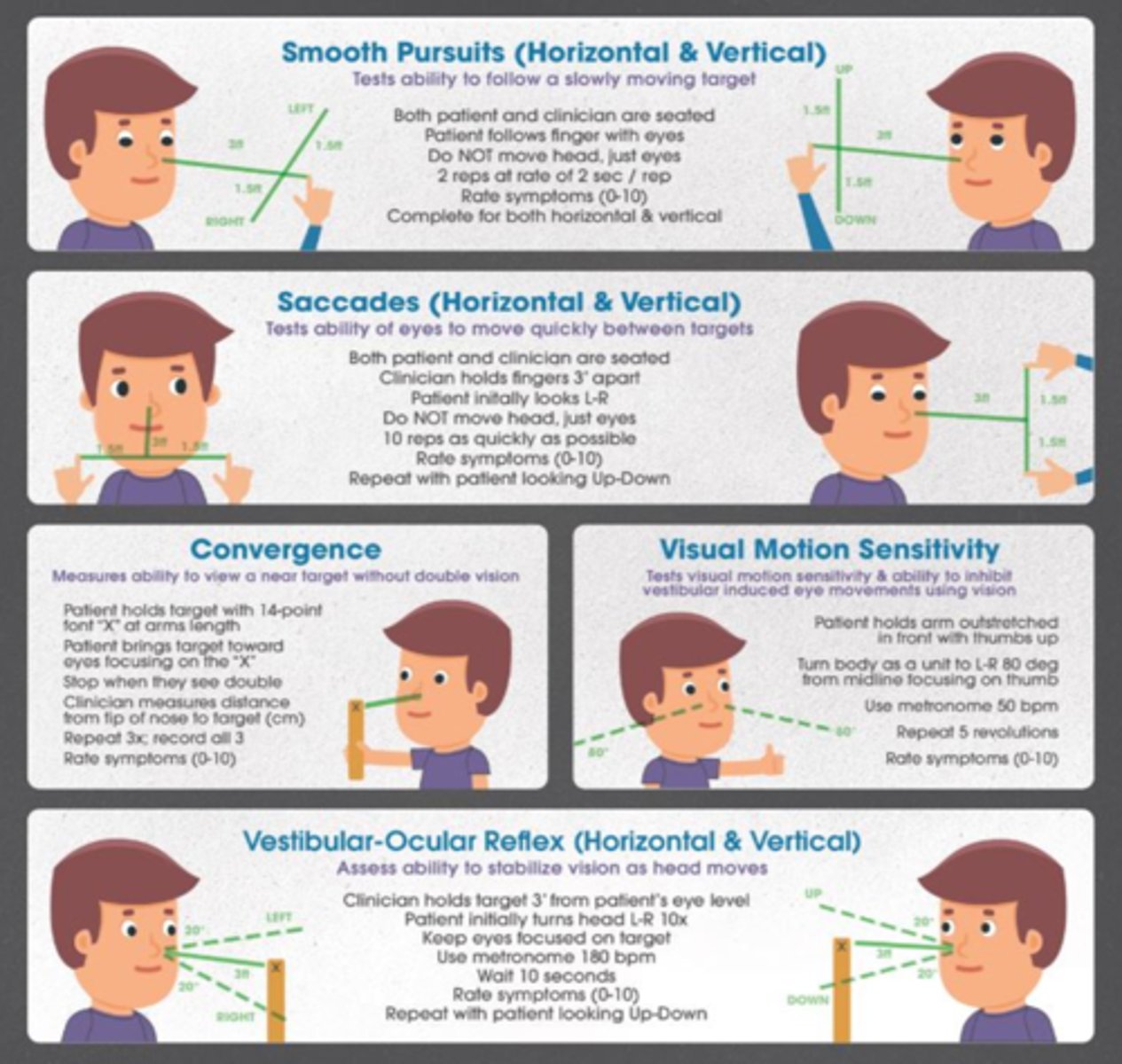
VOMS (vestibular ocular motor screening)
testing that allows clinicians to identify individuals who require additional specialized vestibular and ocular motor testing and therapy early in the recovery process, which may expedite their recovery
concussion outcome measures
- vestibular --> Dizziness Handicap Inventory
- CPG core set
(caution: ceiling effect)
- HIMAT
- computerized postural control assessment (Biodex)
- dual tasking
(TUG manual/cognitive)
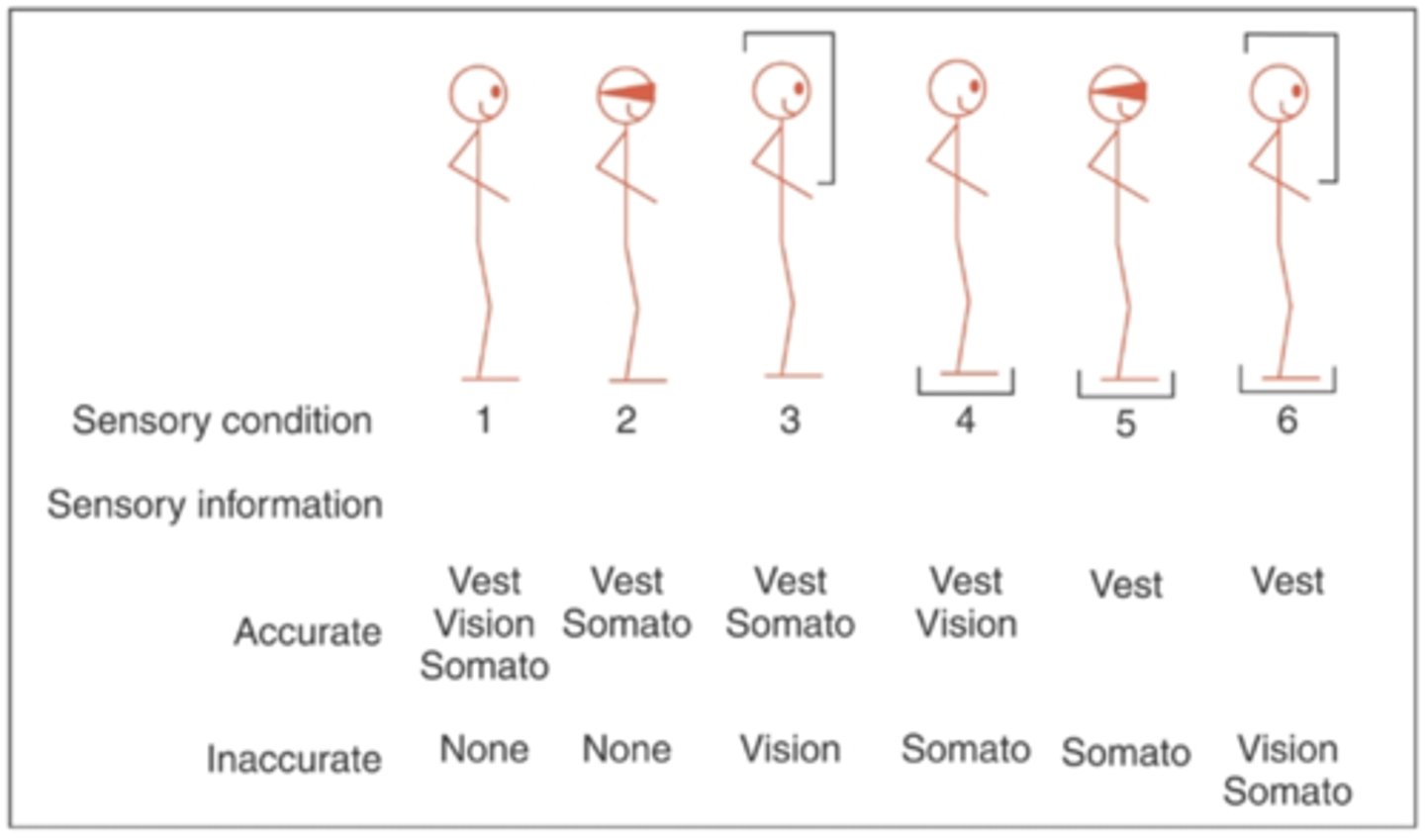
CTSIB
balance test
*can be computerized using biodex
QUANTIFIES:
- time
- sway
PT interventions
PATIENT EDUCATION
- self management strategies
- importance of relative rest
(after 24-48 hrs initial rest, active rehab)
- avoid activities that have a high risk for another concussion
- importance of sleep, safe return to activity, pacing strategies, diet
diet
our cells need proper fuel
AVOID:
- alcohol
- caffeine
- processed food
- sugar
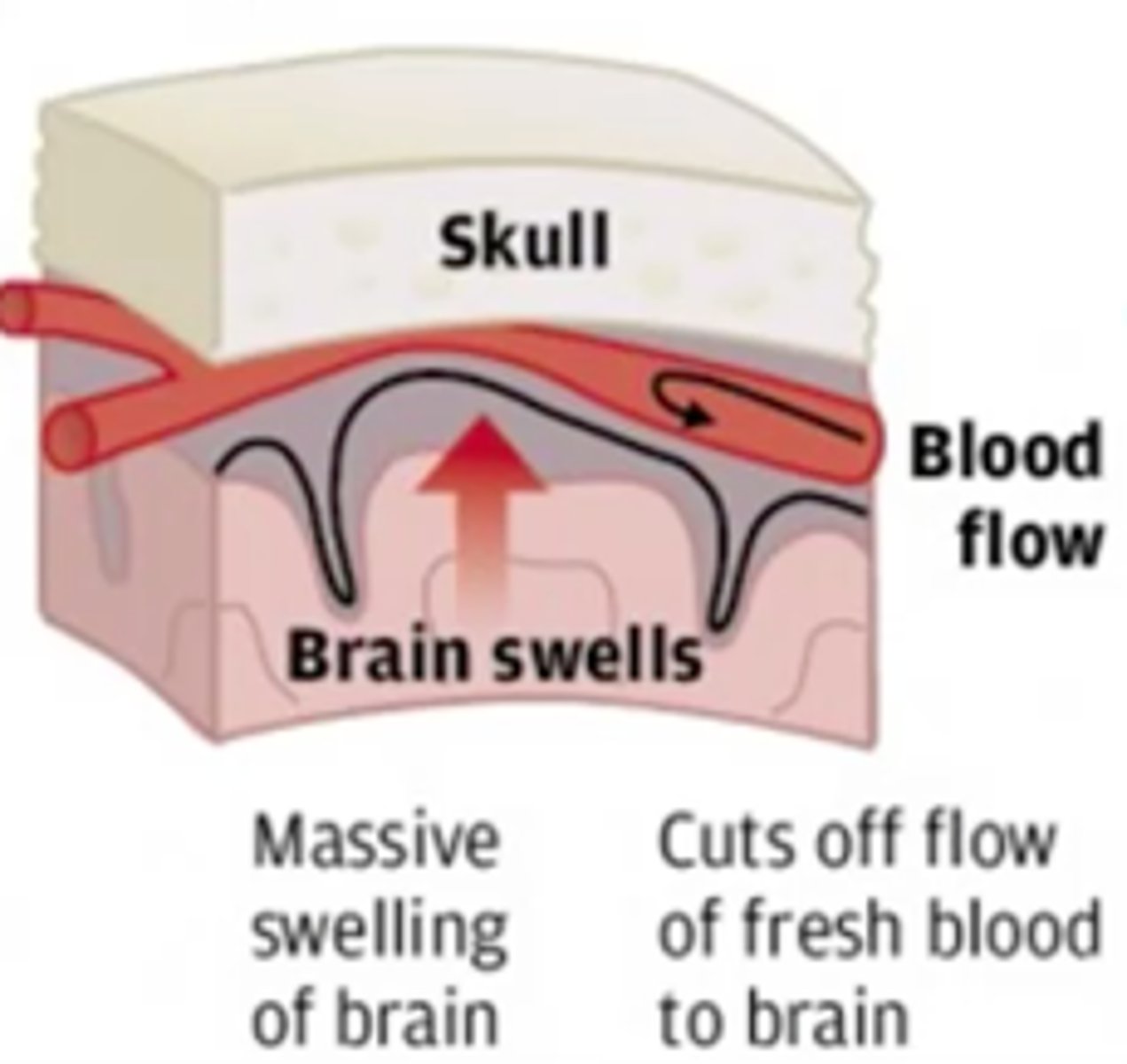
second impact syndrome
exponential increase in symptoms from a concussion following the immature return of an athlete back into competition prior to symptoms being resolved
*brain may swell/herniate which can result in death
return to learn
Should "return to play" or "return to learn" occur first in the sub-acute management of a concussion?
PT interventions for cervical concussion (and thoracic spine)
- ROM
- strength and endurance (cervical spine ms)
- posture position
- cericocephalic kinesthesia
- head position control
- manual therapy

reassessment (ROM, pain, symptoms, etc.)
What is the primary method of monitoring/progression of the cervical spine?
HINT: age appropriate symptom checklist to monitor symptoms
PT interventions for vestibular/ocular concussion
- adaptation/substitution
- habituation
- CRT (BPPV)
- convergence--> Brock string

PT interventions for autonomic dysfunction concussion
- symptom guided progressive aerobic exercise training program
*good for ALL concussion types as aerobic exercise promotes brain healing and mental health

PT interventions for motor function concussion
- static dynamic balance
- motor coordination
- dual task
qualitative assessment of patient's ability to self-management and PT recommendations
What should be completed during EACH VISIT when seeing a patient for a concussion?
age appropriate symptom checklist to monitor symptoms
What should be completed WEEKLY when seeing a patient for a concussion?
neurophysiological testing
ImPACT, C3 logic, Axon
common domains: visual memory, verbal memory, processing speed, reaction time
PERFORMED:
- when symptomatic to assist w/ return to school decisions
- when asymptomatic to assist with return to play decisions
compare post concussive performance to baseline if available or age norms if baseline unavailable
prevention
- mouthguard use should be supported in child and adolescent ice hockey
- policy disallowing body checking should be supported for all children and most levels of adolescent ice hockey
- strategies limiting contact practice in American football should inform related policies and recommendations for all levels
- neuromuscular training warmup programs are recommended
- policy supporting optimal concussion management strategies to reduce recurrent concussion rates is recommended