MOOD DISORDERS (unipolar/depression, and bipolar) AND SUICIDE (ch 5)
1/61
Earn XP
Description and Tags
washu psychopathology and mental health chapter 5 of psych texbook
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
62 Terms
terms for depression
depression, major depressive disorder (MDD), unipolar depression
DSM-V criteria for a major depressive disorder
must meet at least 5 of the following during the same 2-week period. at least one must be 1) depressed mood or (2) loss of interest or pleasure (anhedonia)
depressed mood most of the day, nearly every day, as indicated by self report of observations made by others — NOTE (in children or adolescents an be irritable mood)
markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day
significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day. (a change of more than 5% of body weight in a month)
insomnia or hypersomnia nearly every day
psychomotor agitation or retardation nearly every day (observable by others)
fatigue or loss of energy nearly every day
feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day
diminished ability to think or concentrate, or indecisiveness, nearly every day
recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or suicide attempt or a specific plan for committing suicide
major depressive disorder criteria:
at least one major depressive episode
no manic or unequivocal hypomanic episodes
dysthymic disorder
low level mood for an extended period of time:
depressed mood for at least 2 years
never without these symptoms for more than 2 months within this 2-year period
no major depressive episode during the first 2 years
lifetime prevalence = 3%
lifetime prevalence of dysthymic disorder
3%
premenstrual dysphoric disorder (PMDD) — new DSM-5 diagnosis
for most menstrual cycles over the past year; 5 or more symptoms present during luteal phase that begin to remit following menses
prolonged grief disorder — new DSM-5 diagnosis
continued presence, for at least 12 months after the death of a loved one, of impairing symptoms associated w grief
unspecified mood disorder — new DSM-5 diagnosis
a residual category for presentations of mood symptoms that don’t meet full criteria for any of the disorders in either the bipolar of the depressive disorders diagnostic classes
depression and additional mood disorder specifiers: “with psychotic features”
depression w psychotic features = hallucinations or delusions; mood congruent; only happens during depressive episodes
depression and additional mood disorder specifiers: “chronic major depressive disorder”
depression that does not remit for > 2 years
depression and additional mood disorder specifiers: “seasonal affective disorder”
recurrent episodes with a seasonal pattern
common pattern = when days get shorter / less light —> more depression
depression epidemiology:
lifetime prevalence of MDD = 16-17%
16-17 year olds (adolescents) have the highest rate of MDD
major depression is the leading cause of disability (10%)
age onset = adolescence and young adulthood
earlier onset = more severe
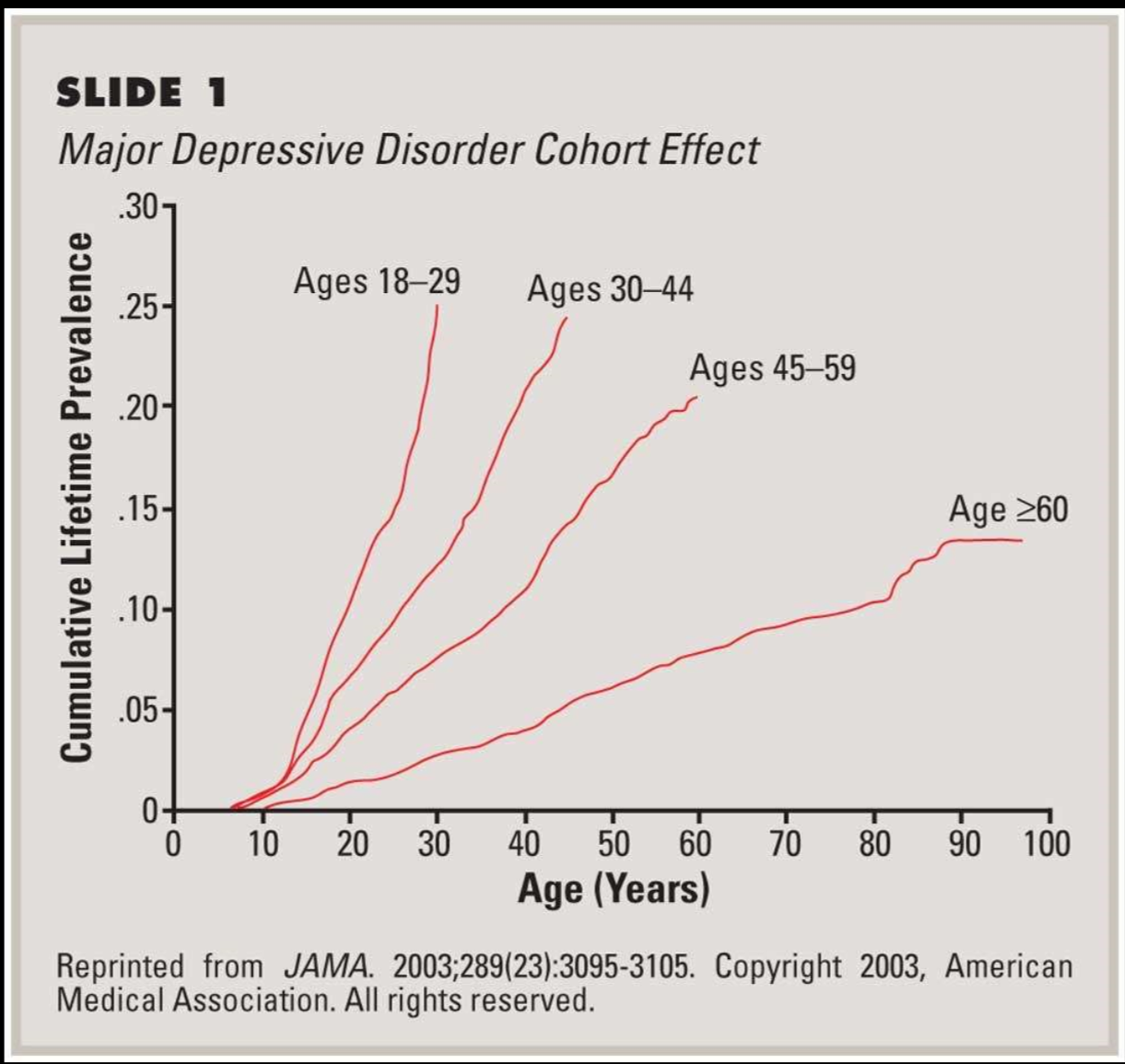
birth cohort trend for depression
prevalence is much higher in recent generations
why? we dont know. maybe awareness, technology, etc?
gender and depression
MDD: 2x as common in women relative to men
why?
women more liekly to present at health clinics, disclose feelings, seek treatment
men more likely to deal w in more externalizing ways (ex alcohol use). women externalize ore
rumination vs distraction
depression across cultures
universal phenomenon, but each culture expresses differently
ex: china and japan: more likely to be described in terms of somatic complaints (sleeping problems, headaches, loss of energy, stomach issues)
depression recovery
remission = period of recovery
full remission = at least 2 months with no significant depressive symptoms
partial remission = some symptoms, but no longer meet full criteria
relapse = return of active symptoms
statistic: 50% recover in 6 months
depression environmental factors
stressful life events
lack of social support
chronic stress
depression biological factors
HPA axis
genetic vulnerability
brain function
neurochemicals
depression psychological factors
information processing bias
cognitive distortions
rumination
personality / temperament
effects of uncontrollable stress on rats — depression study
induces a condition that resembles depression
depletion of: norepinephrine, serotonin, dopamine
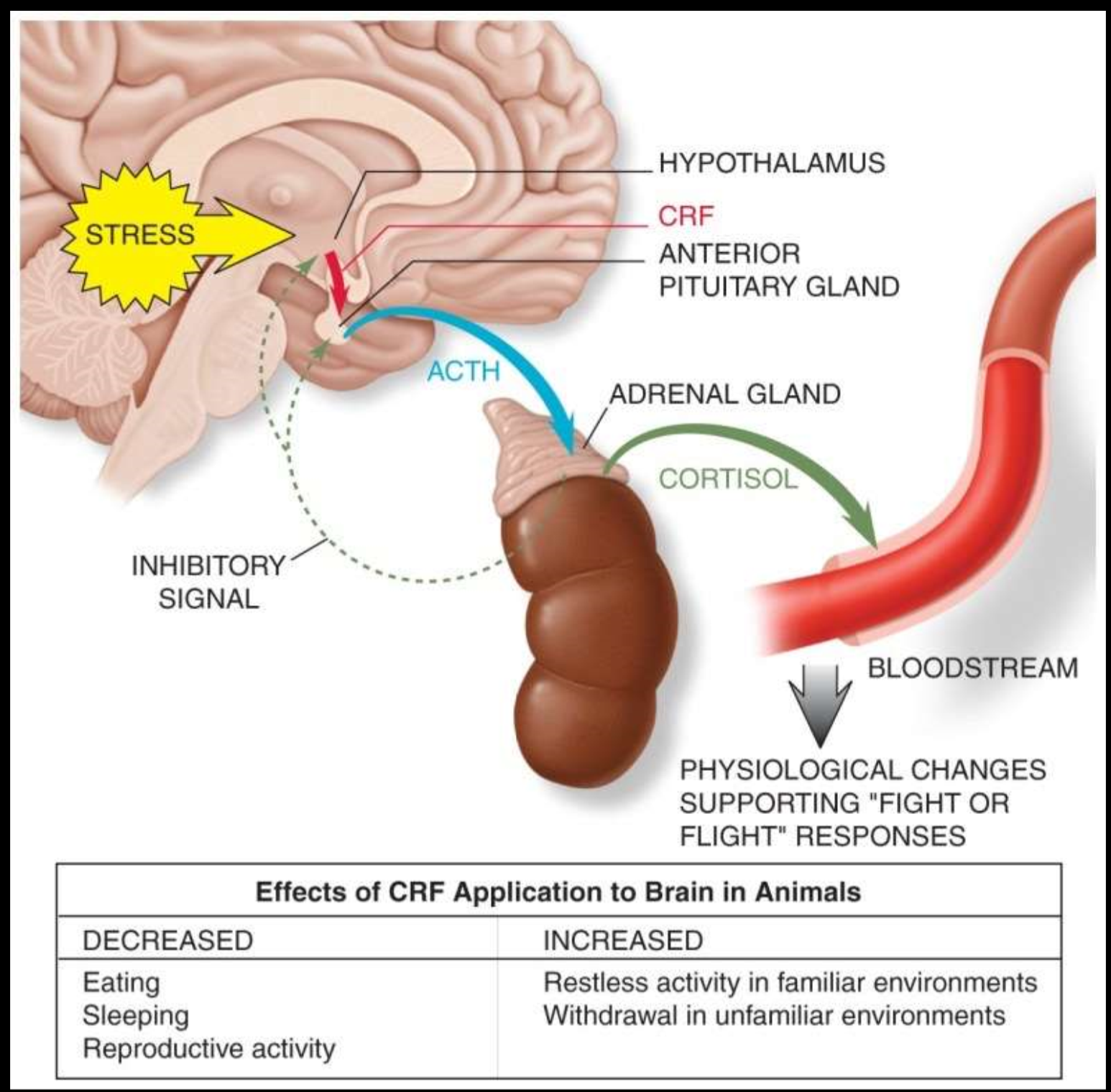
HPA axis: hypothalamic pituitary adrenal axis
individuals with depression: release a lot more CRF (corticotropin releasing factor) from their hypothalamus which stimulates more cotricotropin release form anterior pituitary which stimulates more cortisol release from adrenal cortex.
cortisol released into bloodstream and supports fight or flight responses.
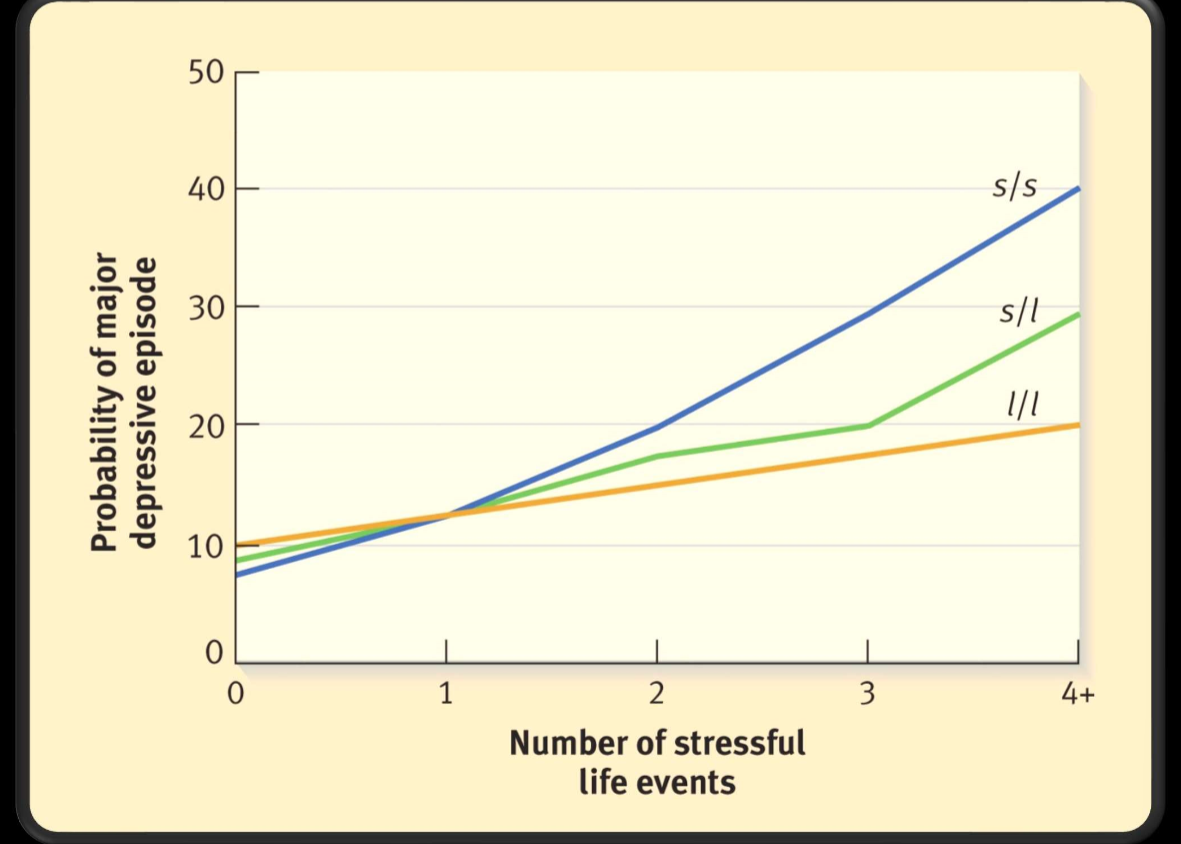
gene x environment interaction in depression
serotonin transporter gene = 5HTTLPR
short (s) allele = associated w increased risk of depression
long (l) allele not associated
homozygous for short allele at greatest risk for depression, especially if experience high stress event
twin studies: 30% increase with severity
1/3 of risk is attributed to genetics
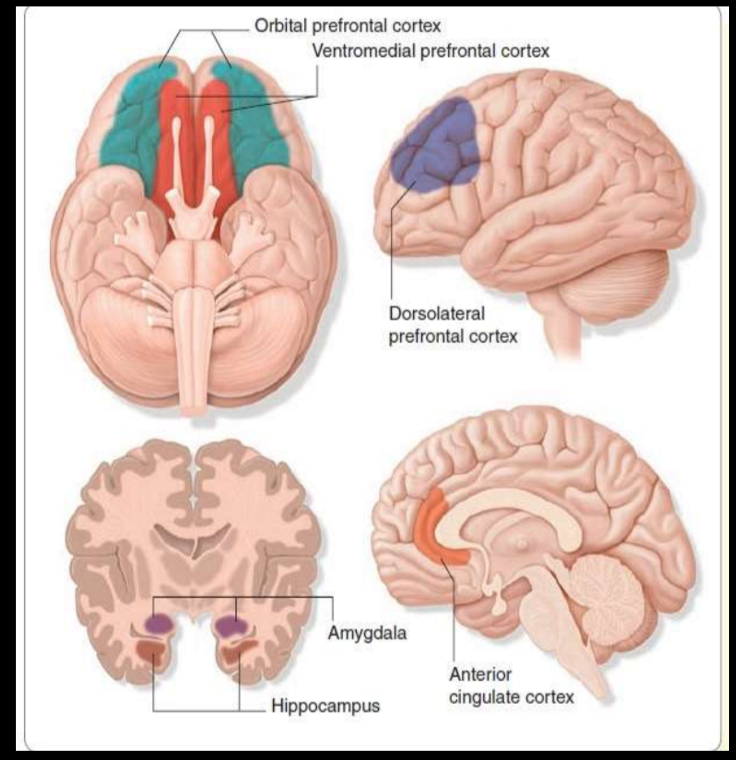
brain regions associated with depression
decreased functioning of:
orbital frontal cortex (OFC): related to reward functioning and how we respond to
ventral striatum: decision making functions and motor control
dorsolateral prefrontal cortex: cognitive control
Anterior cingulate cortex: selective attention
hippocampus (volume): learning and memory
increased functioning of:
amygdala: emotion and threat, fear
depression and reward
depressed individuals reacted less to both penalties and reward stimulus when compared to a normal control group. Shows reward center hypoactivation.
cognitive vulnerability to depression — why some individuals become depressed after stressful life events and some do not
pervasive and persistent negative thoughts about the self
pessimistic view of the environment
these thoughts are activated by the experience of negative life events
becks’ negative cognitive triad
triad of the self, the world, and the future
early negative life experiences —> formation of dysfunctional beliefs —> critical incidents —> beliefs activated —> negative automatic thoughts ←→ symptoms of depression
cognitive distortions (becks negative cognitive triad)
negative attribution style: internal, global, stable way of thinking ab the world; consistently views world in negative way or think that world views u in negative way
negative schemata: tend to view the world negatively and process info in negative ways as a result
rumination
negative automatic thoughts (Beck’s negative cognitive triad)
emerge automatically; rapid duration
not fully conscious
often occur in shorthand
not a result of deliberation, reasoning, or reflection
reflexive
difficult to turn off
validity is accepted without question
often precede a powerful emotion
treatment of depression
cognitive therapy / CBT
interpersonal therapy
behavioral activation treatement (CBT)
antidepressant medication
SSRI
SNRI
MAOI
TCA
alternative treatments
ketamine / psilocybin
deep brain stimulation
electroconvulsive therapy (ECT)
transcranial magnetic stimulation (TMS) — prelim data shows that increasing prefrontal cortex activity can help w depression. however TMS doesn’t reach deep brain structures well like ECT
bright light therapy for SAD — shown to be just as affective as fluoxetine
cognitive therapy for depression
focuses on identifying and replacing self-defeating thoughts with rational statements
deal w current experiences
effective for unipolar depression
interpersonal therapy for depression
focus on current relationships and attempts to improve these relationships via building communication and problem solving skills
idea: improved support system may improve depressive symptoms
behavioral activation treatment for depression
plan positive activities; force individual to get up and go
for indivs. who are severely depressed, just do one thing a week (ex. get out of bed and take a shower)
works very well with meds. not as affective without combination w meds tho.
four classes of antidepressant medication
SSRI: selective serotonin reuptake inhibitor (** current pref method)
SNRI: serotonin and norepinephrine reuptake inhibitor
MAOI: monamine oxidase inhibitors
inhibit enzymes that break down serotonin and norepinephrine
TCA: tricyclic antidepressants
inhibit norepinephrine reuptake (also serotonin tho lesser)
SSRI specifics
positive response: 50% or larger reduction of symptoms
remission: complete and sustained recovery
50% of patients show a pos response following 3-5 wks of treatment
prozac, paxil, zoloft
(also used for anxiety, OCD, bulimia, borderline personality disorder)
issues: nausea, insomnia, sexual problems
suicide relation to mental disorders
vast majority of ppl w mental disorders do not die by suicide
sociodemographic characteristics and stressful life events better predictors of suicide than mental disorders
risk factors: ppl experience crises, violence, abuse, loss, or isolation. also vulnerable groups that experience discrimination; refugees
at least 50% of suicides occur in the context of clinical depression
15-20% of depressed patients eventually commit suicide
many other disorders (schizophrenia, alcoholism) associated w higher suicide risk
active vs passive suicidal ideation
active: “I want to kill myself”
passive: “I don’t want to be alive. It would be better if I wasn’t here”
epidemiology of suicide
suicide rate: 12/100,000
highest completion rate: white men over 50
suicide rate increasing for: adolescents
between 1960 and 1980, completion rate tripled for males 15-24 (doubled for females)
suicide attempts vs completions statistics
in general: attempts to completions ratio = 10:1
among adolescents = 100:1
ages 15-19: females make 3 times as many attempts
male attempts use more lethal/destructive methods
Durkheim’s classifications: the 4 types of suicides
egotistic: individuals feel alienated and lost
altruistic: sacrifice for society (“im a burden, im doing this for others”)
anomic: breakdown of social order (“society is falling apart. this is my reaction”)
fatalistic: unbearable life circumstances (“life is unbearable, this is the only solution”)
Schneidman’s common elements of suicide
purpose: to seek a solution
goal: cessation of consciousness
Cognitive state: ambivalence
Perceptual state: constriction
Interpersonal act: communication of intention
Not always the case, especially for adolescents. Often an impulsive component
Pattern: consistency of lifelong styles
psychosocial factors associated with suicide
impulsivity
one of the main predictors of a suicide attempt. strongly associated w increased attempts compared to ideation
aggression
pessimism
family psychopathology or instability
genetics
sociocultural factors
prevalence of suicidal ideation
24% of high school girls and 15% of high school boys have serious suicidal thoughts
suicidal thoughts especially common amongst depressed adolescents
warning signs for student suicide
depressed and withdrawn
lowered self esteem
deterioration of personal hygiene
loss of interest in studies
communication of distress
students who have completed suicide attempts:
tend to be doing well in school
have low self esteem if academics are involved
have compromised interpersonal relationships
some significant life event / stressor
predictors of suicidal ideation in students: sex specific effects
men and women:
felt depressed and hopeless during the last year
men specifically:
experienced assault in the last year
women:
30 days of alcohol consumption
sexually assaulted
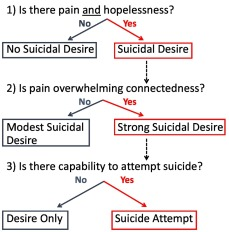
Klonsky’s Framework: From ideation to action (suicide)
two stages of suicide: ideation, attempts
different explanations for the two stages
pain, connectedness, and means
only when your have significant pain, significant loss of connectedness, and the means to do so, do you go from ideation to attempt
most people (~40%) with suicide ideation do not attempt
things that predict ideation do not always predict attempts
Thomas Joiner’s approach to suicide:
“perceived burdensomeness”
“thwarted belongingness” (social isolation)
acquired ability to inflict lethal self injury
mood disorder
an umbrella term that encompasses unipolar and bipolar disorders
disorders made up of episodes:
depressive episodes
manic episodes
hypomanic episodes
mixed episodes
mood disorders are made up of episodes
depressive episodes
manic episodes
hypomanic episodes
mixed episodes
the manic-depressive spectrum
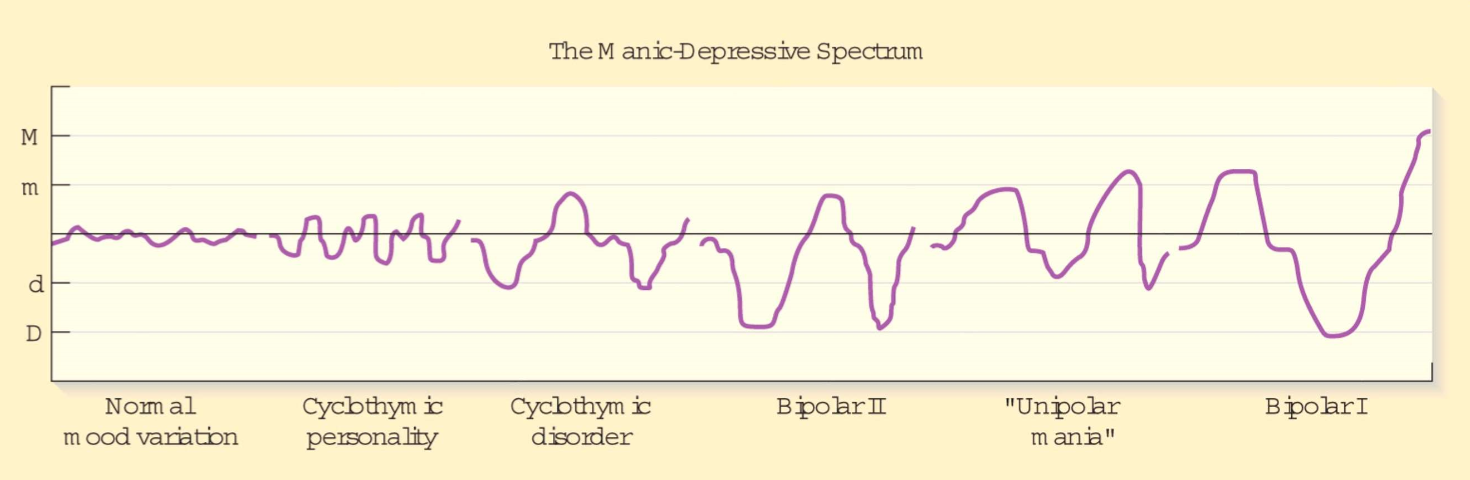
bipolar I criteria
at least one full manic (or mixed) episode
bipolar II criteria
at least one major depressive episode
at least one hypomanic episode
no manic episodes
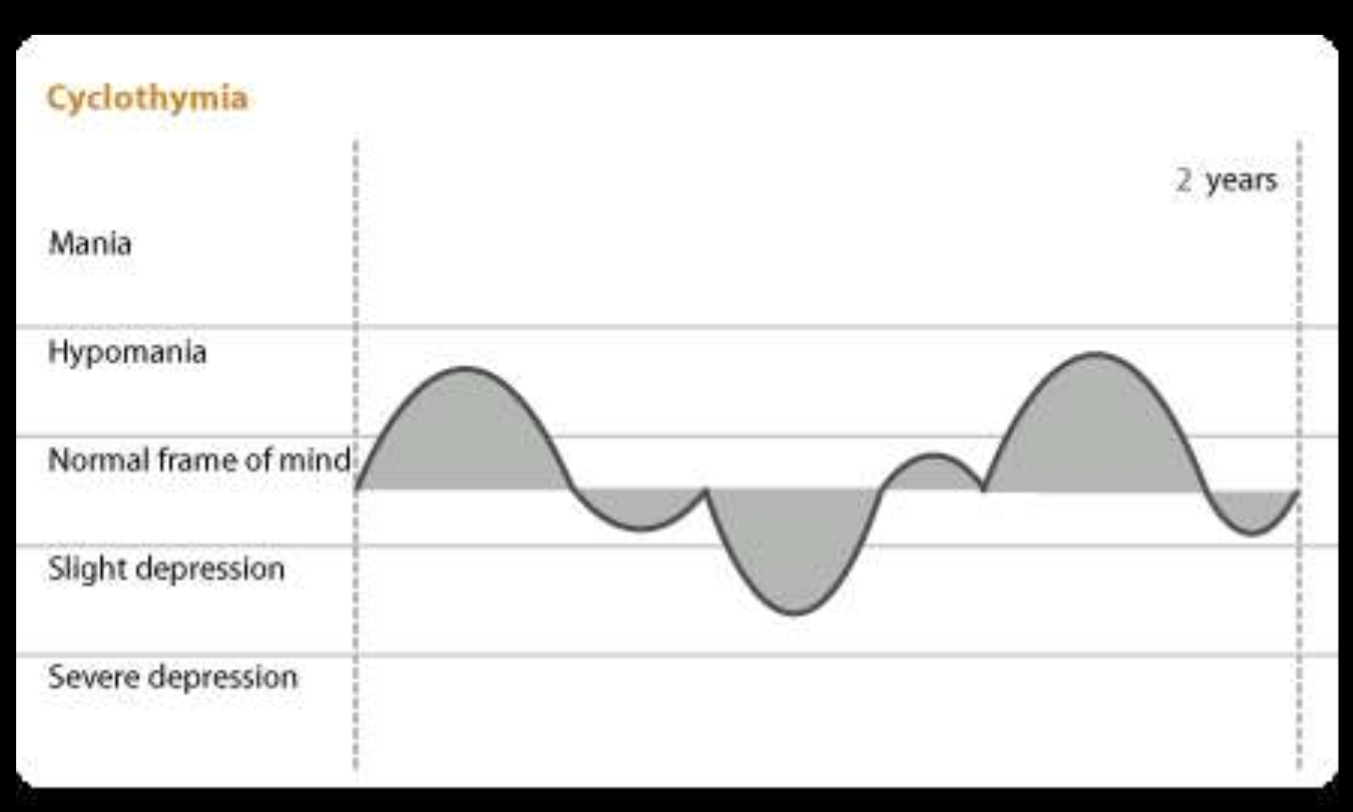
cyclothymia / cyclothymic disordercriteria
no manic or major depressive episodes for at least 2 years
rapid fluctuations in mood, but minor fluctuations (never the extremes of full manic or depressive episode)
lacks severe symptoms and psychotic features of bipolar
much less prevalent
criteria for a manic episode
a period of elevated, expansive, or irritable mood
lasts at least a week
at least 3 of the following: DIG FAST mnemonic
Distractibility
Irresponsibility / irritability — excessive risky pleasure seeking
Grandiosity
Flight of ideas
Activity — goal directed / agitation
Sleep decreased
Talkativeness — disorganized
characterized by significant distress or impairment
often some psychotic symptoms — most often grandiosity
prevalence of mood disorders
depression = 16-17%
dysthymia = ~3%
bipolar = ~4%
bipolar I less prevalent than bipolar II
cyclothymia = ~1%
epidemiology of bipolar disorder
occurs equally btwn males and females
age of onset: 22 years old avg. ( adolescence or young adulthood )
days depressed vs days manic: 3 times as many days are depressed as are manic/hypomanic
unipolar vs bipolar comparison
Unipolar:
Later onset
More prevalent in women
Responds to psychotherapy alone, tricyclic or SSRI antidepressant drugs alone, or combination
Bipolar:
Earlier onset
Equal prevalence among men and women
Responds best to lithium carbonate or other mood stabilizers; does NOT respond to psychotherapy alone
environmental risk factors — bipolar disorder
Stressful life events (HPA axis alteration)
Goal attainment (high)
Schedule disruption
Very important risk factor for relapse.
Lack of sleep -- more unique to manic.
Not only are they sleeping less. During manic episodes, also say that they require less sleep
Also common that prior to the manic episode, they notice they are getting less sleep
biological risk factors — bipolar disorder
Genetic vulnerability
Bipolar is HIGHLY HERITABLE — even moreso than schizophrenia
Brain function
psychological factors — bipolar disorder
cognitive distortions
grandiose thinking
genetics and bipolar disorder
twin studies found bipolar to be highly heritable (High MZ concordance rates)
genome-wide association study (GWAS) finds CACNA1C gene snp associated with bipolar
gene codes for subunit of the L-type calcium channel involved in general action potentials. associated w increased rates of bipolar
brain function associated with bipolar (reward circuitry)
hypoactivation of reward circuit to small gains
hyperactivated amygdala: heightened emotional state → mania
hypoactivated hippocampus and prefrontal cortex: decrease in rational decision making
ppl w mania require more stimulation to get activation of their reward system (Right ventral striatum)
treatment of bipolar disorders
lithium:
effective for mania
40% do NOT improve
side effects that lead to → noncompliance
anticonvulsants:
tegretol, depakene
~50% respond
used for rapid cycling
less severe side effects (gastrointestinal)
psychotherapy:
can supplement medication
NOT effective alone
cognitive therapy
combo of psychotherapy and medication works better than medication alone!!