measuring vision and visual acuity
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
40 Terms
Explain the difference between vision and visual acuity
Vision is the smallest line of letters than can be seen before new refractive error (the optical prescription) is determined whereas visual acuity is the smallest line of letters that can be seen with the best possible refractive correction in place – after eye test
What is aided vision
vision measured with spectacles or contact lenses
what is unaided vision
vision measured without spectacles or contact lenses
what is habitual vision
the measurement taken when the patient is wearing their usual correction (glasses or contact lenses, if any) – varies depending on the patient
what is distance vision/VA
measured for optical infinity
clinically 6m is usually used/regarded as infinity
what is near vision/VA
measured for reading distance
usually around 40cm, but varies for each patient as it is measured at the point the patient carries out near tasks like reading/holding a phone
what is intermediate vision/VA
Around arms length
Typically considered for patients who use computers, read music etc.
Explain when we need to measure near, distance and intermediate vision
On an eye test we should measure vision in these different conditions/distances as vision may vary in each
For most patients near and distances, for some intermediate also depending on their needs
Why do we need to measure vision/VA (6)
1) legal requirement - Opticians Act (1989)
2) baseline data - provides a baseline recording, which can be used to compare to other data acquired afterwards if needed
3) diagnostic tool - to aid the examination and diagnosis of eye diseases/refractive errors - can demonstrate the need for glasses etc.
4) measure progression of a disease - assess changes in VA over time
5) evaluate treatment - assess if vision/VA has bettered or worsened after treatment
6) patient expectation
what is the MAR
minimum angle of resolution - smallest critical detail the patient is able to see to be able to differentiate between details
the ability to see details - critical details (C/O)
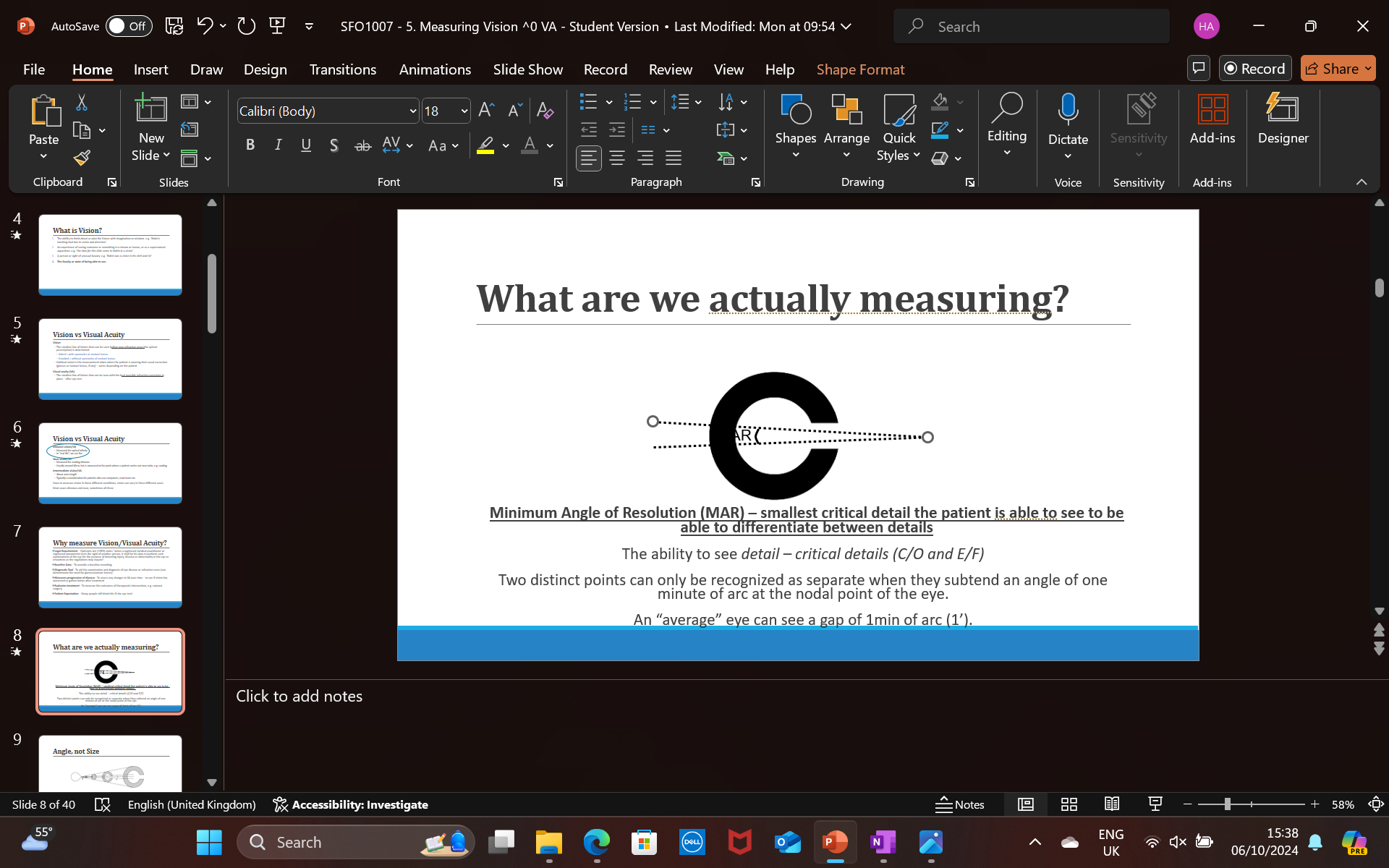
what is the MAR of an average eye
an average eye can see a gap of 1 min of arc (1’)
how many minutes of arc are there in one degree
60
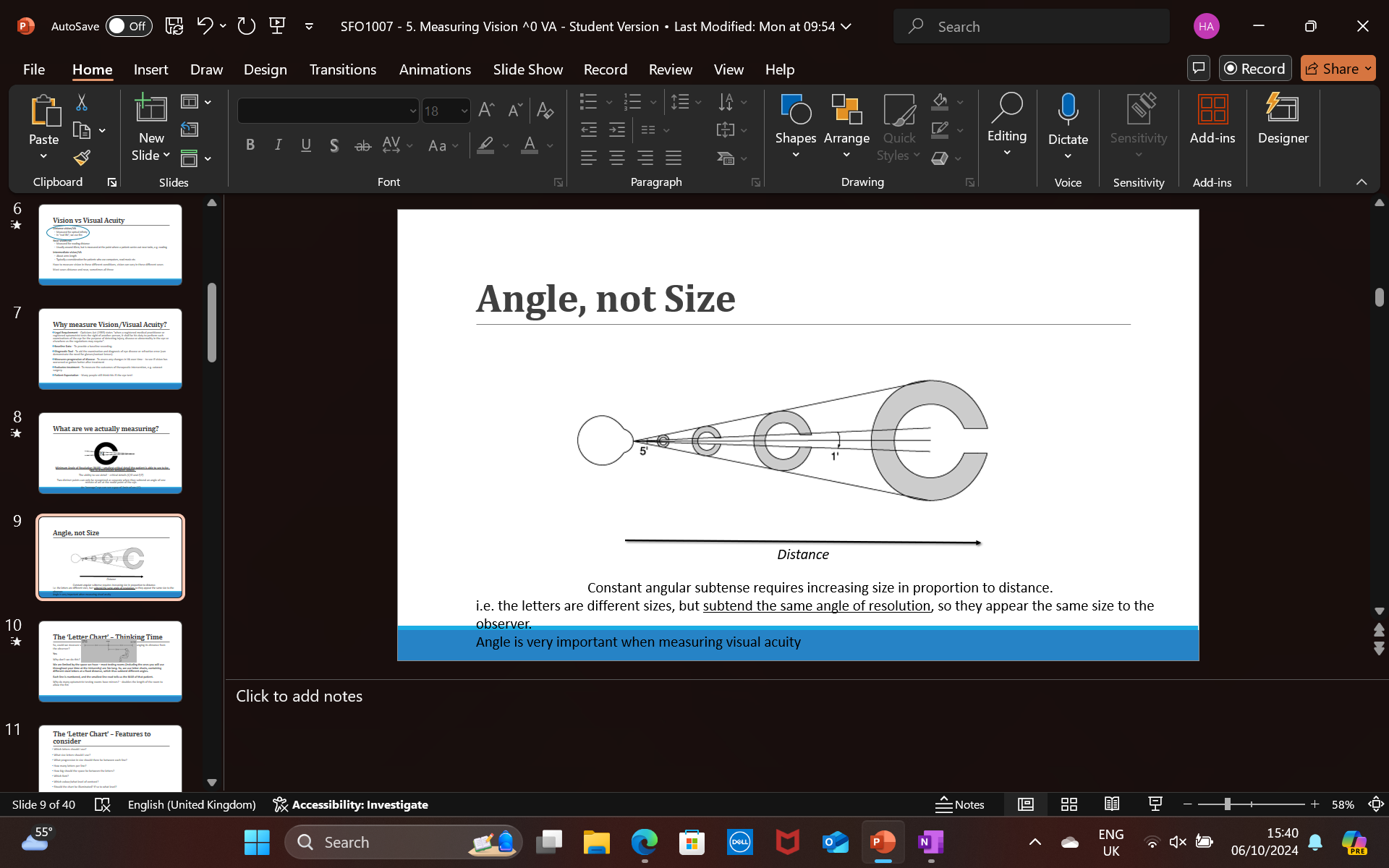
explain why angle is important when measuring visual acuity
Constant angular subtense requires increasing size in proportion to distance = i.e. the letters are different sizes, but subtend the same angle of resolution, so they appear the same size to the observer
If you double the distance between an object and an observer, you must double the size of the object, so it will have same angle and therefore look the same size to the patient
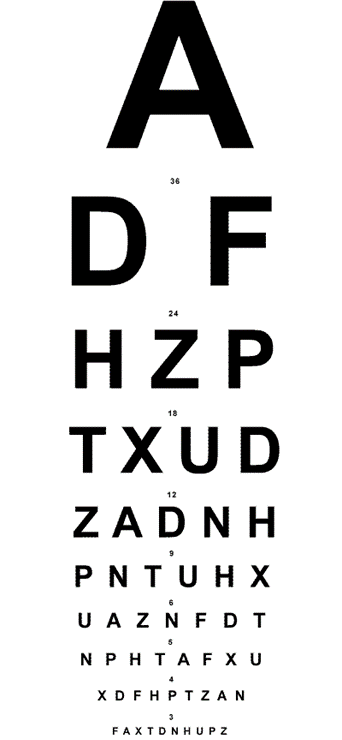
How do we clinically use the MAR to measure vision
we use letter charts, containing different sized letters at a fixed distance, which thus subtend different angles.
Each line is numbered, and the smallest line read tells us the MAR of that patient
could we measure vision by taking a letter of one fixed size and changing its distance from the observer?
Yes, however we are limited by space as most testing rooms are 3m long
why do optometrists use mirrors in their testing rooms
it doubles the length of the room to allow the 6m (to measure optical infinity - distance vision)
what are things to consider when making/using a letter chart (8)
which letters to use, size of the letters, font, colour, illumination of the screen, letters per line, space between each letter, space between each line
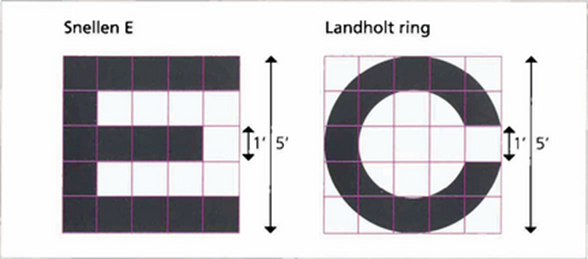
what is the snellen chart
a vision chart with letters constructed on a 5 x 5 grid so that the size of the critical detail (each gap width) subtended 1/5th of the overall height. He used letters which can easily be confused, e.g. C/O, N/H, P/F
what does snellen define standard vision as
the ability to recognize an optotype (a letter on the chart) when it subtends an angle of 5 minutes of arc (5’)
what is the Snellen fraction
= Testing distance (usually 6m) Distance at which optotype subtends an angle of 5’
numerator = 6 (or can be 3 depending on the room)
denominator = the number on the line of the letter chart of what the patient can read up to
how can we work out the MAR using the snellens fraction
reciprocal of the fraction
eg: the reciprocal of 6/12 is 12/6, 12/6 = 2
therefore the MAR is 2’
what is generally standard/average vision
6/6
explain the effect on vision when the denominator increases/decreases
the larger the denominator (6/12) the patients vision is worse than standard - 6/6
the smaller the denominator (6/4) the patient has better than standard vision - 6/6
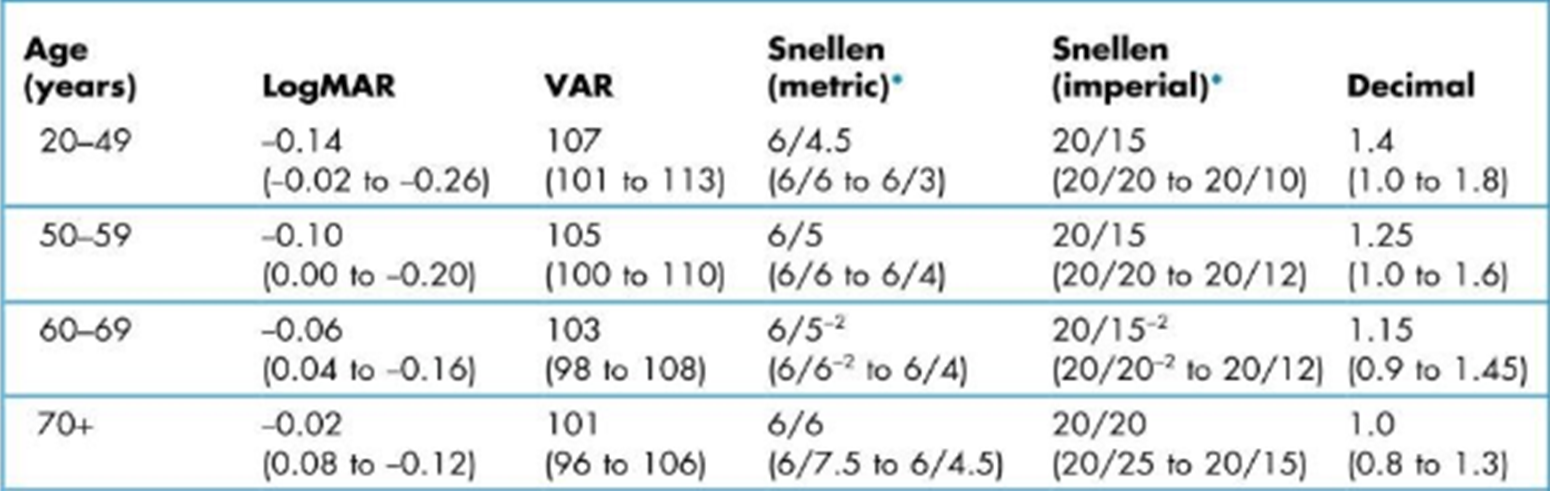
explain how age has an affect on standard vision
6/6 is typically considered “standard vision”, however - depends on age of patient
For an older patient 6/7.5 is seen to be standard vision as vision worsens with age even though the denimator is bigger than 6
For a younger patient 6/4.5 can be seen as standard vision
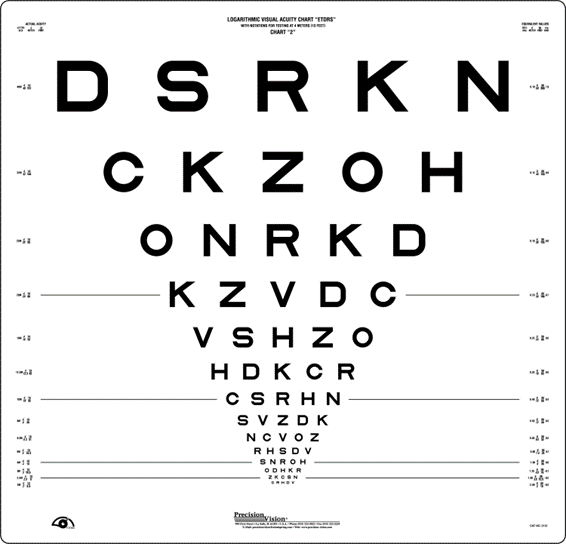
What is another letter chart that can be used instead of the Snellen chart
the Bailey-Lovie Log MAR chart
Advantages of the Snellen chart (3)
portable
commonly used and recognized
easy recording
disadvantages of the Snellen chart (4)
different number of letters on each line so easier for patient to guess the first letter
unequal size progression per line
less repeatable than LogMAR
1/3 less sensitive than LogMAR to interocular differences in vision – between right and left eye
advantages of the Bailey-lovie LogMAR chart (6)
same number of letters on each line
even line spacing and crowding
more repeatable than Snellen
standardized recording - easier to compare as letters scored individually
more sensitive to interocular differences than Snellen
Logarithmic progression - 0.1 steps
disadvantages of the LogMAR chart (3)
large - not portable
less commonly used, so less recognisable
recording can be tricky to initially interpret
explain the procedure of measuring vision/VA clinically (6)
ensure the chart is at an appropriate distance from the patient (6m), and the patient is seated comfortably
make sure room lights are on
gain verbal consent from patient for the test and explain the procedure clearly
cover one eye with occluder- hold it yourself and watch patient to make sure they do not cheat (memorize the chart so you can do this)
ask patient to read the smallest possible line they can - encourage and push them to read the smallest line as possible - make sure they do not squint or lean forward
record result for each eye and then both eyes
explain how to record the results if the patient reads less than half the line
record it as 6 / the line above + the number of letters they read from that line
eg: if they read the 6/12 line fully and only 2 letters from the 6/9 line
6/12 + 2
explain how to record the results if the patient reads more than half the line
record it as 6 / that line - the number of letters missed from that line
eg: if they read 6/12 line fully and 4 letters out of 6 from the 6/9 line
6/9 - 2
What should you do if the patient cannot see any of the letters
bring the chart closer to them, or move them closer to the chart
to 3m closer, then 2m, then 1m if necessary
remember to change numerator to 3/x rather than 6/x
what should you do if the patient cannot see the any of the letters even at 1m (3)
1.Count Fingers (CF) – measure the maximum distance at which the patient can count the number of fingers you are holding up. Record as CF@ ? cm
2.Hand Movements (HM) – measure the maximum distance at which the patient can see your hand moving. Record as HM @ ? cm
3.Light Perception (LP) – hold a pentorch 50cm away from the patient and ask if they can tell you when you turn the light on or off. If they can, record as LP. If they cannot, record as NLP (no light perception)
Explain the correlation between lighting, pupil size and vision
bright light causes the pupil to constrict, which can result in a better vision measurement than expected
dim light causes the pupils to dilate, which can result in a worse vision measurement than expected
how can we standardize lighting to ensure it does not affect vision measurement
British regulations are “normal room lighting” to simulate natural viewing conditions (between 80-320 lux
explain the use of a pinhole to measure VA
Used when VA is not 6/6
same procedure, but with pinhole in front of the eye when testing
recorded as PH 6/x
The pinhole reduces the amount of refractive blur (smaller blur circle on retina; the same effect as reducing the pupil size) and thus helps to distinguishes between refractive blur and disease.
If vision doesn’t improve through a pinhole, suspect disease
limitations of using letter charts to measure VA (3)
only measures central vision
only measures ability to see high contrast letters (doesnt test contrast sensitivity)
6m is not the same as optical infinity
explain the procedure to measure a patients near vision/VA (3)
explain procedure to patient and gain verbal consent to conduct the test
ensure lighting is similar to what the patient is used to when performing near tasks
offer the patient the reading chart and ask them to hold it to their preferred reading distance - measure and record this
explain monocular and binocular vision
monocular = vision in one eye
binocular = vision in both eyes