shock
a life-threatening condition where tissue perfusion is inadequate and cannot deliver oxygen and nutrients for cellular function
without treatment, poor delivery of oxygen and nutrients to cells leads to cellular hypoxia, cell death, organ dysfunction, and eventually total body shutdown or death
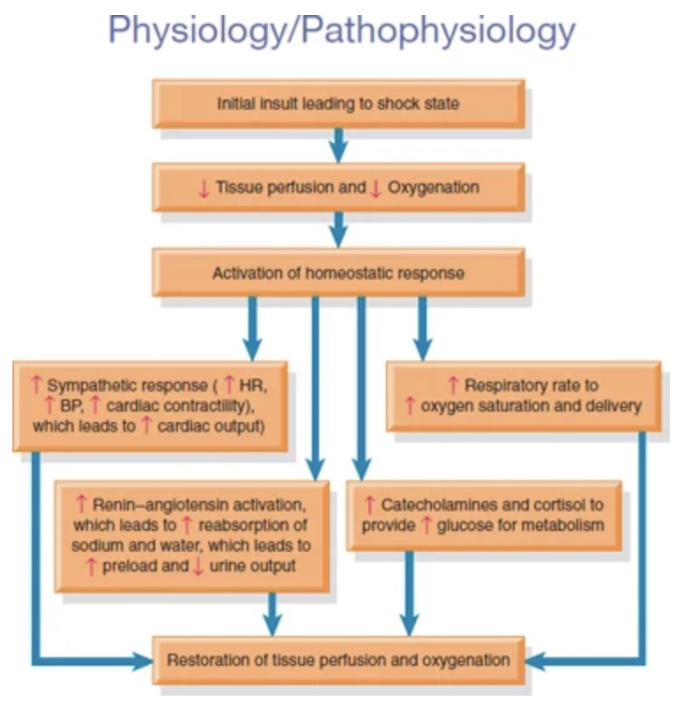
pathophysiology of shock
The initial insult that caused the shocked state
Decrease in tissue perfusion and the start of decreased oxygenation to tissues
Decreases start/spur the activation of the homeostatic response
Sympathetic response (fight or flight) is activated to increase cardiac output (including fresh O2 and nutrients to tissues) in order to compensate; to restore tissue perfusion and oxygenation, vitals increase
Renin-angiotensin activation hits the kidneys to:
Increase reabsorption of sodium and water
Increase preload (due to increase fluid)
Decrease urinary output
Increase in catecholamines and cortisol:
Responses to help the glucose in the anaerobic metabolism
risk factors contributing to shock
being on a disease state
age
Volume loss
Myocardial damage
Infection
Allergic reactions
Trauma to spinal cord
types of shock
hypovolemic shock
cardiogenic shock
distributive shock
septic shock
anaphylactic shock
neurogenic shock
hypovolemic shock
problem with the “tank”
Most common type of shock
Results from some sort of loss from the intravascular volume
Can be internal or external fluid loss
Loss 15-30% creating hypovolemic shock
External fluid loss = trauma, vomiting, diarrhea
Internal = internal bleeding into vasculature, burns (fluid shifted rapidly from intra to extracellular spaces and is displaced), ascites, dehydration
cardiogenic shock
problem with the “pump”
Shock state resulting from impairment or failure of the myocardium
Can be coronary in nature or not coronary
Coronary = direct damage to heart
Ex. myocardial infarction/heart attack
Noncoronary = condition happening somewhere else in the body and is affecting the heart
Ex. acidosis, hypoxemia, hypoglycemia, tension pneumothorax, pulmonary embolus
distributive shock
Problem with “pipes”
Blood is no longer in the right place and is out of the intravascular space and is in the periphery
Relative hypovolemia; related to pipes having problem, not necessarily fluid loss
septic shock
caused by overwhelming infection
Causes chemicals to be released, triggering an inflammation response
After inflamation, whole body dilates and fluid moves into periphery, without any pressure to move it back to the heart
anaphylactic shock
caused by allergen exposure
Massive antibody response causing vasodilation
Treated with epinephrine to reverse vasodilation
Commonly triggered by food , medication, insect stings, bites
neurogenic shock
caused by damage to the nervous system
Spinal cord injury, trauma
Sympathetic stimulation causes the smooth muscle to constrict while the parasympathetic tries to vasodilate
This cross/disruption causes the parasympathetic to take over and vasodilate to loos volume
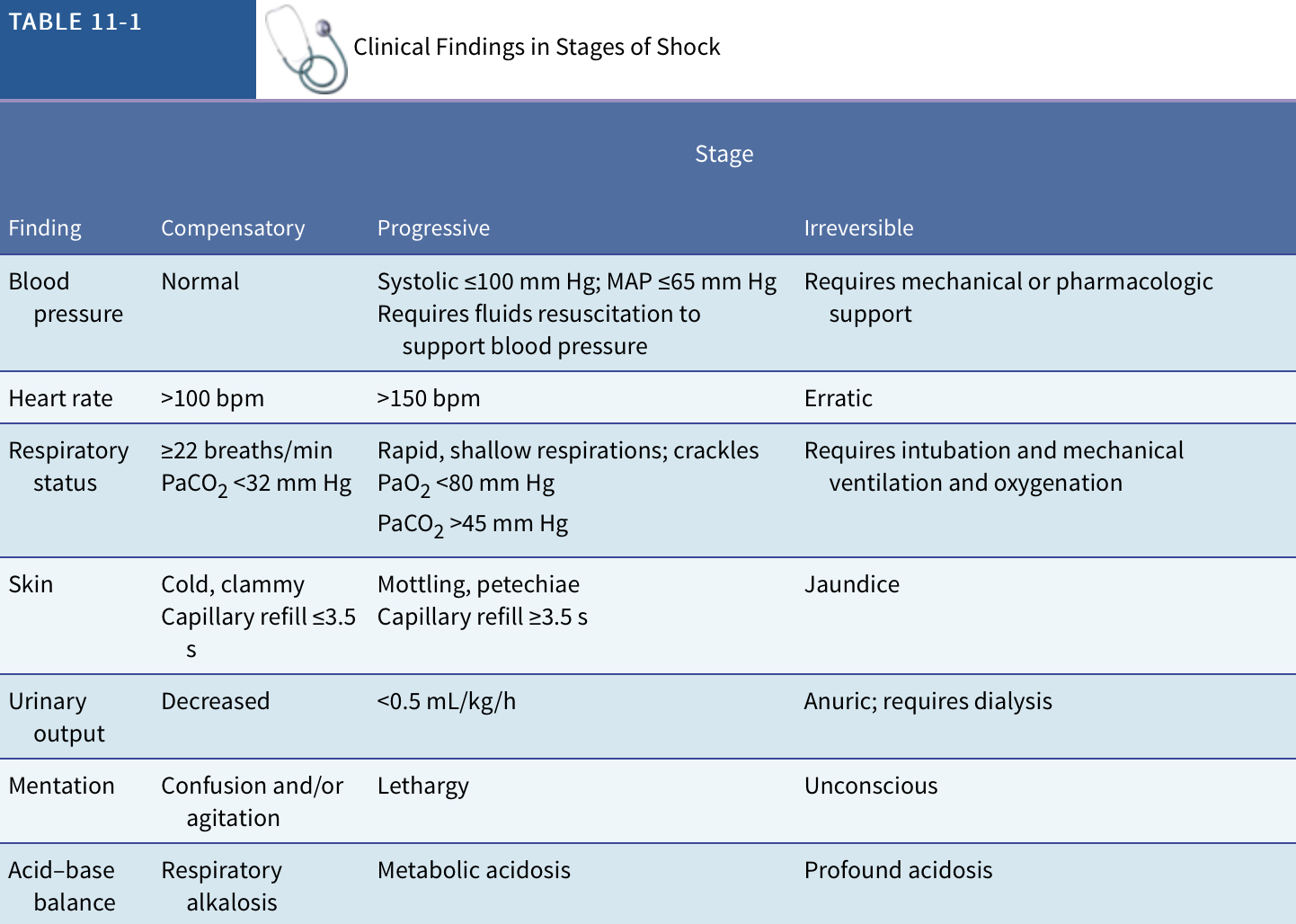
stages of shock
compensatory
progressive
irreversible
clinical manifestations of the compensatory stage of shock
The body automatically shunts blood AWAY from the nonvital organs in order to get the vital organs perfused
normal BP
tachycardia
tachypnea
cold clammy skin
decreased urinary output
clinical manifestations of the progressive state of shock
hypotension
MAP <60 mmHg
tachycardia
rapid, shallow breathing
pulmonary edema; fluid accumulation in lungs
Petechiae = dark red/purple rash due to hematological function impairment
clinical manifestations of the irreversible stage of shock
While pt. Is still being treated, the damage is not reversible
Organs have been damaged beyond repair
BP cannot be maintained
Oxygenation needs constant ventilatory support
MAP is not maintained
MODS = multiple organ dysfunction syndrom; all organs fail
Organ damage is too severe to respond to any treatment
Metabolic acidosis
Lactic acidosis
Complete depletion of energy stores
mean arterial blood pressure (MAP)
MAP is the best indicator of perfusion to vital organs
Average of arterial pressure during a single cardiac cycle
Normal range = 65-110 mmHg
mean arterial blood pressure equation
( 2 x diastolic pressure) + systolic pressure / 3
clinical manifestations of hypovolemic shock
Anxiety or agitation
Cool, clammy skin
Confusion
Decreased or no urine output
Generalized weakness
Pale skin color (pallor)
Rapid breathing
Sweating, moist skin
Unconsciousness (lack of responsiveness)
clinical manifestations of cardiogenic shock
Angina = chest pain
Arrhythmias = abnormal heart rhythm
Fatigue
Feeling of doom
EKG changes = electrical changes
Biochemical markers
Increased when damage or death to heart tissue
clinical manifestations of septic shock
Initial:
Hyperthermia
Tachycardia
Bounding pulse
Hypotension
Decreased urine output
Nausea, vomiting, decreased GI
Mental status changes
Later:
BP drop
Cool clammy
MODS
clinical manifestations of anaphylactic shock
occur 2-30 minutes after exposure to antigen
mild:
headache
lightheadedness
nausea, vomiting
pruitus
flushing
dyspnea
bronchospasm
cardiac arrhythmia
hypotension
severe
rapid hypotension
decreased consciousness
respiratory distress
cardiac arrest
associated priorities to treat shock
Figuring out what is the underlying cause of the shock
Fluid replacement
Respiratory support through oxygenation, ventilators, or more aggressive oxygen therapy
Nutritional support
Maintaining BP and tissue perfusion in order to check for mean arterial pressure (MAP)
Pain control
Morphine = pain control and vasodilator
usual treatments for shock
Giving supplemental oxygen
fluid support
vasoactive medications
nutritional support
positioning
modified trendelenberg for hypovolemic shock
nursing considerations for shock
monitor subtle changes in appearance, outputs, labs, EKG, etc.
advanced directives
older adult considerations
medications used to treat hypovolemic shock
Normal saline (0.9% NS)
Lactated ringers
Albumin
Blood
normal saline and lactated ringers
drug classification
Crystalloid = small, freely moving molecules able to move between intracellular and intravascular spaces
general indications
fluid replacement to get volume in but may move into third space due to small molecules
electrolyte balance
nursing implications
Over rescesutation
Extra fluid may affect other diagnoses’
Hypothermia
High volumes of fluid may be at room temperature but room temperature is still too cold for the body
drug classification
general indications
nursing implications