CNS Sleep pt 1
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
38 Terms
Categories of sleep disorders
- Insomnia Disorders
- Narcolepsy
-Breathing-Related Sleep Disorders
- Circadian Rhythm Disorders
- Restless Legs Syndrome
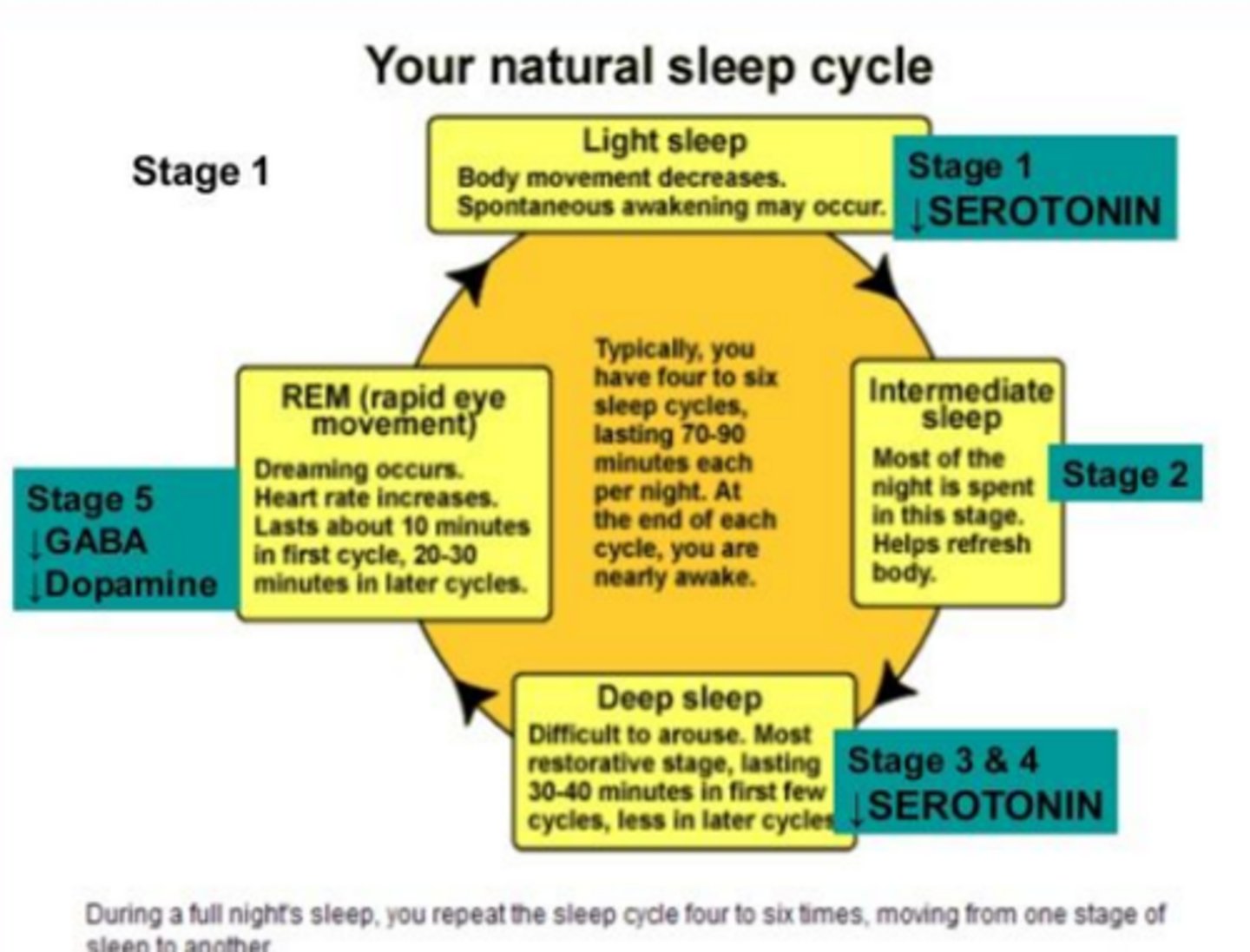
Sleep Cycles
- Non REM Sleep (75%)
- REM Sleep (25%)
Non REM sleep
- 4 stages
- 1&2: wakefulness / light sleep
- 3: delta sleep
- 3&4: metabolic activity and brain waves slow (deep sleep, no eye movement)
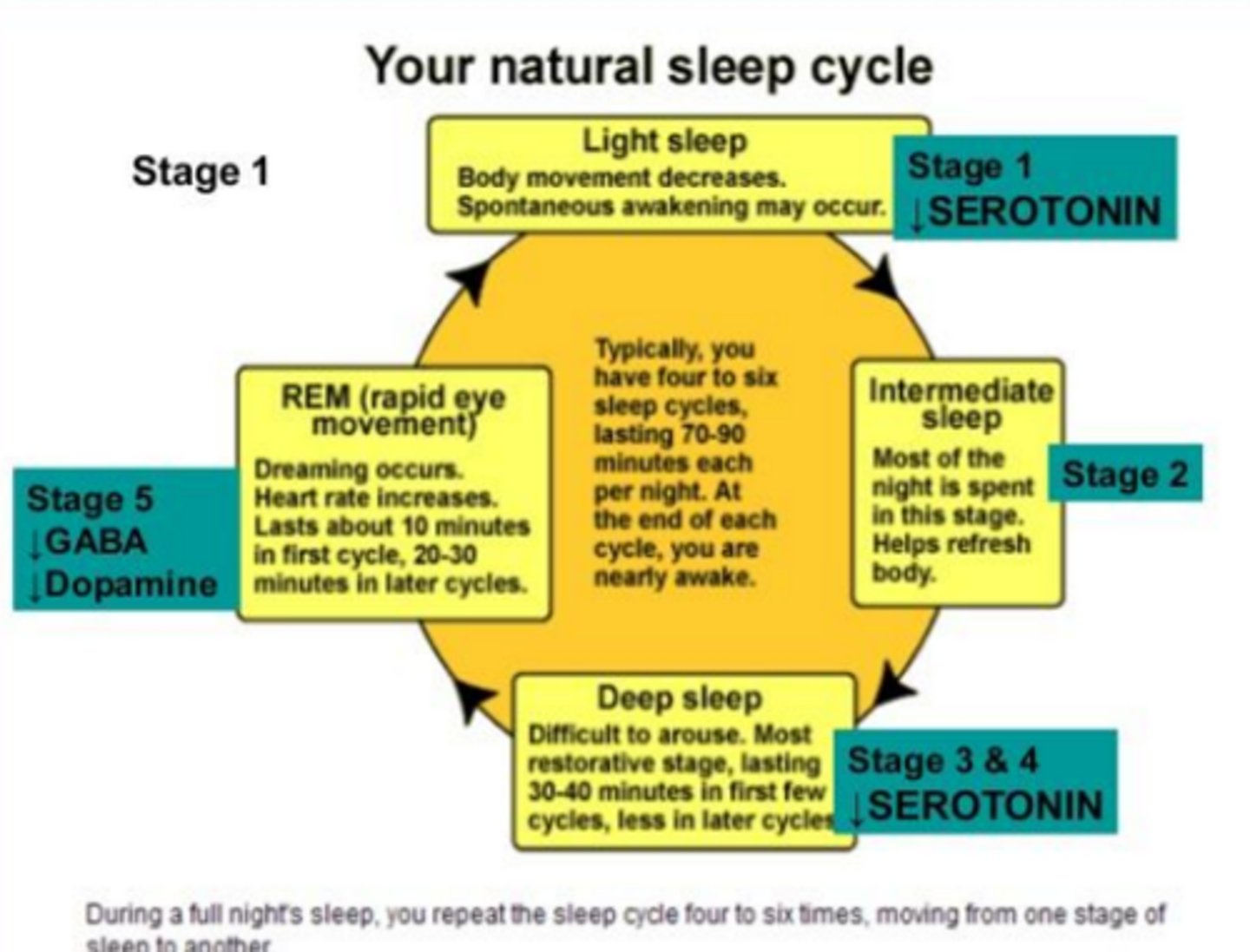
REM sleep
- Rapid eye movement
- Muscle paralysis
- Dreaming
- Brain is MORE active
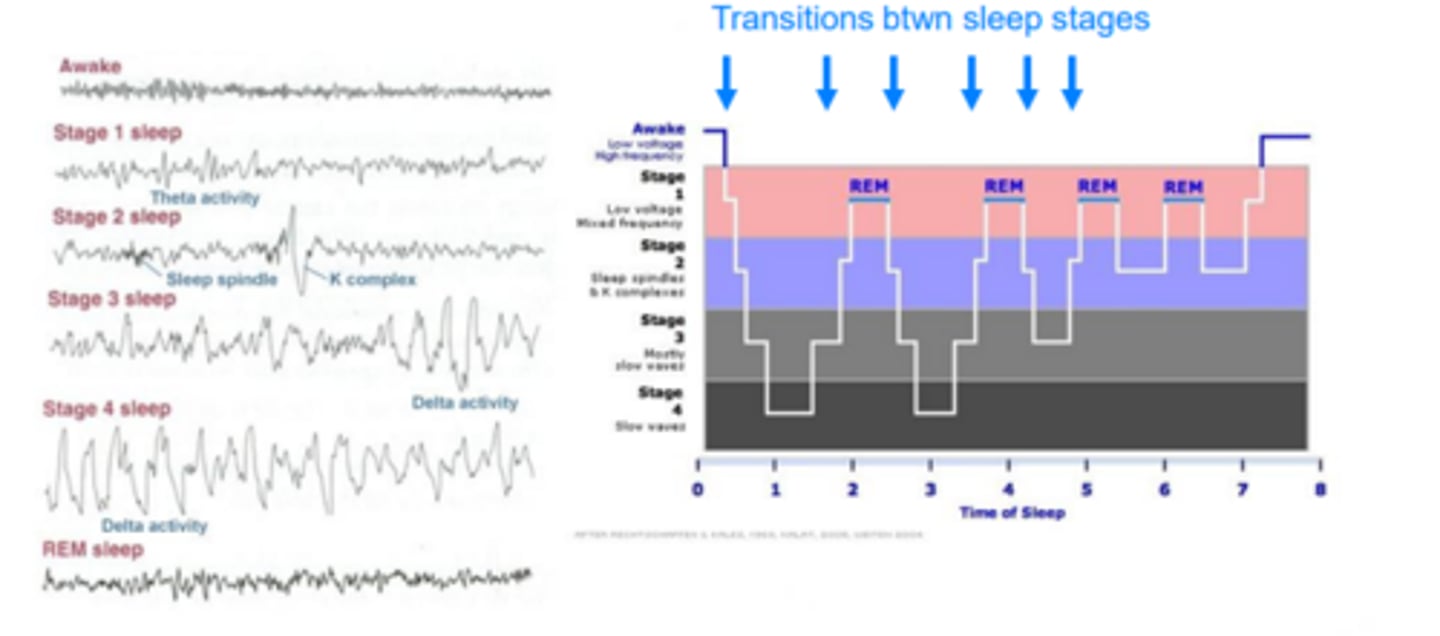
Arousal Systems (wakefulness & sleep)
- Main stages / transitions of wakefulness / sleep
Insomnia
- Trouble initiating or maintaining sleep associated with daytime consequences
- Transient: lasts days
- Short term: less than 3m
- Long / chronic: >3m & 3x / week
Causes of Insomnia
- Situational: work, financial stress, major life events, conflicts, jet lag
- Medical: CV, respiratory, chronic pain, GI, pregnancy
- Psychiatric: mood disorders, anxiety, substance abuse
- Pharmacologically induced: anticonvulsants, central adrenergic blockers, diuretics, SSRIs
Treatment for Insomnia
- Start with non-pharm (OTC, CBT, Sleep hygiene)
- If persists >14 days discuss pharm options
- Choice depends on type of insomnia
Falling asleep insomnia
- Eszopiclone
- Zolpidem
- Ramelteon
- Zaleplon
Staying Asleep insomnia
- eszopiclone
- zolpidem
- doxepin
- suvorexant
Both falling asleep and staying asleep insomnia
- Eszopiclone and Zolpidem (remember EZ)
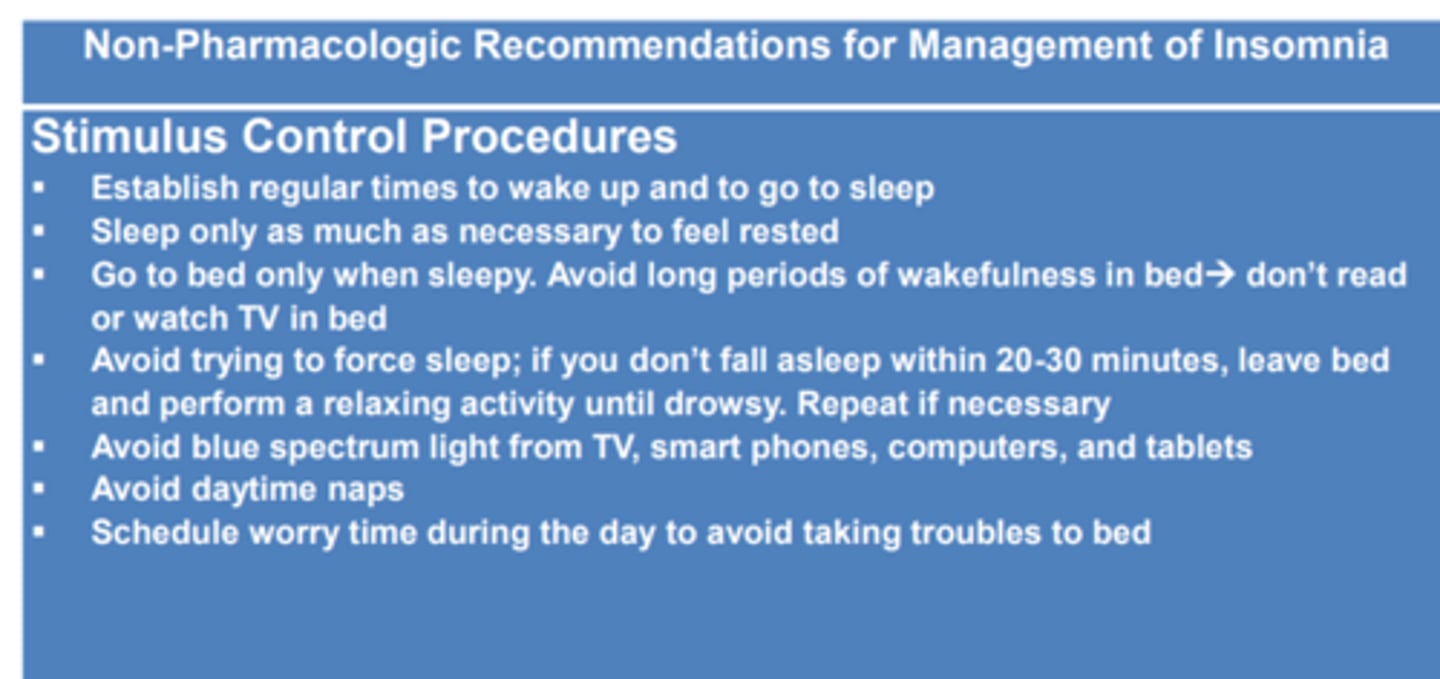
Non pharm treatment
- Stimulus control procedures
- Sleep hygiene recommendations
Stimulus control procedures
- Establish regular times to wake up and to go to sleep
- Avoid blue spectrum light from TV, smart phones, computers, and tablets
- Avoid day time naps
Sleep hygiene recommendations
- Exercise routinely, but not close to bedtime
- Create a comfortable sleep environment by avoiding temperature extremes, loud noises, and illuminated clocks in the bedroom
- Discontinue or reduce the use of alcohol, caffeine, and nicotine
OTC Products
- Antihistamines
- Diphenhydramine and Doxylamine
- Block both H1 and muscarinic receptors
- MILD insomnia
- AVOID in elderly
Dosing Strategies
- Increased Dose ≠ Increased Response
- Consider use for 3 days with an “off” night to reduce
- Should NOT be used for more than 7-10 consecutive nights
- Lower doses required for those with hepatic cirrhosis
Supplements
- Melatonin
- Valerian Root
- Kava
Prescription options
- Benzodiazepines
- Nonbenzos
Benzodiazepines
- Long-Acting Benzodiazepines
- Intermediate-Acting Benzodiazepines
- Short-Acting Benzodiazepines
Long-Acting Benzodiazepines
- Flurazepam
- Quazepam
- Half Life >24 hours
- Daytime sedation, psychomotor incoordination, and cognitive deficits
Intermediate-Acting Benzodiazepines
- Temazepam
- Estazolam
- Half Life of 6-24 hours
- Daytime sedation, psychomotor incoordination, and cognitive deficits
Short-Acting Benzodiazepines
- Triazolam
- Half life <6 hours
- Anterograde amnesia more likely to occur
SE of Benzodiazepines
- Dose dependent
- Tolerance after one month
• Anterograde Amnesia: impairment of memory/recall of events after taken dose
• Rebound Insomnia: increased wakefulness beyond baseline, last a few nights after abrupt discontinuation
• Prolonged sedation and cognitive and psychomotor impairment are common in elderly due to drug accumulation
– BEERS Criteria
Nonbenzos
- Zolpidem, Zaleplon, Eszopiclone
- Suvorexant
- Lemborexant
- Melatonin Receptor Agonists
- Antidepressants
Zolpidem, Zaleplon, Eszopiclone
- MoA: bind to GABA A (agonist effects)
- Only sedative properties (zzzzz drugs)
- Warnings w/ sleep related activities (driving, preparing food, phone calls)
Zolpidem
- Reduces sleep latency and nocturnal awakenings and increases total sleep time
- Take on an EMPTY stomach
- SEs: drowsy, amnesia, HA, GI, weight gain (sleep eating)
Zaleplon
- Decreases time to sleep onset
- Short t ½ (1 hour) → no effects next day and may be used for middle of the night awakenings
- SE: dizziness, HA, somnolence
- DDI with cimetidine (only take 5 mg)
Eszopiclone
- Reduces time to sleep onset, wake time after sleep onset, number of awakenings and increases total sleep time and quality
- Only take for total of 6 months
- Duration of 6 hours → good option for sleep maintenance or early morning awakenin
- SEs: somnolence, unpleasant taste, HA, and dry mouth
Suvorexant
- Difficulty initiating and maintaining sleep
SEs: Somnolence, sleep paralysis (rare) , cataplexy, narcolepsy
- Use NOT Recommended: patients taking STRONG CYP3A4 INHIBITORS
Lemborexant
- Orexin Receptor Antagonist
- Used to induce sleep onset and sleep maintenance
- Side Effects: drowsiness, fatigue, HA
- Rare sleep paralysis / cataplexy
Doses:
- kinda just know women usually need less than men for effective dose
Melatonin Receptor Agonists
- Ramelteon (Rozerem®)
- Tasimelteon (Hetlioz® )
Ramelteon (Rozerem®)
- Sleep-Onset Insomnia
- Mt1 and MT2 agonist
- NOT controlled
- AVOID taking with or immediately after a high-fat meal
Tasimelteon (Hetlioz® )
- Non-24-Hour Sleep Wake Disorder
- May take weeks to months to work
- Drug Interactions: Strong CYP1A2 inhibitors and 3A4 inducers
Antidepressants
- TCAs
- Trazodone
TCAs
- Amitriptyline(Elavil), Nortriptyline (Pamelor), Mirtazapine (Remeron) and Doxepin
- SEs: adrenergic blockade, daytime sedation, weight gain, anticholinergic activity and cardiac conduction prolongation
Trazodone
- Improves sleep continuity
- Inhibits reuptake of serotonin
- Effective for patients with SSRI or Bupropion induced insomnia and in substance abuse
Evaluation of Outcomes
-After 1 Week: Assess efficacy, SE, adherence to nonpharm recs
- Keep sleep diary
- Educate on tolerance, withdrawal, rebound insomnia
- Abuse potential