Unit III Exam Study Guide
1/161
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
162 Terms
Motor Equivalence
The ability of different motor systems to achieve the same behavior.
Ex: Writing can be performed using different parts of the body (dominant hand, nondominant hand, feet, mouth)
Functions of the Corticobulbar pathways?
Corticobulbar pathways are descending pathways from the motor cortex to the cranial nerve nuclei in the brainstem. These pathways are for descending motor control only and will go to motor cranial nerve nuclei.
Upper Motor Neuron lesions .....
Occur in anything in descending pathways above LMN, so anything outside of the ventral horn
Where does the Ventral Corticospinal Pathway terminate?
In the ventral horns bilaterally
Function of the Tectospinal Pathway
Helps maintain neck position by using eye position to modulate our spine for upright position. Only travels to the cervical spine.
Medial Vestibulospinal pathway function
Coordinates neck and head righting reactions for balance
Which of the following is true about motor unit size?
a)Motor units with more muscle fibers are used for fine motor tasks
b)Fast fatigable motor units are recruited second
c) Smaller motor units have fewer muscle fibers per alpha motor neuron
d) Larger motor units are recruited first
C) Smaller motor units have fewer muscle fibers per alpha motor neuron
Which of the following thalamic nuclei is part of the pathway for somatosensation from the body?
a) Medial geniculate
b) Ventral posteriolateral
c) Lateral geniculate
d) Ventral mediolateral
B) Ventral Posteriolateral
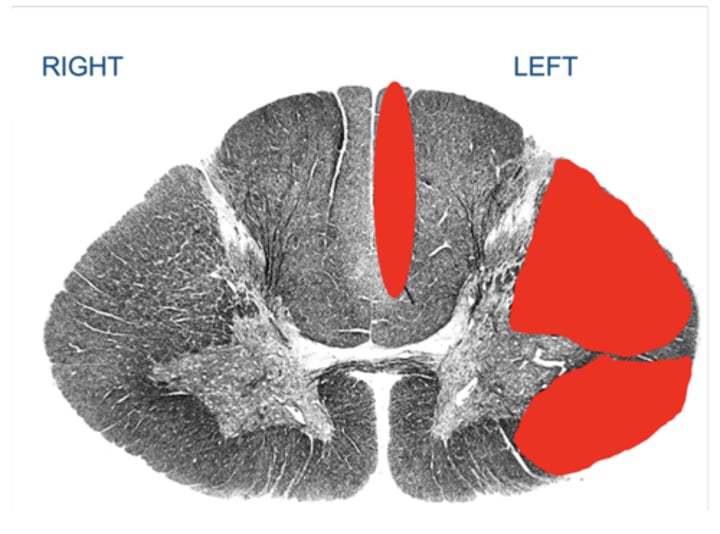
Your patient suffered an injury to the C7 section of the spinal cord. The image below illustrates where the damage (i.e., the lesions) is located by regions covered with red coloring. Note: the image is stained so axons appear dark.
Which of the following answers best describes the patient's expected sensory changes?
a) Loss of left arm proprioception
b) Loss of right arm pain
c) Loss of right arm proprioception
d) Loss of left arm pain
B) Loss of right arm pain
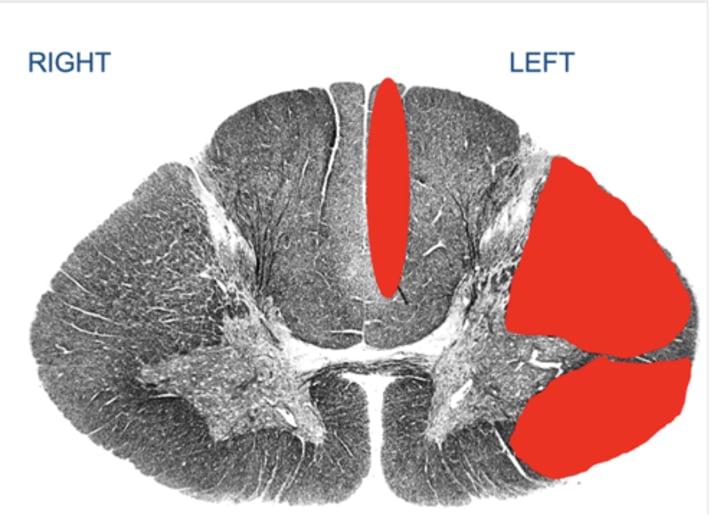
Your patient suffered an injury to the C7 section of the spinal cord. The image below illustrates where the damage (i.e., the lesions) is located by regions covered with red coloring. Note: the image is stained so axons appear dark.
Which of the following answers best describes the patient's expected sensory changes?
a) Loss of left leg light touch
b) Loss of left arm right touch
c) Loss of right leg light tough
d) Loss of right arm light touch
A) Loss of left leg light touch
What occurs to the neuron's membrane potential during the refractory period?
The membrane potential decreases below the resting membrane potential
Which of the following ascending pathways brings information about pain to endogenous opioid pathways in the periaqueductal gray matter?
Spinomesencephalic
Which of the following glial cells help make up the blood brain barrier?
Astrocytes
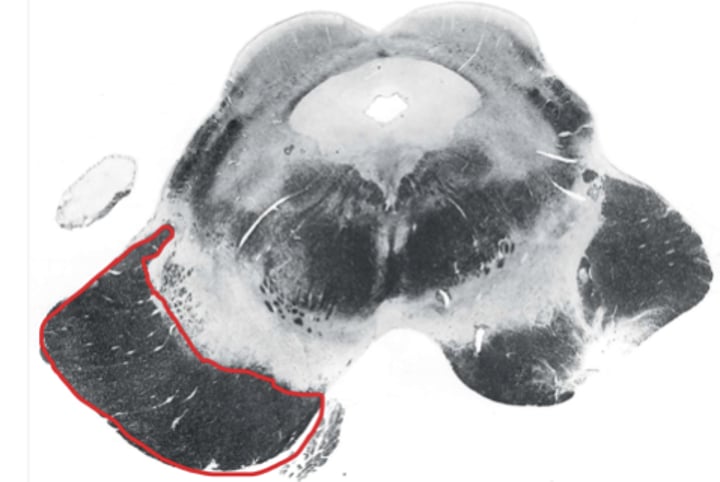
Cerebral Peduncle
Which of the following neurotransmitters can have excitatory or inhibitory effects?
Dopamine
Which of the following best describes the function of the Frontal Eye Fields?
they control voluntary lateral eye movements
Which of the following symptoms is commonly associated with Parkinson's disease?
Bradykinesia
Your patient presents with right-sided face weakness. You see bilateral wrinkling of the forehead when you ask the patient to "open your eyes and wrinkle your forehead".
Left primary motor cortex
Exceptions of lesions to Primary Motor Cortex
Flaccid paralysis (due to cerebral shock, and long-term hypotonia
Lesion to Primary Motor Cortex would result in
UMN signs and symptoms !
Which functional areas are responsible for planning?
a) SMA
b) Premotor Cortex
c) Posterior Parietal Cortex
d) All of the above
D) All of the above
Lesion to SMA would result in ..
Apraxia (can't plan and initiate movements)
Difficulty with tasks requiring coordination of both hands/feet
Lesion to cingulate gyrus
Lesion to Frontal eye fields
Eyes deviate towards side with lesion
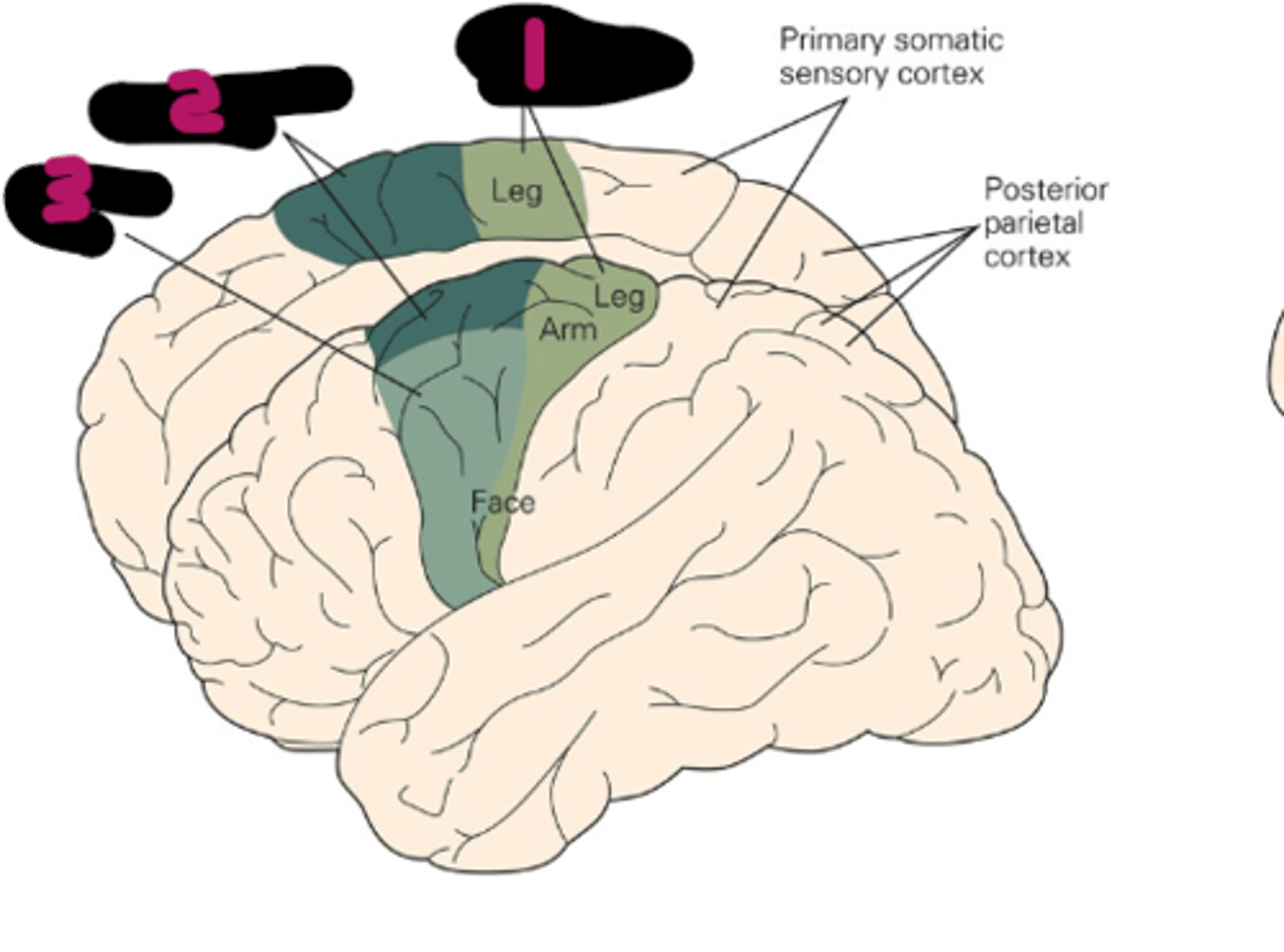
Where is the Supplementary motor area located?
Anterior to Primary Motor Cortex on medial side; #2 on image
Where are the Frontal Eye Fields located?
Just anterior to the Premotor are on the lateral side of each hemisphere
Explain lesions to the Primary Motor Cortex and Premotor Cortex
Provide bilateral info to the upper facial muscles only. Lower facial muscles get contralateral information (right side of cortex controls left side of lower facial muscles.
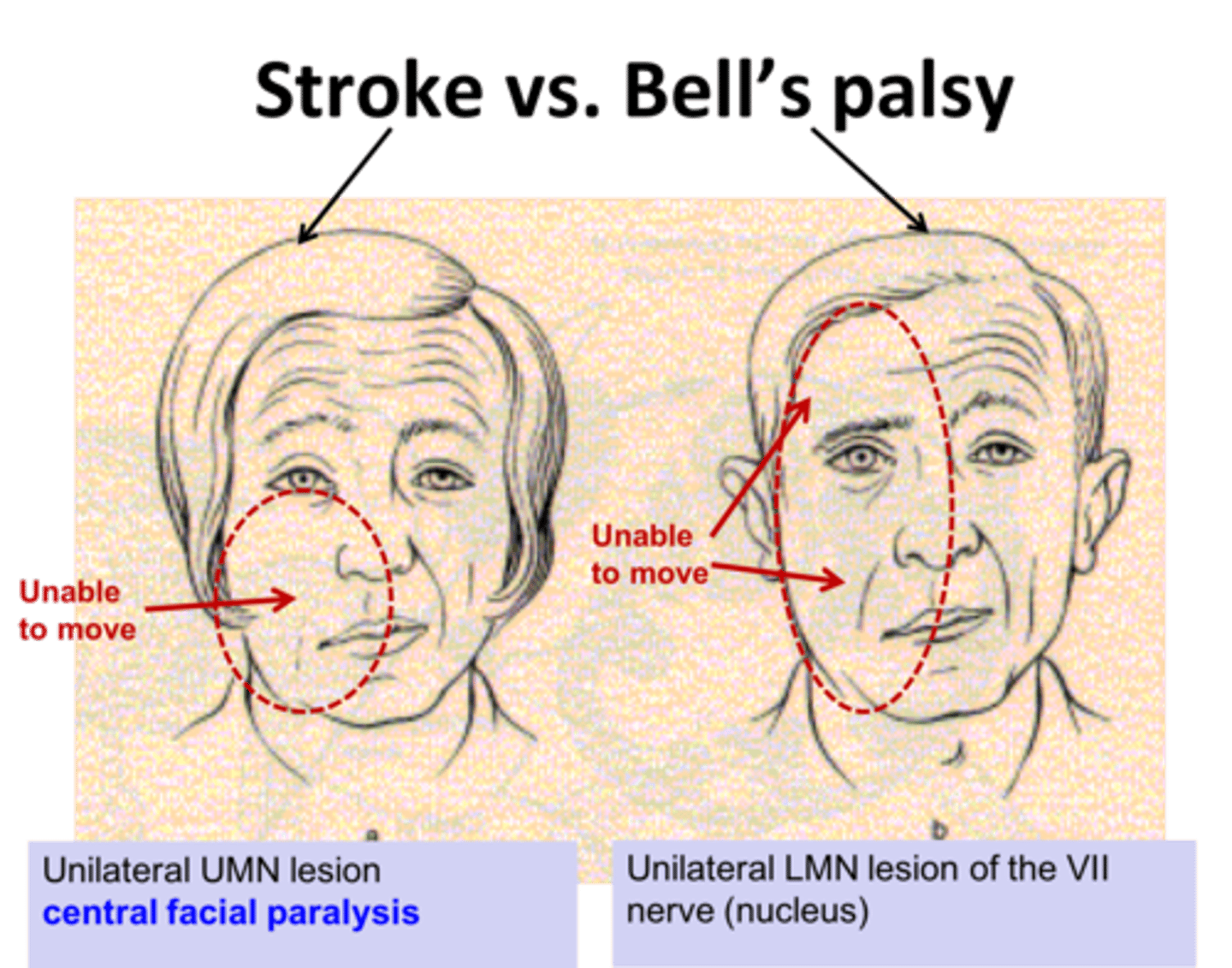
What does a lesion to the Primary Motor Cortex and Premotor Cortex look like?
Stroke; patient can wrinkle forward due to bilateral control to upper facial muscles
2 flocculi with nodulus connecting the two
Flocculonodular Node
What pathways are influenced by the Cerebrocerebellum?
Both Dorsolateral and Ventromedial
Which pathway is influenced by the Spinocerebellum (intermediate)?
Dorsolateral Pathway
What pathway is influenced by the Vestibulocerebellum?
Ventromedial (especially brainstem pathways)
Which is the middle layer of the cerebellum?
Purkinje Cell Layer
Explain the general flow of info between the cerebellar peduncles, purkinje fibers, and deep nuclei
Information enters the cerebellum via the cerebellar peduncles and travels out to the Purkinje fibers. Information then travels from the Purkinje fibers to the deep nuclei and then out of the cerebellar peduncles (mainly superior) out to the thalamus and then primary motor cortex.
What is Ataxia?
Overshooting, jerky movements
What is Dysmetria?
An ataxia in which judgement of distances is off
Indicates a problem with agonist-antagonist rapid alternative movements
Ipsilateral Disdiadochokinesia
What are the common function of the basal ganglia?
- Contribute to normal movement patterns
- Planning and execution of complex motor tasks
- Control fast (saccadic) eye movements
- Establishment of motor memories
- Involved in our psychological well-being and with the production of emotion responses
Input (receptive) for basal ganglia
Striatrum (caudate and putamen)
Output (projective) for basal ganglia
Pallidum (Globus Pallidus)
What structures make up the dorsal striatum?
Caudate Nucleus
Putamen
What structures make up the ventral striatum?
Nucleus Accumbens
What structures make up the dorsal pallidum?
Globus Pallidus
What are the afferents for the motor circuit?
Somatic Sensory Cortex, Primary Motor Cortex, Premotor and Supplementary Motor Areas
Receptive components for the motor circuit of the basal ganglia?
Putamen
Projective components for the motor circuit of the basal ganglia?
Globus Pallidus and Substantia Nigra
Dopamine inhibits movement
Indirect Pathway
1. Dopamine excites the putamen
2. Putamen is going to inhibit the Globus Pallidus
3. Inhibits through the thalamus
4. Excitation of movement of the cortex
Normal effect of the Globus Pallidus on motor activity
Destruction of the subthalamic nucleus of the indirect pathway which results in lots of movement
Hemiballismus
Death of putamen neurons produces involuntary movements that look like fragments of goal-direct movements
Chorea
Hereditary disorder that produces chorea. Symptoms include severe personality changes, cognitive impairments, and movement disorders ( like chorea)
Huntington's Chorea
Common signs and symptoms of Parkinson's disease
- Bradykinesia
- Akinesia
- A mask like expression of the face
- Shuffling gait
Deep brain stimulation is treatment for
Parkinson's Disease
Production of the saccadic eye movements
Oculomotor Circuit of Basal Ganglia
Impairment of working memories that have spatial component
Lesion to Executive Circuit of the Basal Ganglia
Obstacle course, forgetting that there is a step at a point in the course. Defect in directing future movements at patient can't recall info based off of the spatial environment
Example of lesion to Executive Circuit of the Basal Ganglia
Production of emotional response
Limbic Circuit of Basal Ganglia
Feedforward control
Preparation for a movement
Feedback control
Response to perturbations of movement
Alpha Motor Neuron cell bodies are located in the ....
Ventral Horn of every spinal cord segment and motor nuclei for cranial nerves in the brainstem
Shoulder Elevation
C4
Shoulder Abduction
C5
Elbow Flexion, Wrist Extension
C6
Elbow Extension, Wrist Flexion
C7
Finger Flexion
C8
Finger Abduction
T1
Hip Flexion
L2
Knee Extension
L3
Ankle dorsiflexion
L4
Great Toe Extension
L5
Topographic Organization of Ventral Horn
Explains why a patient may have difficulty or trouble with physical movements vs trouble with postural movements
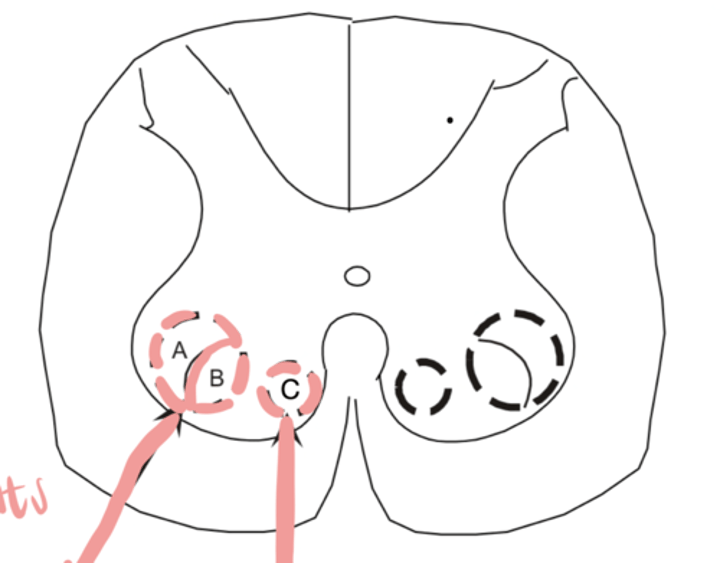
An injury or damage to A would present as
Trouble with distal limb movements
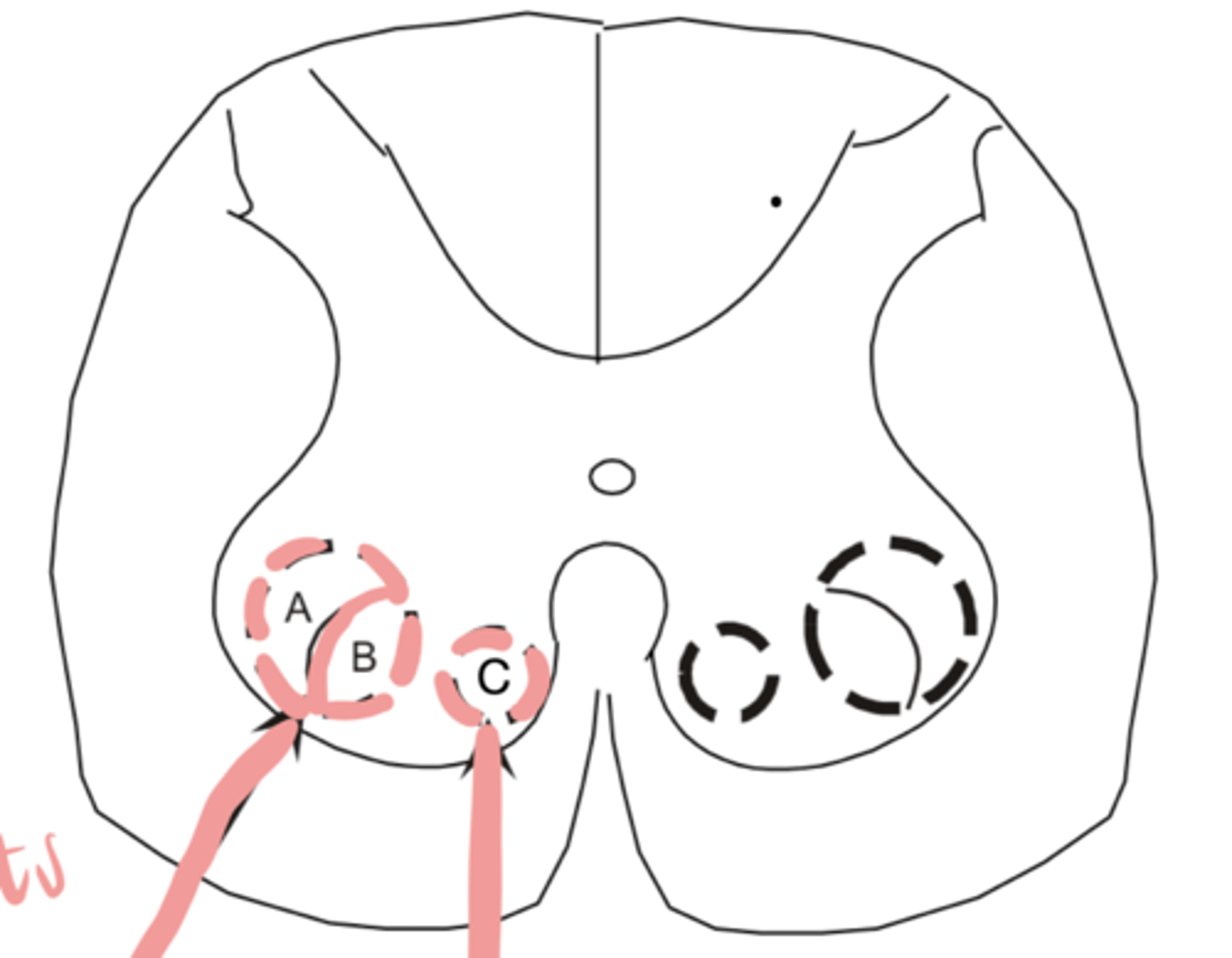
An injury or damage to B would present as
Trouble with proximal limb movements
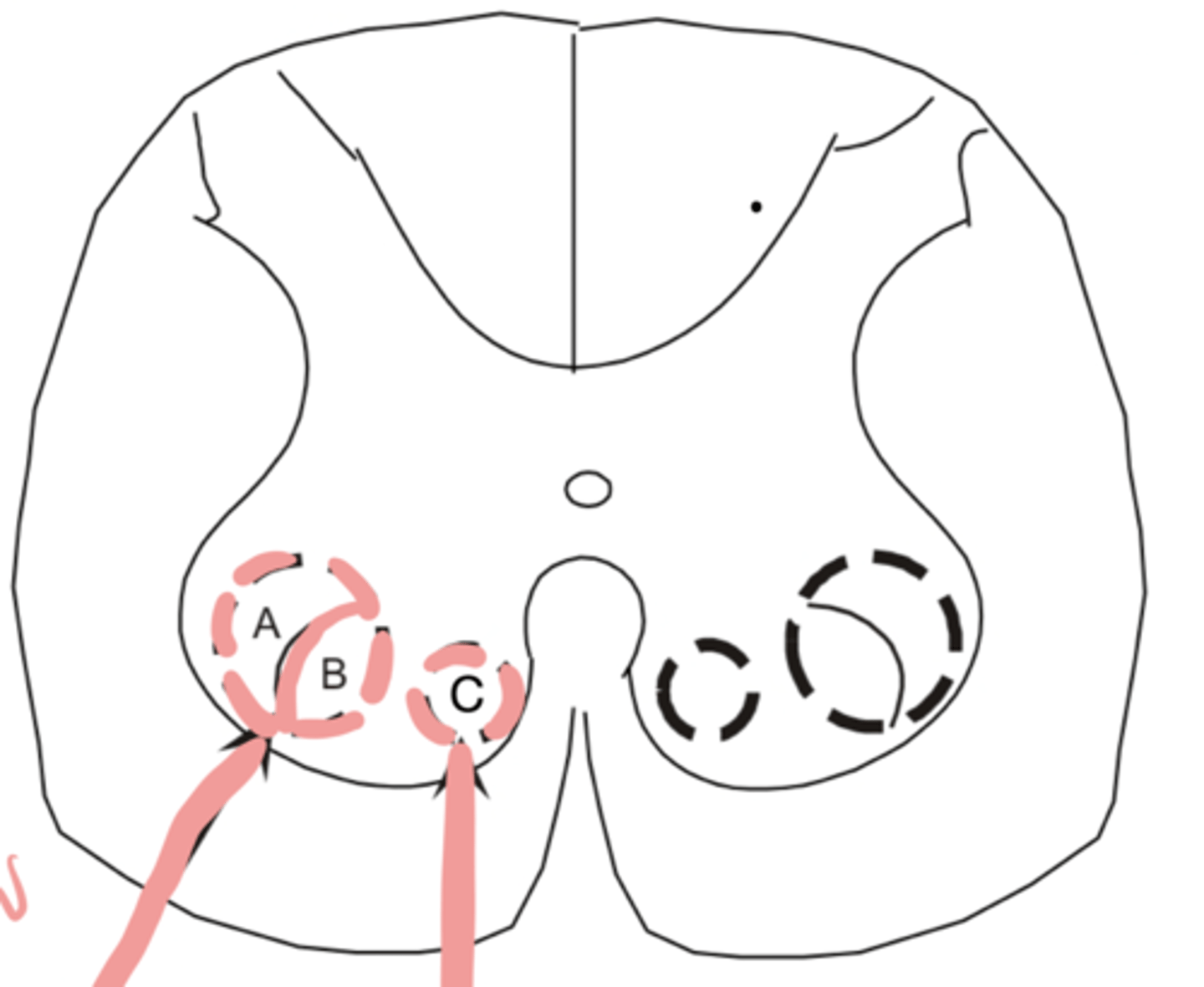
An injury or damage to C would present as
Trouble with postural movements
What is a motor unit?
A motor neuron and all of the muscle fibers it innervates
Slow Motor Units
Produce low amounts of force but over a long time
Fast Fatigue-Resistant Motor Units
Produces moderate - lots of force. Fatigue resistant for a moderate amount of time
Fast Fatiguable Motor Units
Produces lots of force but not for long, fatigues quickly
What kind of tasks require small motor units?
Fine motor and precision tasks
What kind of tasks require large motor units?
Gross motor tasks
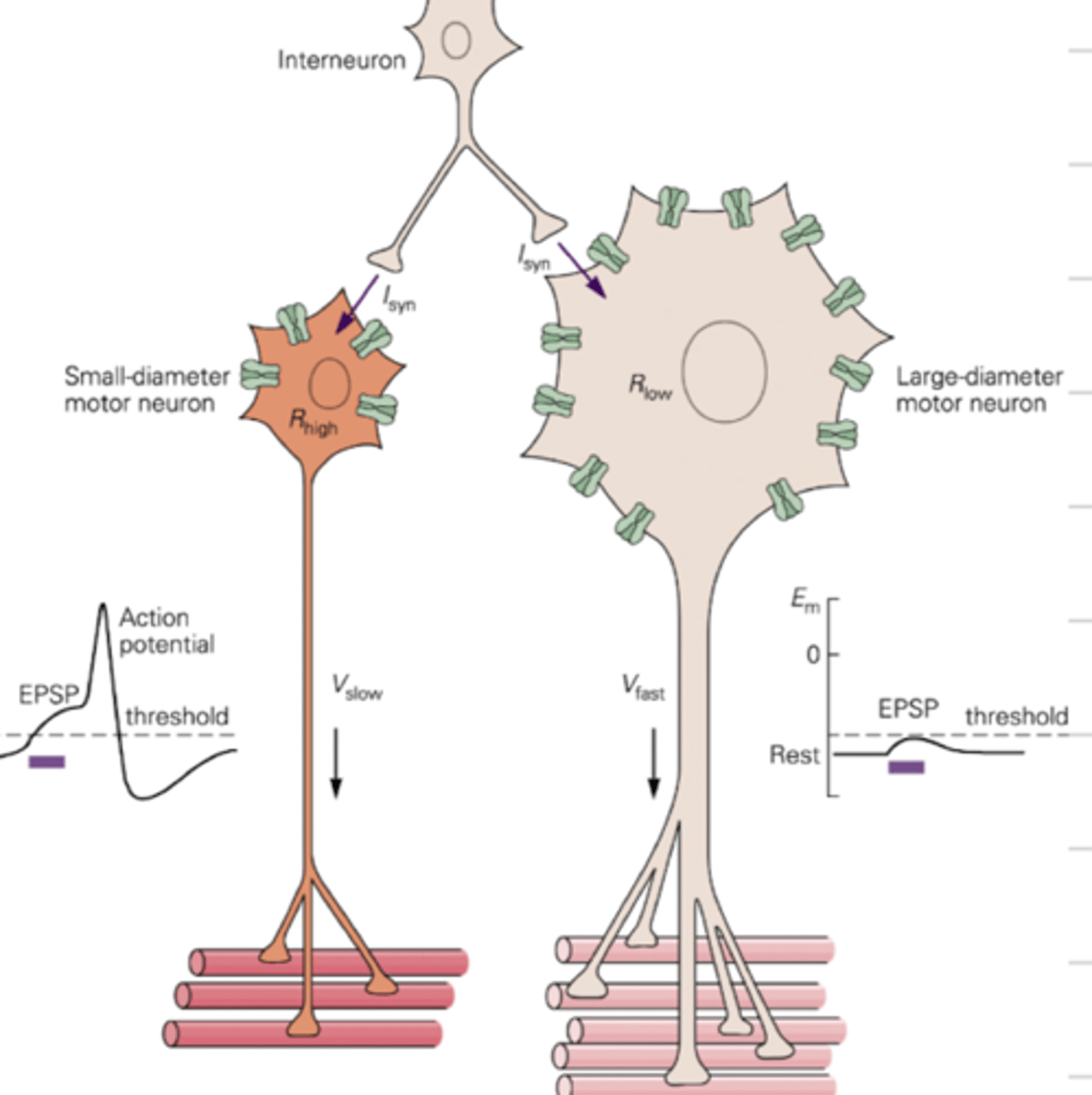
The Size Principle
Governs recruitment of motor units into action. Info comes down to a LMN into the Ventral Horn and a neurotransmitter is released triggering an excitation potential in the LMN. Small Motor Units reach threshold for for an action potential quick causing a muscle contraction. If the neurotransmitter continues, the large motor unit will reach its threshold.
What are the two mechanisms for increasing force production?
Population Coding and Frequency Coding
Recruiting more units is which mechanism?
Population Coding
Which mechanism is rate coding, where each motor unit is firing faster?
Frequency Coding
What are the functions of all reflexes?
To adjust for unexpected perturbations
To organize patterns for coordinated movements
To allow for rapid production from painful or damaging stimuli
- You don't need perception of sensation to obtain a reflex contraction.
- Descending control from the cerebral cortex and brainstem can influence or regulate reflexes by increasing or decreasing the size of the reflex response but you don't need descending motor pathways to have a reflex present
- Stimulation of a spinal reflex pathway may be used to obtain a motor response in a patient
- Motor response occurs over a very short time frame and usually does not last once stimulus is gone
- Descending path lesions WILL NOT abolish reflexes. They make the spinal reflex presentation abnormal and less flexible.
5 Characteristics of Reflexes
How does the Nervous System modulate the GTO reflex?
Protects muscle from exerting excessive force. IB inhibitory interneurons inhibit the muscle from producing more force.
Explain the Flexor Withdrawal Reflex and Crossed Extension
Painful stimulus stimulates nociceptors, and cutaneous afferent nerve fibers transmit signal to spinal cord and synapse on LMN. This reflex is intersegmental, meaning many muscles are coordinated activate at once to withdraw the limb. The opposite limb goes into extension to support your body. Flexed limb is rapidly protecting the body
Cutaneous Stimulation
Fast "icing", brushing, or stroking to the skin contracts muscle underneath stimulated area.
What does maintained heat do to the muscle
It relaxes or inhibits the muscle
What reflexes or reflex changes are associated with UMN syndrome or lesions?
Babinski Reflex and Clonus
If the toes fan out in the Babinski Reflex, this means
Positive for UMN lesion
What does clonus mean for a UMN lesion?
No inhibition or fatiguing of the stretch reflex. Makes the reflex repetitive
What is spasticity in an UMN lesion?
Stretch reflex disorder in which there is an increase in muscle tone that is apparent with rapid stretching. Also characterized by hyperreflexia (exaggeration) of the stretch reflex.
UMN Lesion
Hypertonia
Hyperreflexia
No early atrophy (may occur months later due to disuse)
Nonsegmental and contralesional or ipsilateral
LMN Lesion
Hypotonia
Hyporreflexia
Muscle atrophy
Segmental and ipsilesional
What are the different Ventromedial White Matter Pathways?
Tectospinal, Reticulospinal (Pontine & Medullary), Vestibulospinal (Lateral & Medial) and Ventral Corticospinal
What are the different Dorsolateral White Matter Pathways?
Rubrospinal and Lateral Corticospinal
Function of Rubrospinal pathway?
Muscle tone in flexor muscles
Function of Lateral Corticospinal pathway?
Primary pathway for all of our voluntary movement for limbs