Intra-Abdominal Infections
1/45
Earn XP
Description and Tags
1.5 LH - I really doubt he will ask about the normal flora even though it's on study guide so ignore that if it's too much
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
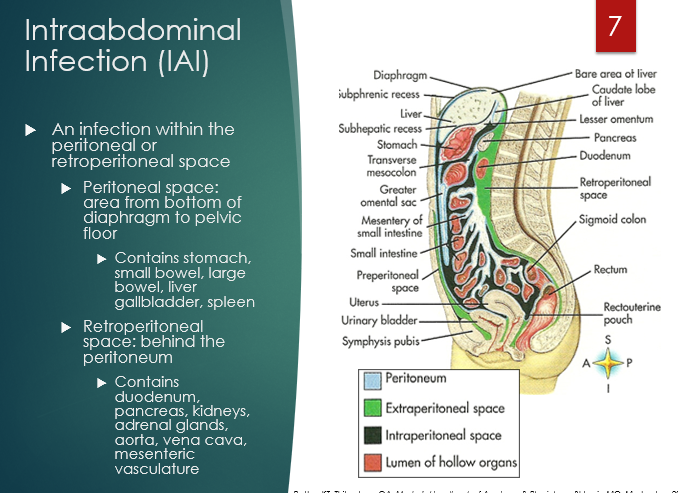
An intraabdominal infection is one that is located within the _________ or _____________
An infection within the peritoneal or retroperitoneal space
Define uncomplicated and complicated IAIs
uncomplicated if infection remains contained within an organ
complicated if it extends beyond a single organ, involves anatomical disruption, peritonitis
peritonitis = (inflammation of the peritoneum) or abscess (localized collection of pus caused by infection - dead WBC, bacteria, tissue + fluid)
What is the difference between primary, secondary, tertiary peritonitis?
Primary - (spontaneous) = infection w/o any clear source of the infection
Secondary - infection of peritoneal cavity caused by another infection within the abdomen
Tertiary - persistent or recurring infection after tx of primary or secondary that happens >48h after it seemed controlled
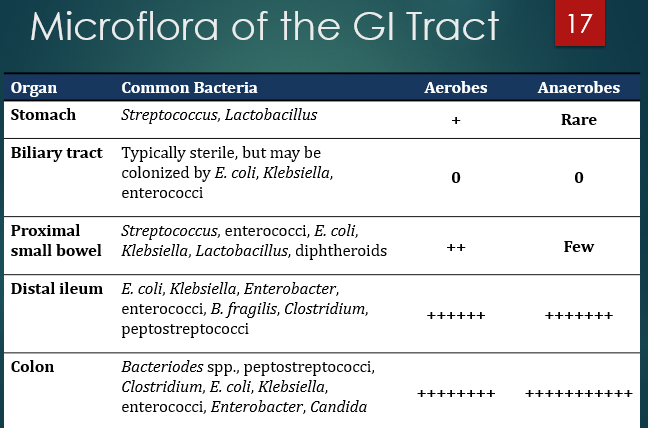
what flora are normal to the stomach?
streptococcus and lactobacillus
what flora are normal to the bilary tract?
e. coli, klebsiella, enterococcus
Infection occurs because abdominal organs leak bacteria into the peritoneal cavity
secondary peritonitis
Infection occurs without GI perforation (blood spread or bacterial translocation).
Primary peritonitis
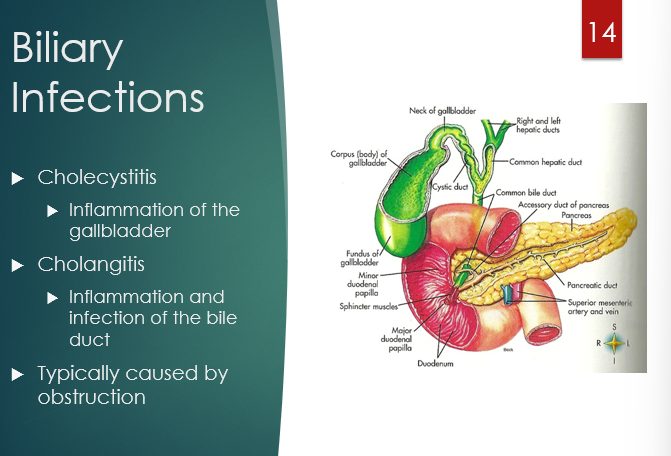
inflammation of the gallbladder
cholecystitis
inflammation and infection of the bile duct
cholangitis
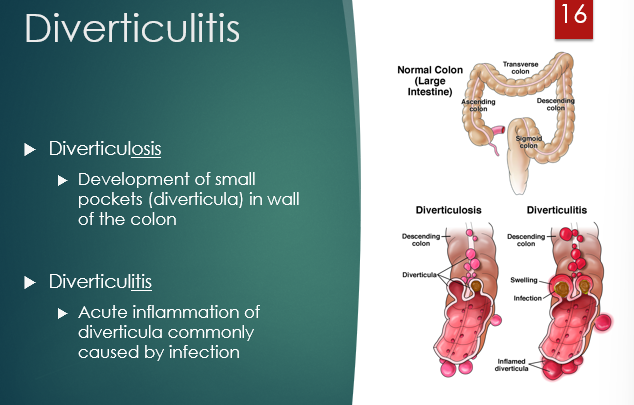
What is the difference between diverticulitis and diverticulosis?
diverticulosis - small pockets develop in wall of colon
“ “ itis - acute inflammation of diverticula caused by infection
What generalization about number of bacteria and aerobes/anaerobes can you make as you go down the GI tract?
as you go down the GI tract the # of bacteria increases and anaerobes become dominant
The biliary tract is normally sterile. If infection (usually ascending from the intestine) is present, what 3 bacteria would be suspected to colonize?
e. coli; klebsiella; enterococci
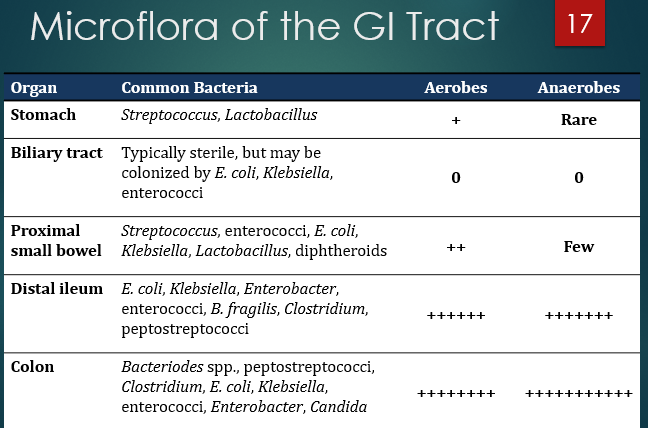
Prob low yield - (aside from stomach) - Which THREE bacteria are located in all regions of the GIT?
e. coli, klebsiella, enterococci
Colonizers of the proximal small bowel, aside from the 3 that are everywhere:
strep, lactobacillus, diptheroids
(+ e. coli, klebsiella, enterococci)
Colonizers of the distal ileum, aside from the 3 that are everywhere:
enterobacter
b.fragilis
clostridium
peptostrepto
ebcp
(+ e. coli, klebsiella, enterococci)
Colonizers of the colon, aside from the 3 that are everywhere:
= distal ileum BUT NOW WITH candida
Are primary and secondary peritonitis usually mono or polymicrobial?
primary = mono
secondary = poly
common bacteria that are culprits in cirrhosis SPB (primary;spontaneous)
e. coli
klebs
strep pneumo
h.influenzae
What family is klebsiella:
Enterobacteriaceae (gram negative rods)
What is the oxygen requirement of enterobacteraceae?
facultative anaerobes
What are the GRAM POSITIVES that are culprits in peritoneal dialysis-associated primary peritonitis?
staph, strep, and enterococci
What are the GRAM NEGATIVES that are culprits in peritoneal dialysis-associated primary peritonitis?
e.coli, klebs, and psuedomonas
Way of remembering the pathogens that can cause a secondary peritonitis
anything that we said colonized the GIT + proteus
List the big 3 most clinically important anaerobes that we see:
bacteroides
clostridium
peptostrepto
difference in s/s of primary vs secondary peritonitis
primary sx are vague and mild and pretty nonspecific + moderate iflammation
secondary are acute and severe, sepsis/medical emergency signs + high inflammation
How is spontaneous bacterial peritonitis diagnosed (i.e., what is the main diagnostic criteria)?
paracentesis - ascitic PMN count ≥ 250 cells/mm³ is the main diagnostic criterion ± culture to identify pathogen
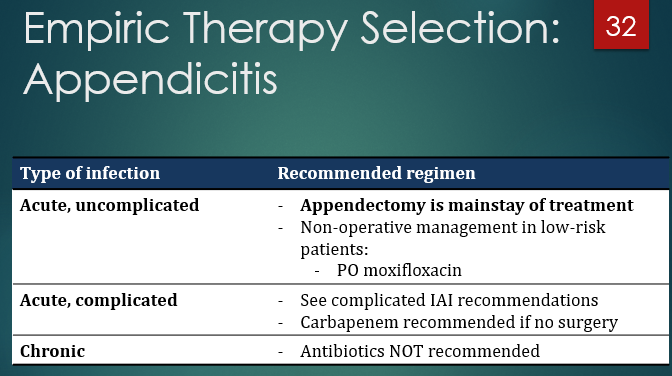
mainstay of uncomplicated IAI treatment
surgical management
T/F - Primary peritonitis may often be managed with abx alone
true; in secondary the abx have more of a supplemental role to surgical intervention
Say you want to design an empiric regimen for secondary bacterial peritonitis… what general spectrum would you aim for?
gram negative that covers both aerobes and anaerobes
T/F - an empiric regimen for secondary peritonitis should always include enterococci, fungal, and MRSA coverage
false;
Empiric enterococcal coverage recommended only in high-risk patients
Fungal coverage is NOT recommended empirically
Antifungal therapy is indicated for higher-risk patients with IAI if Candida spp. is grown from an intraabdominal culture
MRSA also typically not rec’d
Source control (non-pharm procedures) are almost always needed for secondary peritonitis. This includes what 4 steps, starting with
draining the abscess
?
?
?
draining the abscess
correcting perforation
remove dead tissue
irrigate w/ NS
What are some of the characteristics that make a patient “high risk” for treatment failure? List at least two.
HEALTHCARE-ASSOCIATED IAI
sepsis or shock
APACHE-II score > 10
comorbidities (hepatic, CV, malignancy, renal)
(FYI) What generalizations can you make about the empiric coverage for treating biliary infections?
Mild
Moderate
Severe
as severity increases, we get more nuclear and increase severity of coverage
Mild - use narrower gram-negative coverage
moderate - broader gram neg + anaerobes
severe/healthcare - broader spectrum + MRSA coverage
gram (-) rods + anaerobes
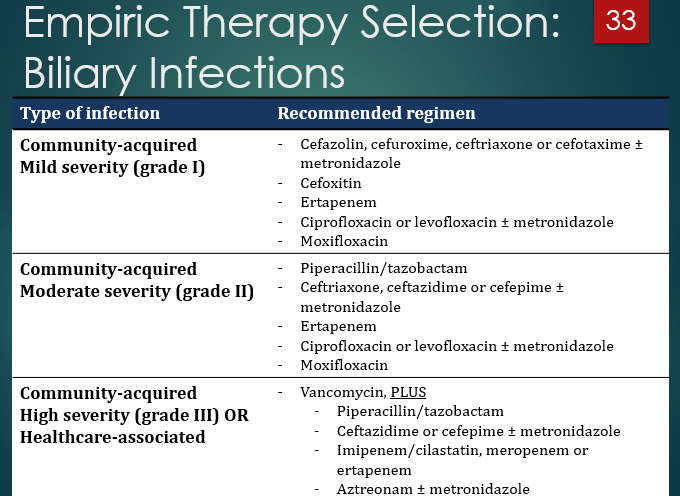
Why is metronidazole often added on to cephalosporins?
for anaerobe coverage (cephalosporins do not reliably cover anaerobes)
List at least 3 drugs that cover anaerobes:
pip/tazo
carbapenems
cefoxitin (2nd gen)
moxifloxacin
When do we add vanco in the contxt of empiric tx for biliary infections? Why?
When high severity or healthcare-associated - to cover MRSA

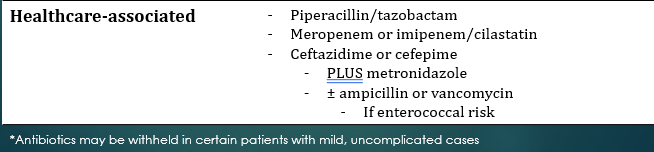
A way to think about treating diverticulitis is to always cover flora from the ______
colon (colonic diverticulum is what gets infected)
(again, gram negative rods and anaerobes)

Which two drugs should always raise a flag to add metronidazole to due to lack of anaerobe coverage?
cephalosporins* and FQs
*some exceptions
Why might ampicillin or vanco be added in healthcare-associated diverticulitis?
Enterococcus coverage
What is the preferred empiric treatment for spontaneous bacterial peritonitis?
IV 3rd-generation cephalosporin
• ceftriaxone
• cefotaxime
Most common cause of primary peritonitis
Cirrhosis with ascites
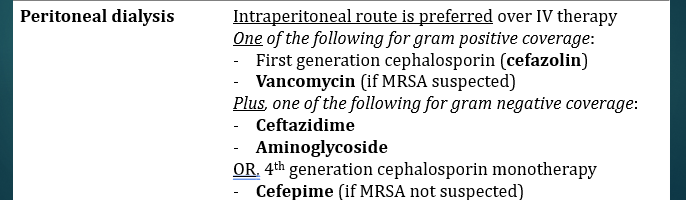
Preferred antibiotic route for peritoneal dialysis peritonitis
Intraperitoneal (not IV)
Gram-positive coverage for peritoneal dialysis peritonitis
Cefazolin (gen 1)
Vancomycin (if MRSA suspected)
Gram-negative coverage for peritoneal dialysis peritonitis
Ceftazidime
Aminoglycoside
cefipime (if no suspected MRSA) (would be monotherapy)
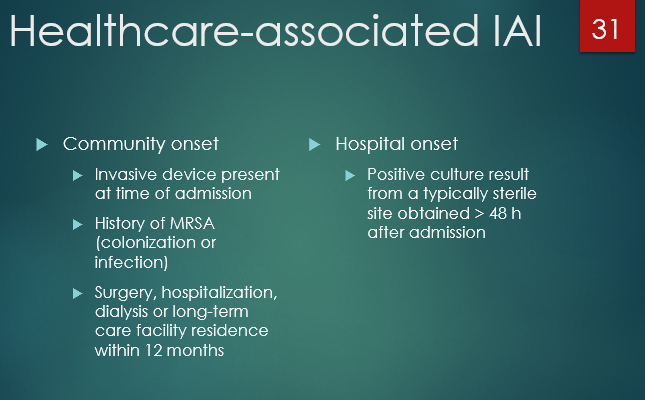
How do we distinguish between a community onset and healthcare onset IAI?
healthcare = obtained >48h after admission
community - see attachment
What is the first line preferred antibiotic regimen for chronic appendicitis?
ANTIBIOTICS ARE NOT RECOMMENDED!