INB365S: Electrical Events of the Heart
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
What happens where the sarcomere becomes shorter?
the whole muscle becomes shorter = contraction
contraction pulls a bone closer to another bone to create movement
= gliding door (exists in skeletal and cardiac muscle (NOT smooth muscle)
thick filaments
made of myosin (head + tail)
thin filaments
actin chain made up of tropomyosin, troponin, and g-actin molecules
tropomyosin
covers the binding sites of actin in thin filaments
= duck tape
troponin
sensor
Ca2+ binds to troponin to trigger muscle contraction
g-actin molecule
interacts with myosin
** actin and myosin naturally want to glue together
Initiation of contraction
Ca2+ levels increase in cytosol
Ca2+ binds to troponin
Troponin-Ca2+ complex pulls tropomyosin away from actin’s myosin-binding site
Myosin binds strongly to actin and completes power stroke
Actin filament moves
Why are dead bodies rigid?
Muscle relaxation requires ATP!!!!!!!!!!!
What happens when ATP binds to myosin?
Myosin releases actin.
Myosin hydrolyzes ATP.
Energy from ATP rotates the myosin head to the cocked position.
Myosin weakly binds to actin
Relaxation!
Where does the signal for muscle contraction come from?
Motor cortex → neurons go to spinal cord → skeletal muscle
Initiation of Muscle Action Potential
Somatic motor neuron releases ACh at neuromuscular junctions (nicotinic receptors = nonselective cation receptors) at motor end plate
Net entry of Na+ through ACh receptor-channel causes depolarization → end plate potential
Generates action potential through T-tubule
Muscle Action Potential in T-tubule (skeletal muscle)
Triggers DHP to open RyR Ca2+ release channels in sarcoplasmic reticulum
Ca2+ enters cytoplasm
Ca2+ binds to troponin, allowing actin-myosin binding
Myosin heads execute power stroke
Actin filament slides toward center of sarcomere
Relaxation Phase! in skeletal muscle
sarcoplasmic Ca2+-ATPase pumps Ca2+ back into SR
decrease in the free cytosol causes Ca2+ to unbind from troponin
Tropomyosin re-covers binding site. When myosin heads release, elastic elements pull filaments back to their relaxed position
short coming of skeletal muscle
Summation of contractions: stimuli closer together do not allow muscle to relax fully
1. Unfused tetanus: stimuli are far enough apart to allow muscle to relax slightly between stimuli (= not all Ca2+ pumped back to SR)
2. Tetanus: muscle reaches steady tension. If muscle fatigues, tension decreases rapidly
What is the force of contraction proportional to?
The force of contraction is proportional to the concentration of calcium!!!!!!!!!
Contractility in cardiac cells is graded!!!!!!!!!!!
pacemaker cells
spontaneously fire to generate action potential
do not need external stimuls to trigger action potential
depolarization of pacemaker cells spread rapidly to adjacent contractile cells through gap junctions
- note that pacemaker cells and contractile cells have different action potentials!
most famous pacemaker
SA node
right atrium
Action potential in pacemaker cells
Funny channels open (no stabilized resting potential) as a result of hyperpolarization
Net Na+ in
Some Ca2+ channels open, funny channels close
Lots of Ca2+ channels open
Ch2+ channels close, K+ channels open
K+ channels close
Funny channels open
Action potential in contractile cells
stabilized resting potential
signal from pacemaker cells is received
Na+ channels open
Na+ channels close
Ca2+ channels open; fast K+ channels close = Ca2+ plateau, which makes the action potential last longer and prevents muscle cramps (also limits how fast heart rate is)
Ca2+ channels close; slow K+ channels open
stabilized resting potential!
Muscle Action Potential in T-tubule (cardiac muscle)
Action potential enters from adjacent c ell
Voltage-gated Ca2+ channels open → depolarization
Ca2+ induces Ca2+ release via RyR (CARDIAC ONLY)
Ca2+ signal
Ca2+ ions bind to troponin to initiate contraction
Relaxation occurs when Ca2+ unbinds from troponin
Ca2+ is pumped back into SR for storage
Electrical pathway
SA node → internodal pathways → AV node → AV bundle → Bundle branches → purkinie fibers
It gets slower to fire as you go down…
What dominates heart rate?
SA node
this is where parasympathetic and sympathetic work
Conducting system of the heart
SA node depolarizes
Electrical activity goes rapidly to AV node via internodal pathways
Depolarization spreads more slowly across atria. Conduction slows through AV node. (BOOM)
There are not a lot of gap junctions in the AV node → AV node delay → all 4 chambers do not fire at once → prevents accumulation of blood → prevents clot formation/platelets
Depolarization moves rapidly through ventricular conducting system to the apex of the heart
Depolarization wave spreads upward from the apex (BOOM)
ECG
3D signal to 2D surface
electrodes attached to both arms and leg form a triangle
each two-electrode pair (+ and -) constitutes one lead, an ECG is recorded one lead at a time
Lead 2 is the best one to pick up the signal!!!!!
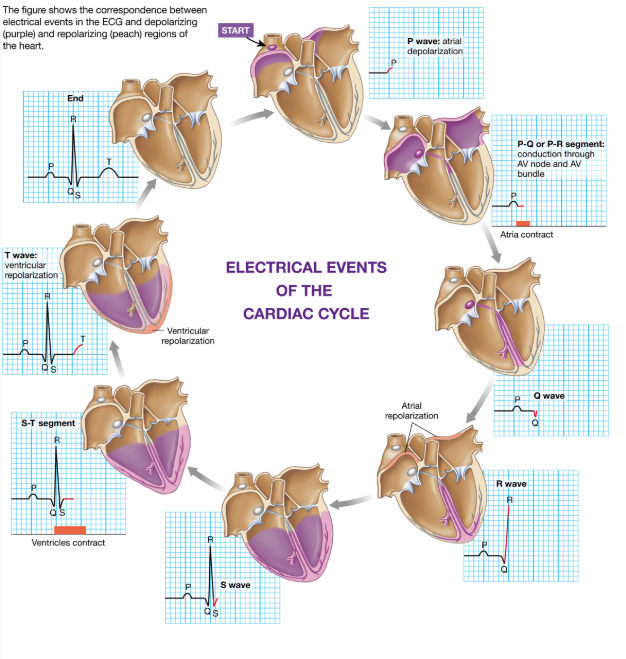
How does an ECG correlate with electrical events in the heart?
P wave = only part from atrium
QRS, T = from ventricle
arrhythmia
abnormal/irregular intervals
heart block
“traffic jam”
partial: longer interval between P and QRS
complete: P and QRS not in synch with more P waves than QRS
atrial fibrillation
p wave different but QRS may or may not be affected
ventricular fibrillation
no QRS and T
= code blue