SOCIAL ANXIETY DISORDER (SOCIAL PHOBIA) AB Psych Chapter 3
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
SOCIAL ANXIETY DISORDER
marked fear or anxiety focused on one or more social or performance situations
Can be anxious in any interaction with people
Can be anxious during specific performance situations in public (Performance Anxiety)
PERFORMANCE ANXIETY
a subtype of SAD; the individual is very anxious only while others are present and maybe watching and, to some extent, evaluating their behavior
Individuals typically have no difficulty with regular social interaction
Anxiety arises when required to perform a specific task in front of others
Focus of fear: possibility of embarrassment
Common Performance Anxiety Situations:
Public speaking (most common)
Eating in a restaurant
Signing a paper/check in public
Physical Symptoms of Anxiety:
Blushing
Sweating
Trembling
For males: Using a public restroom (paruresis or “bashful bladder”)
OLFACTORY REFERENCE SYNDROME
A condition where individuals are preoccupied with the belief that they are embarrassing or offending others due to a foul body odor
Has been reported in North America as well as other regions
Shares features with social anxiety disorder, but more closely resembles obsessive-compulsive disorder (OCD)
Often responds well to psychological treatments used for OCD
CAUSES OF SOCIAL ANXIETY DISORDER
Evolutionary Preparedness
Temperamental Vulnerability
Evolutionary Preparedness
Humans seem biologically prepared to fear angry, critical, or rejecting people
People with SAD are more likely to notice and remember angry or critical expressions
They also show stronger brain responses (e.g., amygdala activation, less cortical control) to threatening faces, especially the eyes
This fear may have evolutionary roots—avoiding hostile or dominant individuals increased survival chances
Temperamental Vulnerability
Some infants are born with a temperament of behavioral inhibition or shyness, evident as early as 4 months old
These infants react more strongly (crying, agitation) to new stimuli
Excessive behavioral inhibition increases the risk of developing phobic behavior and SAD
model of SAD
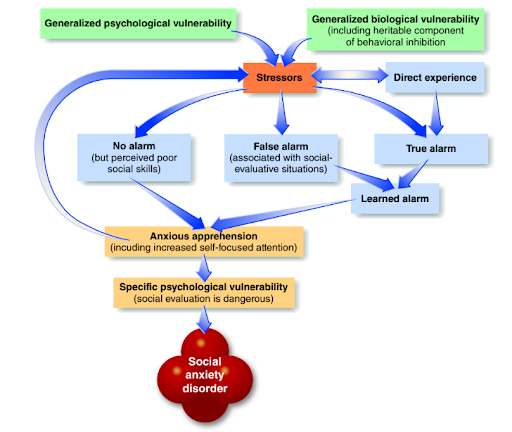
THREE PATHWAYS TO SOCIAL ANXIETY DISORDER
Inherited Vulnerabilities
Conditioned False Alarm
True Alarm (Real Social Trauma)
Inherited Vulnerabilities
Generalized biological vulnerability:
Inherited tendency to develop anxiety
Biological tendency to be socially inhibited
Generalized psychological vulnerability:
Belief that stressful events are uncontrollable
Under stress → anxiety + excessive self-focused attention → disrupted performance
Conditioned False Alarm
Under stress, a person may have an unexpected panic attack in a social situation
This becomes conditioned to social cues
Result: Person grows anxious about future social situations where panic might occur
True Alarm (Real Social Trauma)
Person experiences a real social trauma (e.g., rejection, bullying, humiliation)
Anxiety becomes conditioned in the same or similar social settings
Childhood and early adolescence (ages 12–15) are high-risk periods because of teasing and bullying
Example: 92% of adults with SAD reported severe childhood bullying (versus 35–50% in other anxiety disorders)
ADDITIONAL FACTORS THAT STRENGTHEN SAD
initial pathways explain the onset of social anxiety, but additional factors are needed to show why it persists, generalizes, and deepens into a chronic disorder
Learned Alarm
Anxious Apprehension
Specific Psychological Vulnerability
Family and Genetic Influence
PSYCHOLOGICAL TREATMENTS
Cognitive Therapy
Cognitive Behavioral Therapy
Adolescent Adaptations
Exposure Therapy (Social Mishap Exposures)
DRUG TREATMENTS
Beta-blockers (e.g., Inderal)
SSRIs approved for SAD: Paxil, Zoloft, Effexor
D-Cycloserine (DCS)
SELECTIVE MUTISM
A rare childhood anxiety disorder marked by the consistent failure to speak in specific social situations where speech is expected, despite being able to speak in other settings (e.g., speaks at home but not at school)