WE, Polio, Syringomyelia, and MG
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
Wernicke's Encephalopathy (WE): an acute neurological life-threatening condition caused by __________ deficiency
Thiamine (vitamin B1)
WE: impacts the __________ (central vs. peripheral) nervous system
Central AND peripheral
WE: leads to a triad of symptoms, including __________, __________, and __________
Ophthalmoplegia, ataxia, confusion
what is opthalmoplegia
weakness or paralysis of eye muscles --> nystagmus (most common), conjugate gaze paralysis, pupillary sluggishness, ptosis, anisocoria)
WE: which demographic has a higher incidence?
Developing countries due to malnutrition
how is WE determined
via autopsia
WE: __________ is a PRIMARY cause, but is can also occur w/:
- Severe malnutrition
- Hyperemesis gravidarum (severe N/V during pregnancy)
- Prolonged parenteral nutrition
- Malignancies
- Immunodeficiency
- Liver disease
- Hyperthyroidism
- Severe anorexia nervosa
- Bariatric surgery (due to malnutrition w/ decreased food intake)
Alcohol consumption
WE: why is thiamine, or Vitamin B1, so important?
plays a central role in cerebral metabolism and the Krebs cycle so deficiencies can lead to metabolic imbalances and eventually neuronal death in the mammillary bodies and thalamus
WE: What are some conditions that we should consider in our differential diagnosis? Which condition may occur along WITH WE?
Hepatic encephalopathy, stroke, alcohol withdrawal symptoms (may also be occurring along WITH WE), delirium tremens, chronic hypoxia, normal pressure hydrocephalus
WE: what are other s/s beyond the triad of confusion, ataxia, and ophthalmoplegia?
Delirium, hypotension, peripheral neuropathy, hypotonia, <5% enter level of decreased consciousness leading to death
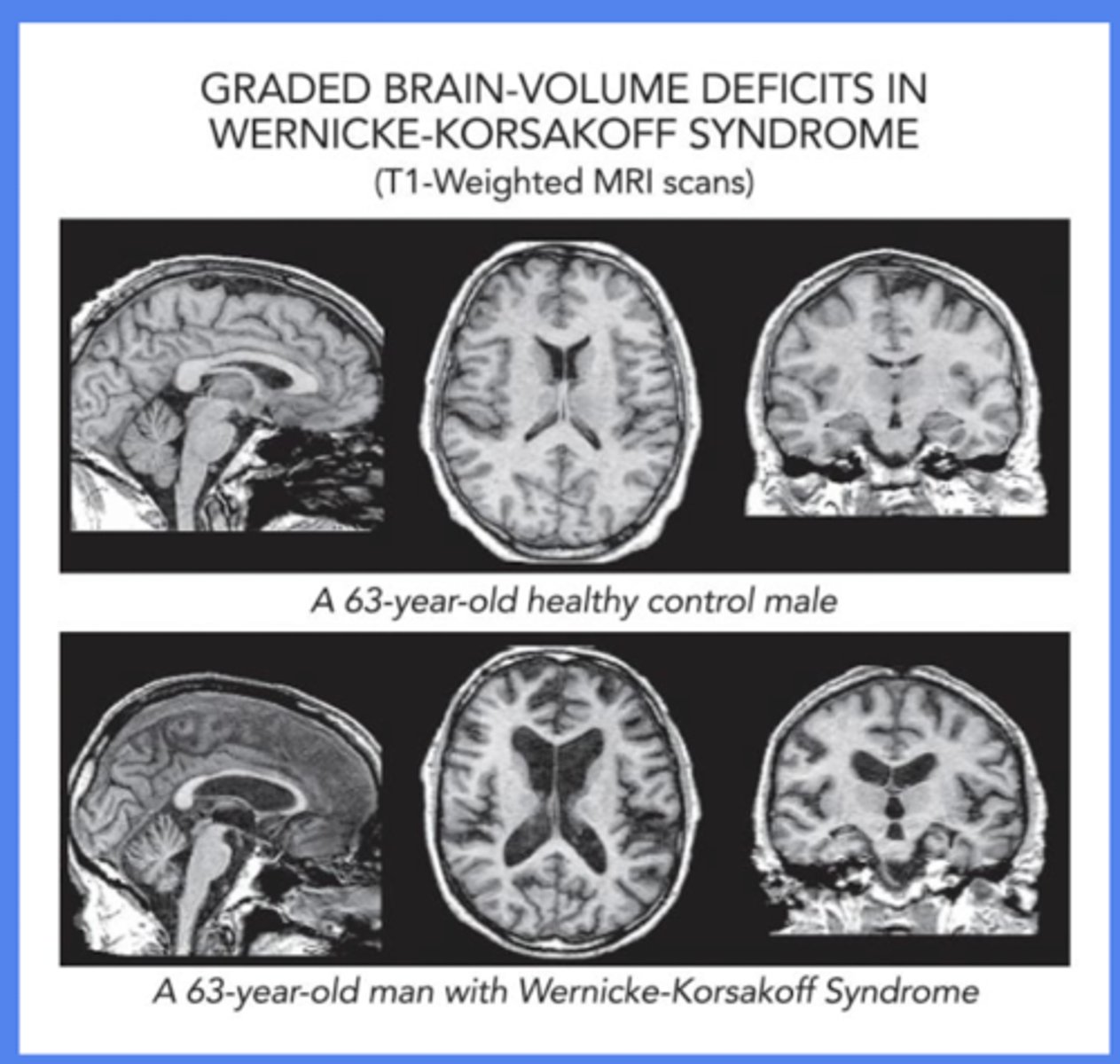
WE: how is it diagnosed?
- clinical presentation (triad + hx of risk factors, including malnutrition, alcohol use, bariatric surgery)
- imaging (MRI findings = lesions in mammillary bodies, periaqueductal area lesions, enlarged ventricles)
- laboratory tests (low thiamine, electrolytes abnormalities)
WE: considered to be an emergent and __________ (reversible vs. irreversible) condition
Reversible
WE: how do we treat it?
Hospitalization for IV thiamine (may need up to 500 mg of thiamine 1-3x/day...may also need a Mg drip as well when alcohol is involved)
WE: what is KEY to treatment?
Prevent chronic status of encephalopathy, as this lead to chronic damage known as Korsakoff Syndrome
WE: PT intervention...when is it safe to see them? What are our next steps?
As mental status improves, appropriate to eval gait needs to get to/from bathroom with nursing --> make suggestions for safety, assist, and assistive devices AS necessary (note: assistive devices tend to do more harm than good w/ ataxia and altered mental status)
Continue to progress gait, strength, balance, and coordination to Mod I
WE: when working with a patient w/ WE, what is ABSOLUTELY essential?
GAIT BELT!!
WE: who is part of the interdisciplinary team?
SLP, OT, nutritionists/ dieticians, social work for discharge planning
__________: neuropsychiatric disorder w/ deficits in anterograde and retrograde memory. May be a consequence of one episode of WE BUT is more typical w/ chronic alcohol use.
Korsakoff Syndrome
KS: severe and often __________ (reversible vs. irreversible) memory impairments
Irreversible
KS: anterograde vs. retrograde amnesia...what do they mean?
Anterograde = unable to form NEW memories, while retrograde = difficulty RECALLING memories
KS: __________: making up inaccurate stories -- brain's way of "filling in the blanks"
Confabulation
KS: besides memory impairments and confabulation, what are some other common s/s?
Hallucination, repetitive speech and/or actions, poor executive functioning (difficulty w/ decision making, planning, or organizing tasks), lack of motivation, emotional apathy
WE vs. KS: acute, reversible neurological condition
Wernicke's Encephalopathy (remember, Korsakoff's Syndrome is a chronic, often irreversible neuroPSYCHIATRIC condition)
WE vs. KS: caused by prolonged or untreated thiamine deficiency leading to PERMANENT damage
Korsakoff's Syndrome (remember, Wernicke's Encephalopathy is caused by thiamine deficiency affecting the brain ACUTELY)
WE vs. KS: classic triad of ataxia + ophthalmoplegia + confusion
Wernicke's Encephalopathy (remember, Korsakoff's Syndrome involves severe memory impairment, confabulation, and apathy)
WE vs. KS: affects the brainstem, mammillary bodies, and thalamus (acute damage)
Wernicke's Encephalopathy (remember, Korsakoff's Syndrome affects the mammillary bodies and thalamus CHRONICALLY)
WE vs. KS: memory deficits are typically PERMANENT despite treatment
Korsakoff's Syndrome (remember, Wernicke's Encephalopathy can improve w/ prompt thiamine replacement)
WE vs. KS: __________ often precedes __________
Wernicke's often precedes Korsakoff's Syndrome (this condition develops as a sequela of untreated WE)
Poliomyelitis aka "Polio" is caused by an __________ from ______ or ________ transmission in humans, and was often transmitted via local swimming areas prior to vaccine
Enterovirus, fecal-oral, oral-oral
Polio: the majority of cases are __________ (mild vs. moderate vs. severe)
Mild
Polio: paralysis occurs in 1/200 when the virus invades the nervous system --> destroying __________ in the spinal cord and __________ in the brain stem
Anterior horn cells, motor neurons
Polio: which type has been FULLY eradicated?
Type 2
Polio: which countries still experience a polio endemic?
Pakistan & Afghanistan
Polio: which demographic is MOST likely to contract the condition?
Children <5, people in developing countries
Polio: what leads to death in individuals?
Respiratory muscle paralyzation -- HOWEVER, this is NOT a high mortality rate (5-10%)
Polio: initial s/s
Fever, fatigue, HA, N/V (i.e., cold or flu-like s/s)
Polio: s/s down the line
Neck stiffness, limb pain, pharyngitis, myalgia, anorexia, severe muscle spasm, asymmetrical flaccid weakness or paralysis
Polio: is it progressive?
NO!!
Polio: explain the five phases
1. widespread denervation of muscle (1 month)
2. Motor neuron recovery and reinnervation (2-12 months)
3. Continued clinical recovery (2-8 years post infection)
4. Functional stability (8-40 years post infection)
5. Late deterioration (8-40 years post infection)
__________: new neuro s/s occurring in polio survivors 15-30 years after initial infection
Post-polio syndrome (PPS)
PPS: true or false...associated w/ severity of polio in initial acute stage
TRUE!! (more likely to have post-polio s/s if experienced bulbar or respiratory involvement; correlated w/ overuse of muscles)
PPS: what is the proposed etiology?
Degeneration of motor neurons due to high burden of surviving anterior horn cells OR increased cytokines from inflammation cause denervation
PPS: what are s/s?
**New onset muscle weakness, **unaccustomed fatigue, joint and muscle pain (nociceptive), decreased endurance, skeletal deformities, muscle atrophy, sleep disorders, difficulty chewing and dysphagia, difficulty emptying the bladder, urinary incontinence, fasciculation, bulbar or respiratory difficulties, cold intolerance
PPS: how do we diagnose it?
NO SPECIFIC TESTS!! Diagnosis of exclusion!! Criteria include: symptoms previously listed, elimination of other causes, prior known hx of polio, initial strength improvements after paralysis, 15 years (avg. 25-35) of stability
PPS: prognosis?
Severe and persistent fatigue BUT highly variable (comorbidities, age, muscle overuse, and weight gain are all factors)
PPS: medical mgmt.?
No medications reverse physiological changes, but we may be able to get symptom relief
PPS: treatment for fatigue
Amantadine, hydrochloride, pyridostigmine bromide, pemoline
PPS: treatment for depression and pain
IV immunoglobin
PPS: surgery for MSK problems
Tendon transfers, muscle transplants, arthrodesis, limb lengthening, joint replacement, etc.
PPS: which three factors most impact happiness?
Age, family, need for assistive technology
PPS: what is absolutely CRITICAL to consider in our interventions?
AVOID OVERWORK WEAKNESS!! (mild to mod activity w/ low reps and sets)
PPS: interventions?
Improve flexibility and endurance, isometric muscle screening, aerobic exercise (reduce fatigue and improve QOL), aquatic therapy (cardiorespiratory fitness), transcranial direct current stimulation (tDCS) for central fatigue
PPS: which outcome measures are appropriate? which outcome measure is TOO fatiguing?
6MWT is fatiguing!! Multidimensional Fatigue Inventory (MFI-20) & Post-Polio QOL are good!!
PPS: which education should we provide?
Lifestyle changes!!
- Frequent rest periods and naps
- Weight loss when appropriate
- Use AD and modalities
- Energy mgmt. techniques
- Exercise modifications: aerobic, ROM, strengthening (combo = BEST)
__________: rare but chronic, PROGRESSIVE disorder of the spinal cord involving a fluid-filled cavity in the spinal cord (Type I-IV)
Syringomyelia
Syringomyelia: involves the development of a fluid-filled cavity or __________
Syrinx
Syringomyelia: where is a syrinx ~typically~ located? What does it push on?
Paramedian in the spinal cord, specifically cervical region --> pushes on grey matter, ascending/ descending tracts and fibers of the lateral spinothalamic tract
Syringomyelia: if the syrinx forms WITHIN the central canal, it is called a __________
Hydromyelia
Syringomyelia: occurs MOST often in which demographics?
Children OR adults 30-40
Syringomyelia: associated w/ which conditions?
Congenital malformation (Chiari malformation), 2nd to SC trauma, result of SC tumors, Klippel-Feil, any disturbances in CSF, hydrocephalus, trauma to cervical region, abnormal cervical spinal canal diameters
Syringomyelia: type _______ (communicating): w/ obstruction of foramen magnum and dilation of central canal
Type I (type A = chiari malformation, type B = other obstructive lesions of foramen magnum)
Syringomyelia: type _______ (noncommunicating): w/o obstruction of the foramen magnum (idiopathic)
Type II
Syringomyelia: type _______: with other diseases of the spinal cord
Type III (type A = SC tumors, type B = traumatic myelopathy, type C = spinal arachnoiditis and pachymeningitis)
Syringomyelia: type _______ (neoplastic cavitation): pure hydromyelia w/ or w/o hydrocephalus
Type IV
Syringomyelia: s/s are DIRECTLY related to the size and location of the syrinx, but typically involves __________
Cape-like loss of pain and temperature along back and arms (aka dissociative anesthesia) --> later development of paresis and muscle atrophy of bilateral hands and arms
Syringomyelia: what are other s/s besides the cape-like loss of pain and temperature along back and arms?
Weakness and ataxia or UE's, HYPER-reflexia, spastic HYPER-tonia, Charcot's joints, hypoesthesia, loss of BB control, HA, inconsistent chronic pain, cerebellar signs (ataxia, dysmetria, dysdiadochokinesia), scoliosis, disc problems/ pinched nerves, fasciculations, paraplegia/ tetraplegia, respiratory failure
Syringomyelia: how do we diagnose it?
Clinical neuro eval + central motor conduction times -- imaging (MRI and CT) WITH clinical screening = optimal diagnosis
Syringomyelia: what are some clinical tests we can integrate for diagnostic purposes? Why do they work?
The Queckenstedt test, Valsalva maneuver, cough test (increase pressure differential in subarachnoid spaces which then elicits patient's symptoms)
Syringomyelia: prognosis?
PROGRESSIVE!! Highly dependent on size and location of syrinx, but early detection for surgical intervention can improve prognosis!!
Syringomyelia: curable?
NO!!--there is ALWAYS a risk it comes back, and it can be therapy resistant when central pain syndrome occurs
Syringomyelia: what is the only viable treatment option?
Surgical intervention to drain or decompress syrinx cavity (w/ diversion of fluid to subarachnoid space or peritoneal cavity), decompress chiari malformation, spinal cordectomy (LAST RESORT, but can improve spasticity, pain, and ascending neuro deficits + QOL), and artificial conduit to reconstruct the CSF channels
Syringomyelia: which type is surgical intervention less effective for?
Type II -- idiopathic in nature w/ no direct cause
Syringomyelia: PT precautions
1. Pain and thermal sensation loss
2. Prevent Valsalva
3. Monitor vital signs
Syringomyelia: PT interventions
1. Functional activities/ADL's
2. Prevention and loosening of contractures and tx of spasticity
3. AD training
4. Balance, coordination, and strength training
5. Pain mgmt. (aquatic therapy)
__________: rare neuromuscular autoimmune disorder that leads to extreme fatigue and profound muscle weakness
Myasthenia gravis (MG)
MG: can impact a person's ability to...
See, swallow, smile, walk, breathe, and/or engage in ADLs
MG: in a normal body, binding of ACh to its receptor activates the muscle and causes a muscle contraction...what happens in MG?
Antibodies (immune proteins produced by the body's immune system) block this activation by either binding to the ACh receptors themselves and/or destroying them --> limits the brain's ability to control muscle movement
MG: type of MG where the cause isn't well understood BUT the likely cause is production of certain types of antibodies
Autoimmune myasthenia
MG: type of MG where a fetus gets certain antibodies from their birth mother who has MG
Neonatal myasthenia
MG: type of MG where it isn't an autoimmune condition and genetic changes are to blame
Congenital myasthenia
MG: which type is MOST common?
Autoimmune
MG: subtype of autoimmune MG that involves the muscles that move your eyes and eyelids --> drooping or inability to keep eyes open, some may have diplopia
Ocular MG
MG: subtype of autoimmune MG that involves muscle weakness that affects your eye muscles AND others in your face, neck, arms, legs, and throat
Generalized
MG: What is the MOST prevalent subtype:
- anti-ACh receptor antibody positive (AChR)
- anti-muscle-specific kinase antibody positive (MuSK)
- anti-lipoprotein receptor-related protein 4 antibody positive (LRP4)
- seronegative MG
Anti-ACh receptor antibody @ 85%
MG: explain the various stages/classes
Class I -- only eye muscles
Class II -- mild muscle weakness
Class III - moderate muscle weakness
Class IV -- severe muscle weakness
Class V -- MG crisis
MG: what are the s/s? (hint: 6x)
Drooping eyelids, double vision, trouble smiling, trouble breathing or swallowing, extremely weak arms, hands, or legs, profound tiredness/ fatigue, impeded mobility and movement
MG: what is the epidemiology?
Young women <40 and older men >60 (more common in adults than children)
MG: is it curable?
NO!!
MG: treatment that involves surgical removal of a particular structure in the body; found to be HIGHLY effective
Thymectomy
MG: treatment that allows ACh to remain at the NMJ for a longer period
Anti-acetylcholinesterase agents (ex: mestinon (pyridostigmine bromide))
MG: treatment that reduces production of autoantibodies
Corticosteroids and immunosuppressants (ex: Prednisone, Imuran, Cellcept, Cyclosporin, Prograf)
NOTE: many steroids and immunosuppressants and infusions are used off-label
MG: list ALL of the methods of treatment (hint: 8x)
1. Thymectomy
2. Anti-acetylcholinesterase agents (Mestinon (pyridostigmine bromide)
3. Neonatal Fc receptor (FcRn) blockers (ex: Vyvgart & Rystiggo)
4. C5 Protein Inhibitors (ex: Soliris, Ultimoris, Zilbrysq)
5. Corticosteroids and immunosuppressants (ex: Prednisone)
6. IV immunoglobulins (IVIg)
7. Rituximab
8. Therapeutic plasma exchange, or plasmapheresis (PLEX)
MG: what factors may cause exacerbation/ worsening of s/s?
Previous deconditioning, fatigue/ intensity/ excessive load/ reps, illness, stress, extreme heat or temp changes, some meds
MG: what is occurring during a myasthenia crisis? which muscle are PRIMARILY affected?
Life-threatening manifestation defined by respiratory insufficiency that requires the use of invasive and non-invasive ventilation as a result of respiratory muscle weakness (could also be due to bulbar weakness w/ upper airway collapse)
MG: approx. 15-20% of patients w/ MG will experience an MG crisi within __________
First 2-3 years
MG: what exam procedures would be useful to assess the s/s of a person w/ MG?
Energy conservation, safety/fall risk, home set-up, life goals, ADL score sheet
MG: what encompasses the ADL score sheet?
Talking, chewing, swallowing, breathing, brushing teeth OR hair, arising from chair, double vision, eyelid droop
MG: which healthcare providers may be indicated to address the deficits experienced?
Occupational & speech therapy
MG: what is the anticipated focus of OT?
Energy conservation, adapt w/ other tools at home, emotional mindfulness (yoga, reduce stress, relax), distal weakness (hands/fingers), adaptive equipment, environmental modifications
MG: what is the anticipated focus of ST?
Breathing strategies/techniques, voice quality, eating/swallowing; dysphonia (change in voice QUALITY), dysarthria (decrease in articulation), dysphagia (swallowing deficits)