regeneration and repair
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
84 Terms
during the early stages (beginning) of inflammation
does repair occur at the end or beginning of inflammation?
replacement of dead cells with cells of the same lineage
what is regeneration?
regeneration
replacement of dead cells with cells of the same lineage is called _______
replacement of dead cells with CT
what is scarring?
scaring
the replacement of dead cells with CT is called _______
regeneration
scaring
when dead cells are replaced with cells of the same lineage, this is called _______.
when dead cells are replaced with CT, this is called _______
soluble factors (everything in the blood)
what factors regulate the processes of regeneration and repair?
extracellular matrix
the ______ is important for repair, and can only heal by scarring if damaged.
soluble factors
regeneration and repair is regulated by ______
no.
the extracellular matrix has the important role.
do WBCs have an important role in regeneration and repair?
-growth factors
-injury
-cell death
-tissue deformation
what can stimulate cell proliferation?
micro
sometimes the presence of the pathogen/etiological agent is not enough to stimulate
the ______environment has an important role in regeneration.
labile tissues
these are tissues that have continuously replicating cells- skin, intestinal lining, etc.
what tissues have the greatest capacity of regeneration?
tissues that have a high capacity of regeneration because their cell population is constantly replicating.
ex: skin, intestinal lining
what are labile tissues?
tissues composed of cells that are at rest (not dividing) in normal circumstances. however, they can replicate in response to a stimulus.
ex: liver
what are stable/quiescent tissues?
labile
their cells are constantly replicating, so they have a high regeneration capacity
the skin and intestinal lining are ______ tissues
stable/quiescent
the cells do not usually replicate, but can replicate in response to a stimulus
the liver is an example of a ______ tissue
tissues composed of cells with no replication/dividing capacity.
ex: heart, brain
what are permanent tissues?
permanent
they are composed of non-dividing cells, so have no regeneration capacity
the heart and brain are _______ tissues
the replacement of tissue components that are identical to those that have died
regeneration is defined as....
regeneration
the replacement of tissue components that are identical to those that have died is called...
compensatory growth- hypertrophy, hyperplasia
what are the types of regeneration that mammals can exhibit?
functional capacity;
original anatomy
with regeneration, the _________ is restored, but the ______ may not be
an intact connective tissue background.
the stroma (extracellular matrix) must not be damaged.
what is absolutely necessary for regeneration to occur?
no, the stroma cannot be damaged.
it also must have an intact CT background.
if a damaged tissue also has their stroma (extracellular matrix) that has been damaged, is it capable of regeneration?
no, the stroma cannot be damaged in order to regenerate.
instead, these lesions will be replaced by CT.
can severe lesions of both the parenchyma and stroma be regenerated?
those with severe lesions of both the parenchyma and the stroma.
they will be replaced by CT
what tissues will undergo scar formation rather than repair/regeneration?
24 hours
-fibroblast migration
-proliferation of fibroblasts and endothelial cells (for blood vessel formation)
repair begins after _____ (time). what is involved in this process?
repair (involves fibroblast migration and proliferation, + proliferation of endothelial cells)
granulation tissue formation (involves proliferation of fibroblasts and neocapillaries + fibrosis)
for a severe lesion of the parenchyma and stroma, after 24 hours, the _____ process will begin.
after 3-4 days, _____ will occur.
3-5 days
-proliferation of fibroblasts and neocapillaries
-loose extracellular matrix of CT forms → fibrosis (scar)
the granulation tissue formation occurs _____ (time) after a severe lesion to the parenchyma and stroma.
what is involved in this process?
1. angiogenesis
2. fibrosis
3. remodeling
healing consists of what 3 components?
the formation of new blood vessels.
the emission of capillary buds through preexisting vessels.
angiogenesis is...
angiogenesis
the emission of capillary buds through preexisting vessels is called ______
1. proteolysis of the basement membrane of the vessel
2. migration and proliferation of endothelial cells
3. maturation and organization of capillary tubes
what are the 3 stages of angiogenesis?
basement membrane of the vessel;
endothelial cells;
capillary tubes
angiogenesis involves the proteolysis of _______.
next, there is the migration and proliferation of _______.
lastly, there is the maturation and organization of ________.
edematous granulation tissue
this is the early stage of tissue, with many blood vessels and rubber texture,
we want this to form because it promotes the growing process.
during angiogenesis, there is a high vessel permeability, which forms......
-basic fibroblast FC (bFGF)
-vascular endothelial FC (VEGF)
what factors regulate angiogenesis?
perpendicular
new vessels always grow ______ to regular vessels
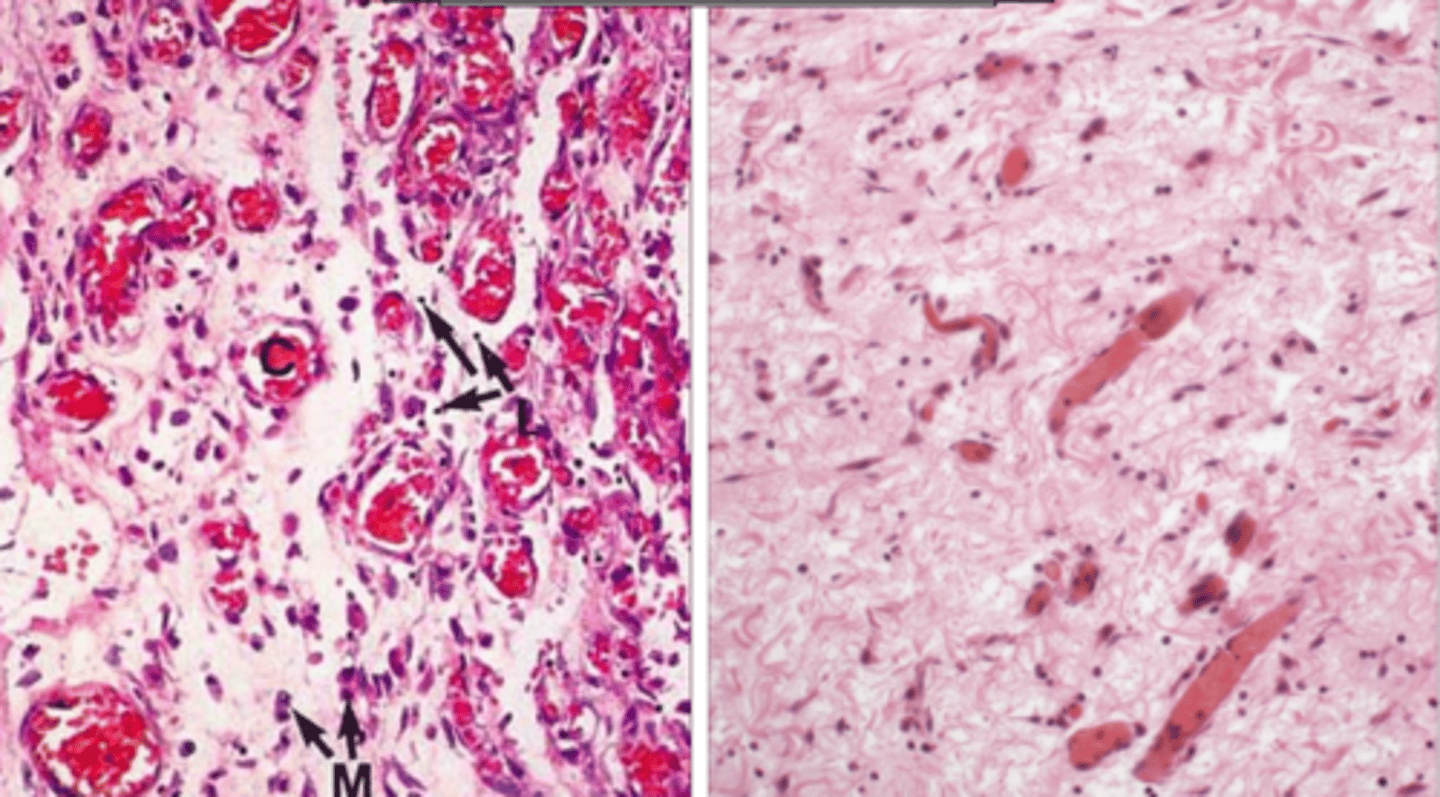
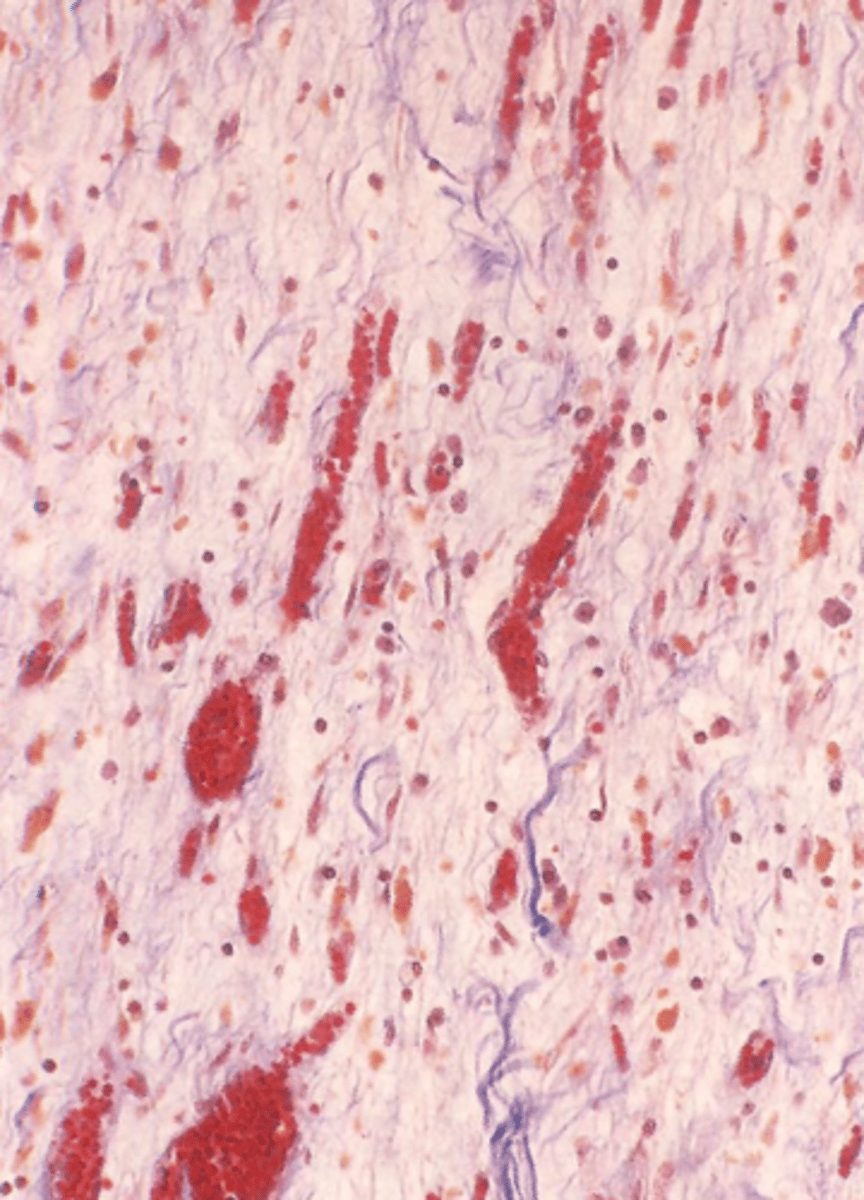
angiogenesis
-inflammatory cells
-not many cells, but lots of fibers separated by edema
what is happening in these 2 images?
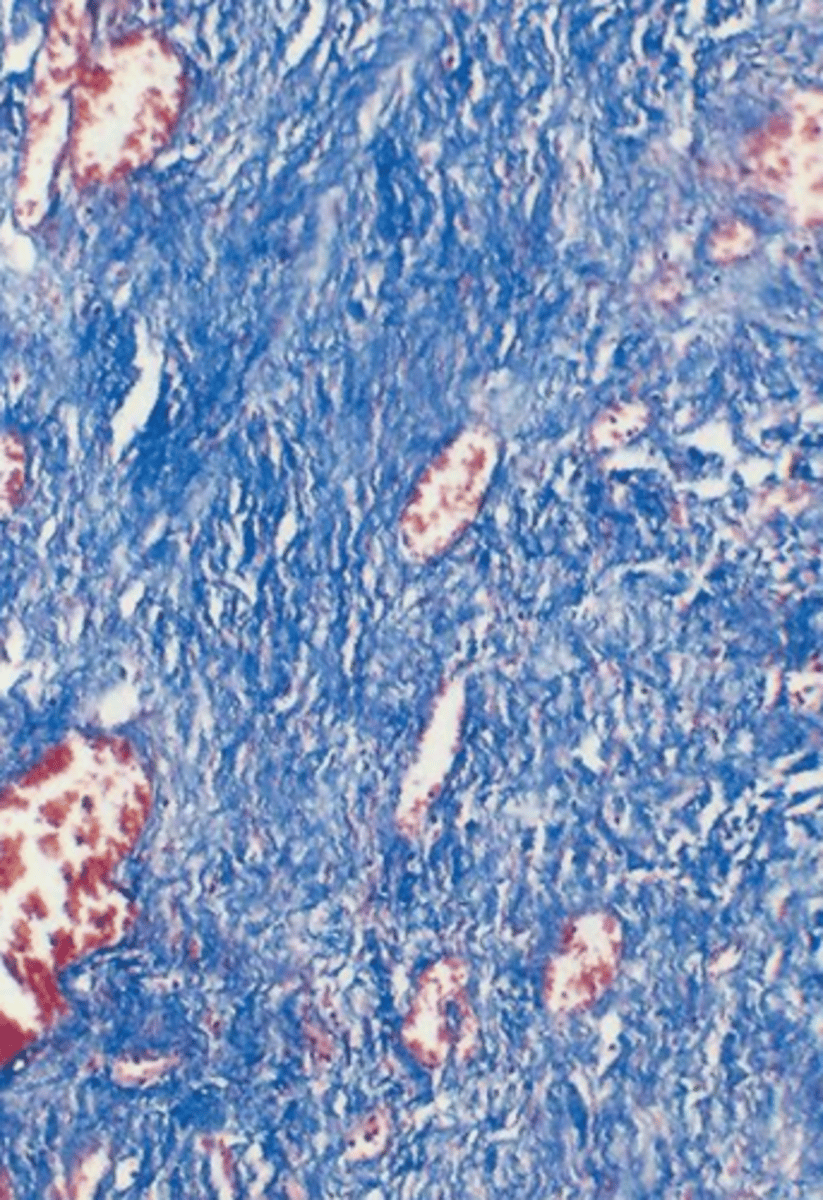
fibrosis
scar formation is called....
on the meshwork of anterior granulation tissue.
it replaces the granulation tissue with fibrous tissue.
where does fibrosis occur?
granulation tissue;
fibrous tissue
fibrosis restores tissue rigidity by replacing ______ with _______
growth factors:
platelet derived GF
basic fibroblast GF
beta transforming GF
these factors are synthesized by activated endothelium and inflammatory cells
for fibrosis, what factors regulate the fibroblast migration and proliferation process?
-fibroblasts
WBCs and fibroblasts regulate this process
for fibrosis, what cells help the deposition of the extracellular matrix?
granulation tissue to scar
scar remodeling is the change from ______ to _______
protease enzyme whose catalytic mechanism involves a metal (Zn2+).
they degrade collagen and other ECM components.
they are produced by fibroblasts, macrophages, neutrophils, synovial cells, and some epithelial cells.
their synth and secretion is regulated by GF, cytokines, phagocytosis, etc.
what are metalloproteinases? what process are they a part of?
to break down the rigid scar tissue structure, to try to recreate some of the original tissue
what is the purpose of metalloproteinases?
metalloproteinases
produced by fibroblasts, macrophages, neutrophils, synovial cells, epithelial cells.
what component breaks down the rigid scar tissue structure, to try to recreate some of the original tissue?
granulation tissue
-fibroblasts
-new blood vessels
-ECM
-inflamm cells
-edema
-collagen
what type of tissue is this?
a type of new connective tissue and microscopic blood vessels that form on the surfaces of a wound during the healing process
what is granulation tissue?
scar tissue
-dense collagen fibers (CT)
-not many cells
-not much vascularization
what type of tissue is this?
scar
granulation tissue becomes ____ tissue when the collagen tissues become more organized and densely packed.
initially eliminate the offending agent.
after, they build a frame work to fill the resulting defect
the cells that reach the focus of reparation do what?
soluble growth factors and the ECM
reparation is a complex set of events directed by the interaction between.....
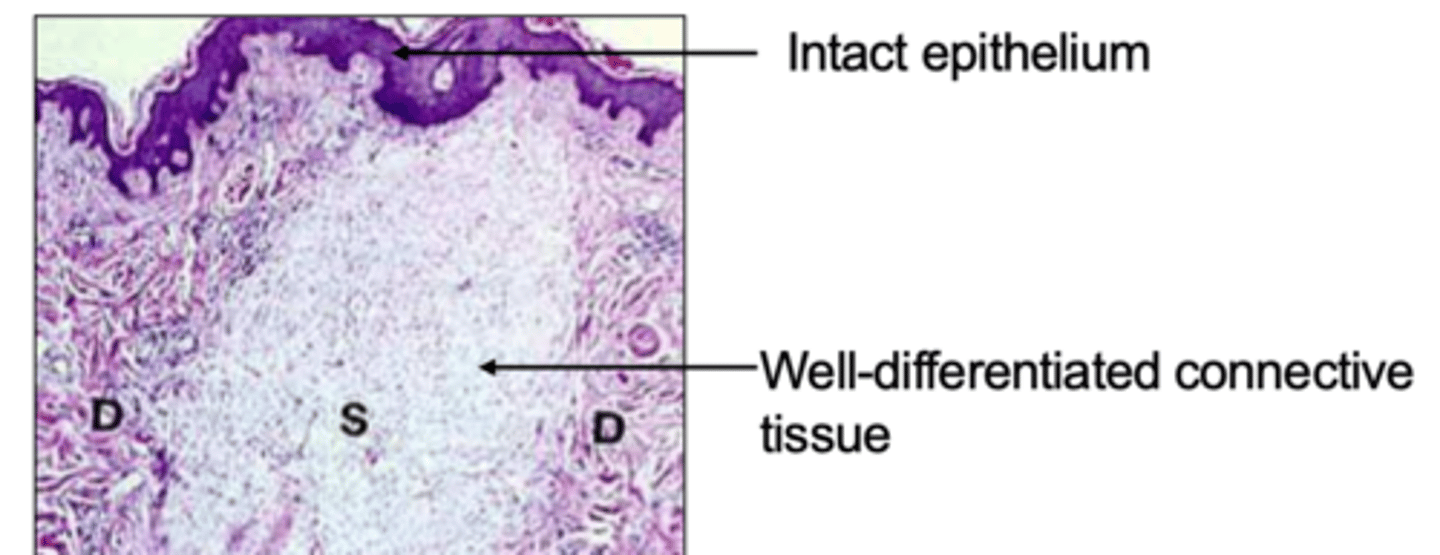
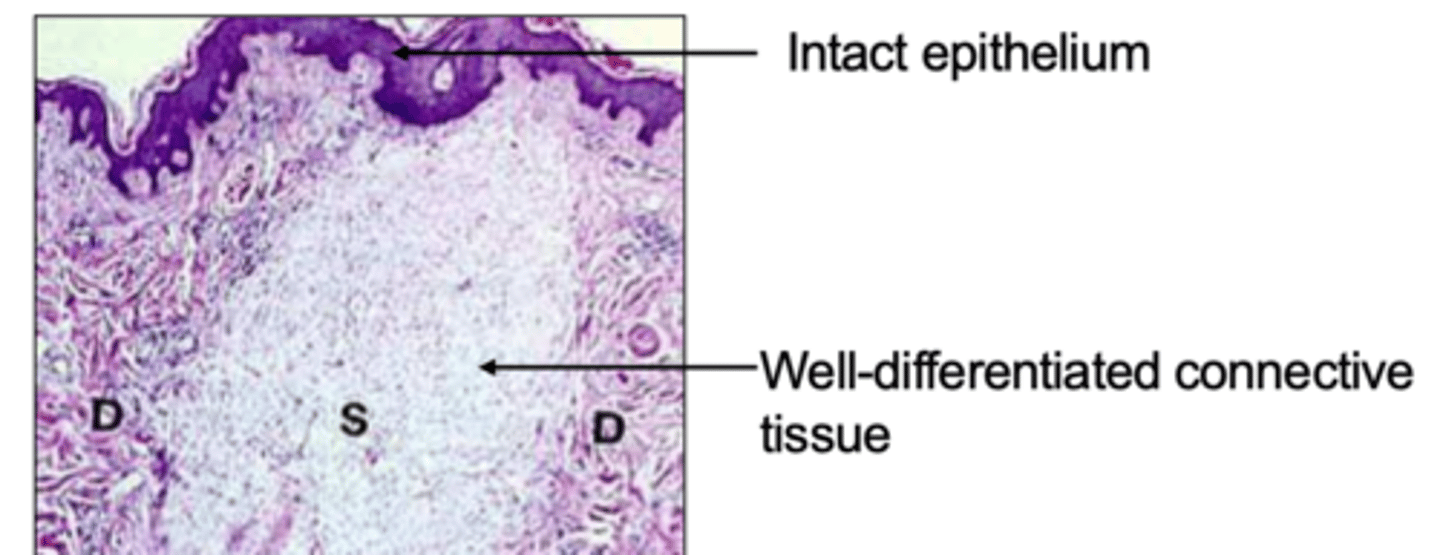
it is the repair of a cutaneous wound, by epithelial regeneration and scarring.
regeneration > repair
-this occurs when there is focal interruption of the basal membrane and there is only death of a few cells and little CT damage.
steps
1. exudative stage (first 24hours)
2. proliferation (day 3)
3. maturation/scar formation (week 2)
describe the process of reparation of a primary intention
primary intention
there will be epithelial regeneration and scarring.
what type of reparation occurs when there is an cutaneous wound, with only focal interruption of the basal membrane and death of few cells and little CT damage?
-fibrin occupies the incision space
-dehydration of the surface → scab
-neutrophils are in the margin
-increased mitosis of epithelial cells
it forms a wet environment that allows the migration of WBCs, cytokines, etc.
this occurs during the first 24 hours after a cutaneous wound
what occurs during the exudative stage of a primary intention?
-macrophages replace neutrophils
-granulation tissue invades incision
-many collagen fibers, which begin to bind the edges of the wound (at 5-7 days)
-continued proliferation of epithelial cells (epidermis recovers its normal thickness)
-lots of CT formation
start of angiogenesis and fibroblast migration.
this occurs 3 days after a cutaneous wound.
what occurs during the proliferation stage of a primary intention?
-accumulation of collagen
-fibroblast proliferation
-WBC infiltrate, edema, and vascularization are ↓
-"whitening" of the scar due to collagen accumulation and capillary regression
-no more fibrin
what occurs during the maturation stage of a primary intention?
-scar made of CT
-no inflamm cells
-normal epidermis
-resistance is increased up to 70-80%
after 1 month of a cutaneous wound, we see....
final stages- 1 month post injury
-no more inflamm cells
-lots of CT where the injury was
what stage of wound healing is this?
primary intention:
cutaneous wound
focal interruption of basal membrane
death of few cells
little CT damage
involves ↑ epithelial regeneration and scar formation (regeneration > scar)
secondary intention:
extensive loss of cells and tissues
scar formation > repair
↑ necrotic debris, fibrin, and exudate
↑ inflamm response
what is the difference between a primary and secondary intention?
regeneration
in a primary intention, which do we see more of, regeneration or scar formation?
scar formation
in a secondary intention, which do we see more of, regeneration or scar formation?
secondary
which- primary or secondary intention, do we see more damage, more exudate, more fibrin, more necrotic debris, and a more intense inflammatory response?
secondary intention
which- primary or secondary intention, results in a bigger area of scar tissue?
secondary
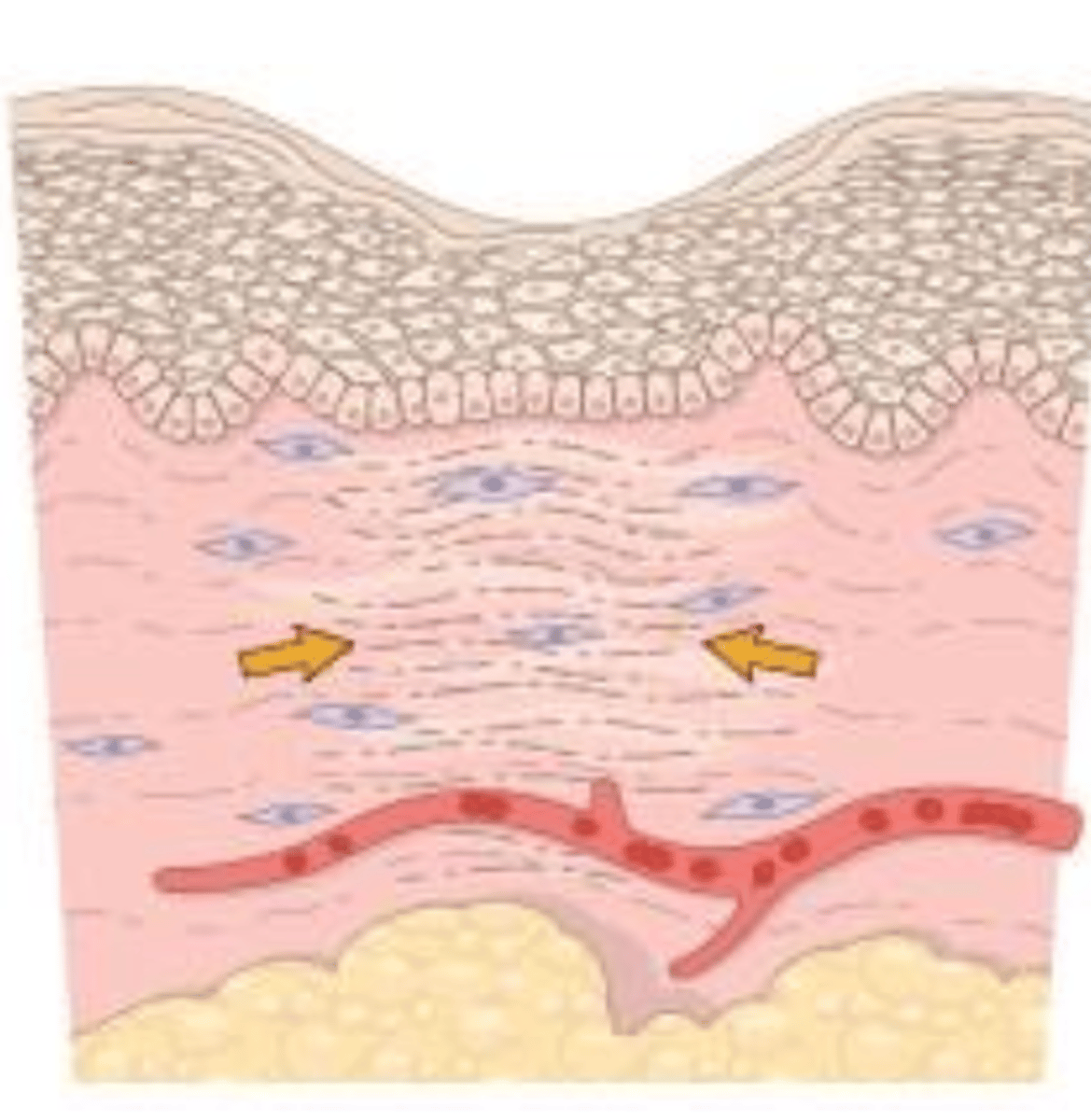
so we will see myofibroblasts
this will reduce the scar 5-10%
wound contraction is seen in _____ intention (primary/secondary)
general:
nutrition: protein deficiencies inhibit collagen synth and delay healing
immune status
circulating WBCs
hormonal factors: glucocorticoids reduce fibrosis, weakening the scar
Local:
infection
mechanical factors: pressure, torsion cause edge separation
foreign bodies: prevent healing
type of injured tissue
location of injury
what factors can influence the reparation response?
inhibits collagen synthesis and delays healing
especially seen with vitamin C deficiency (scurvy)
how does a protein deficiency impact reparation?
they reduce fibrosis, which weakens the scar
how can glucocorticoids impact reparation?
in difficult places to heal, or if there is pressure or torsion, there can be edge separation (dehiscence)
how can mechanical factors impact reparation?
infection
the most important cause of delayed healing is....
they prevent healing
how can foreign bodies impact reparation?
-minimal/absent necrosis
-removal or organization of exudate
-recovery of the normal structure/healing
if after an acute inflammation, there is a quick elimination of stimuli, what occurs?
it is either removed or organized if it cannot be removed completely.
the removal results in the recovery of the normal structure.
the organization results in healing mechanisms, which can be seen as fibrous pericarditis, for example
what happens to the exudate after acute inflammation?
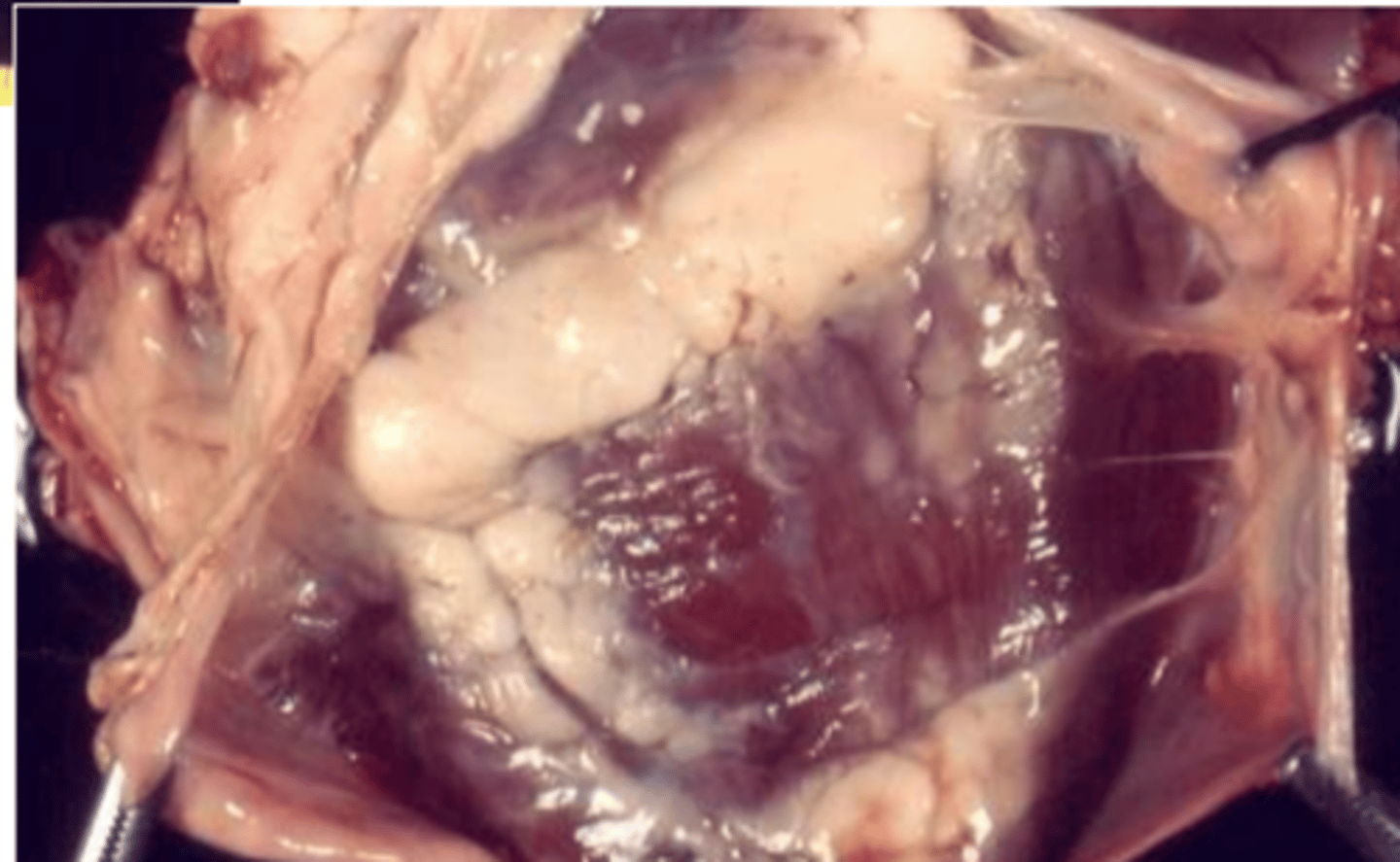
fibrous pericarditis
the exudate of this acute inflammation could not be completely removed, so was instead organized and remains in the pericardium.
what do we see here?
fibrinous pericarditis
the exudate of this acute inflammation could not be completely removed, so was instead organized and remains in the pericardium.
usually fibrinous exudate is in large quantities and cannot be removed completely
what do we see here?
acute
if we see fibrinous exudate, this indicates a _______ inflammation
cellular necrosis
in tissues with permanent cells, this appears as scar formation (ex: myocardial infarct)
in tissues with stable or liable cells, this appears as regeneration and recovery of the normal structure (if the structure remained intact), or as scar formation (if the structure was destroyed)
if there is a slow elimination of stimuli after an acute inflammatory response, what happens?
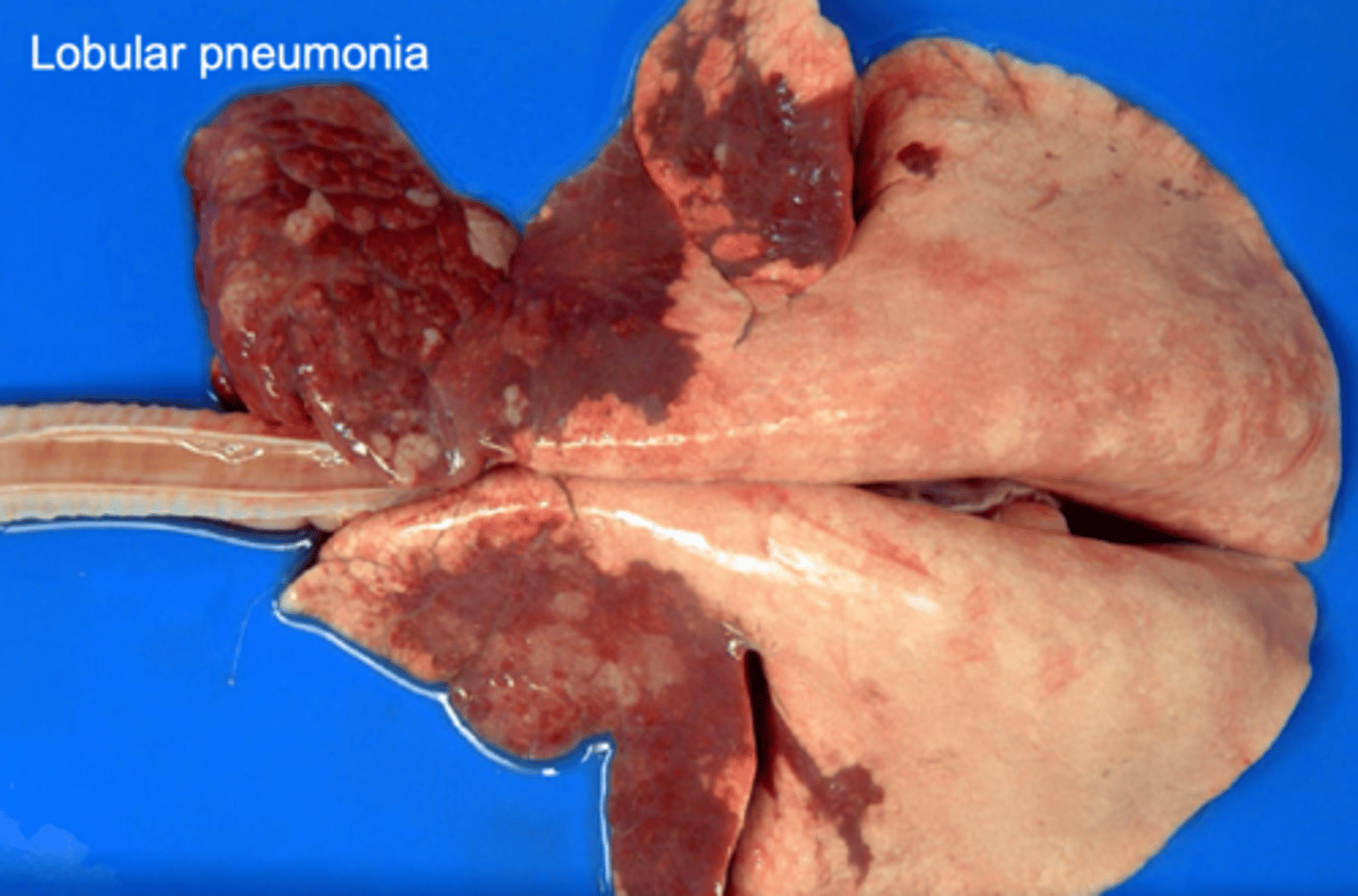
if we recover from this inflammation, we can recover the lung to normal function (unless there is extensive necrosis)
this lobular pneumonia will likely be resolved in what way?
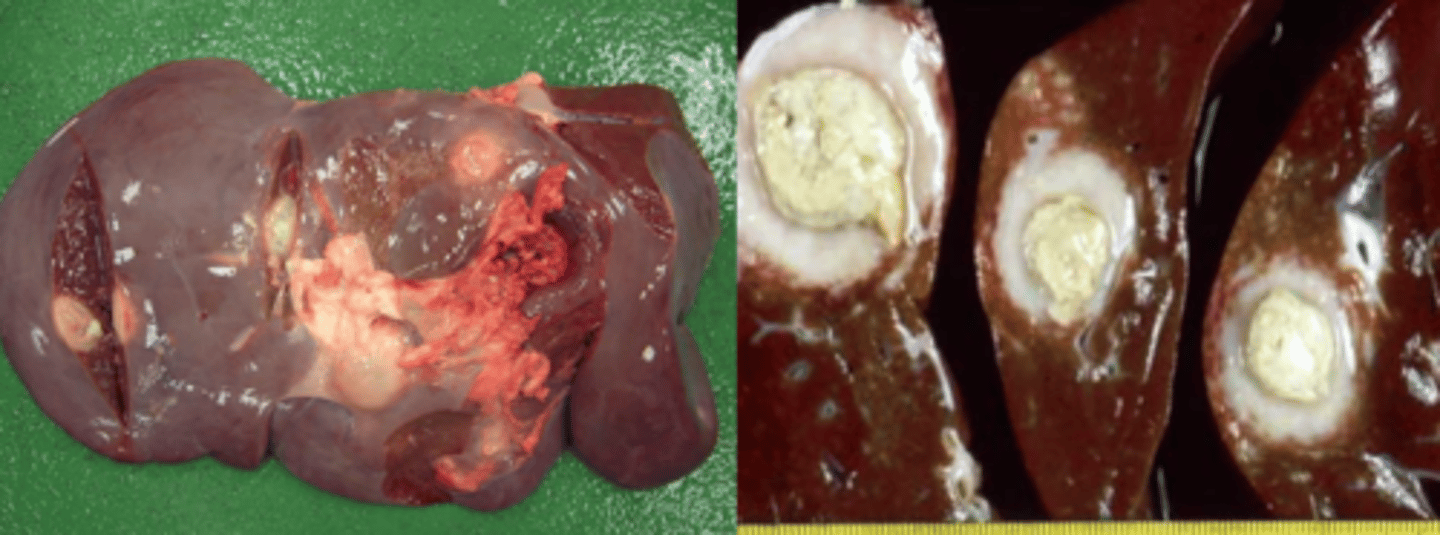
there was too much damage to be repaired, so instead the injury was isolated by encapsulation.
these hepatic abscesses occurred because....
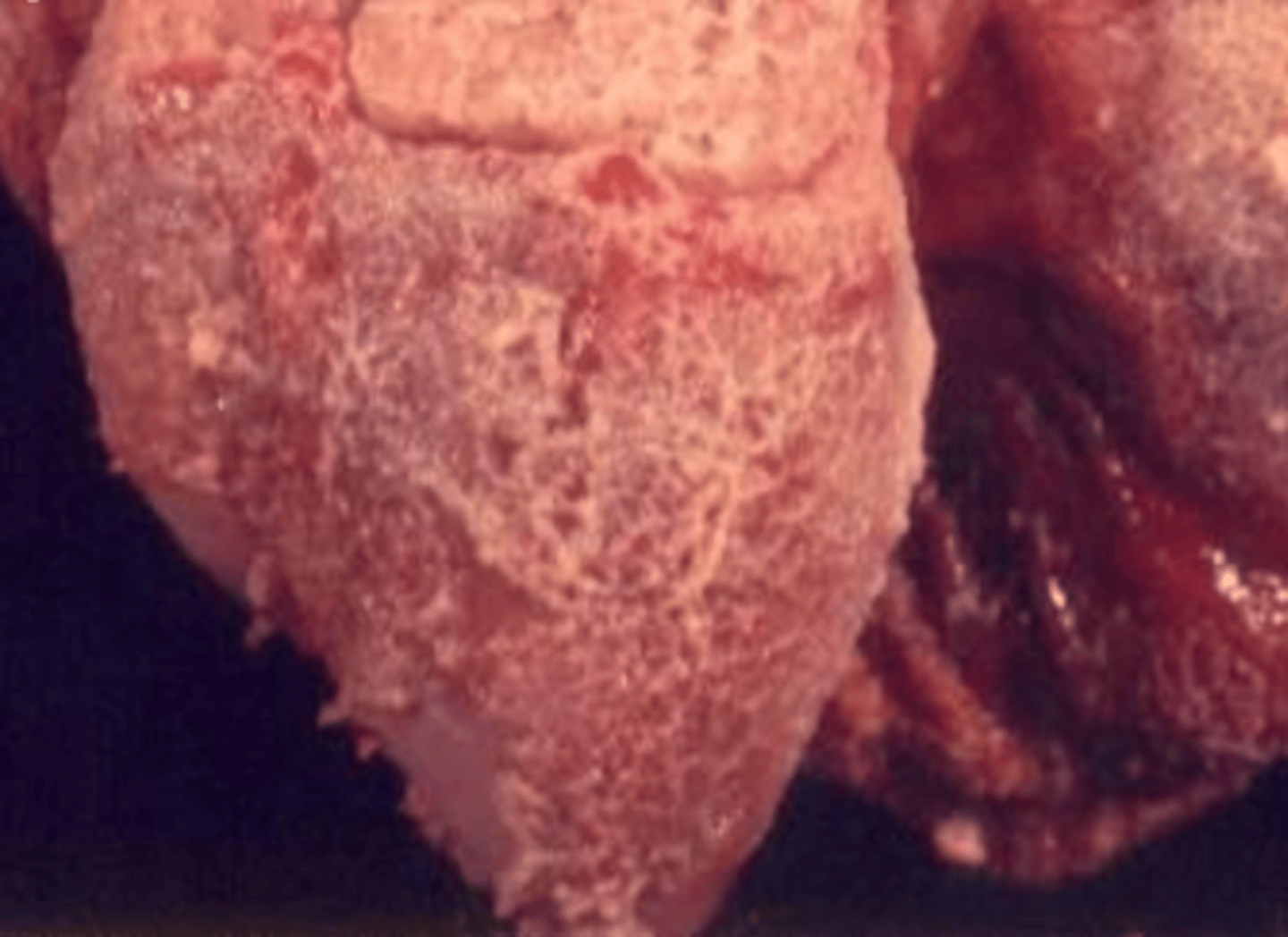
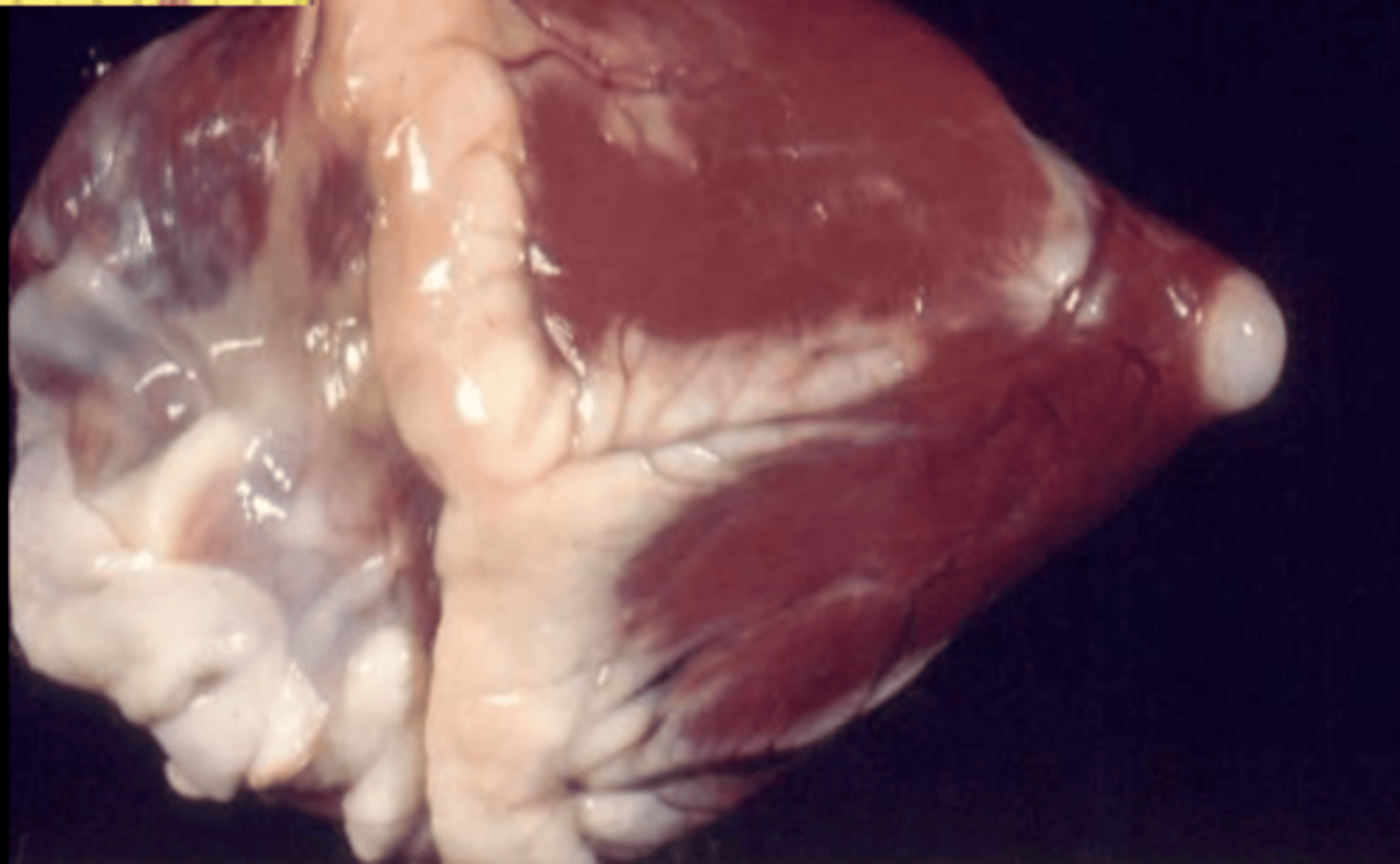
scar tissue (hard+white)
what do we see on this heart?
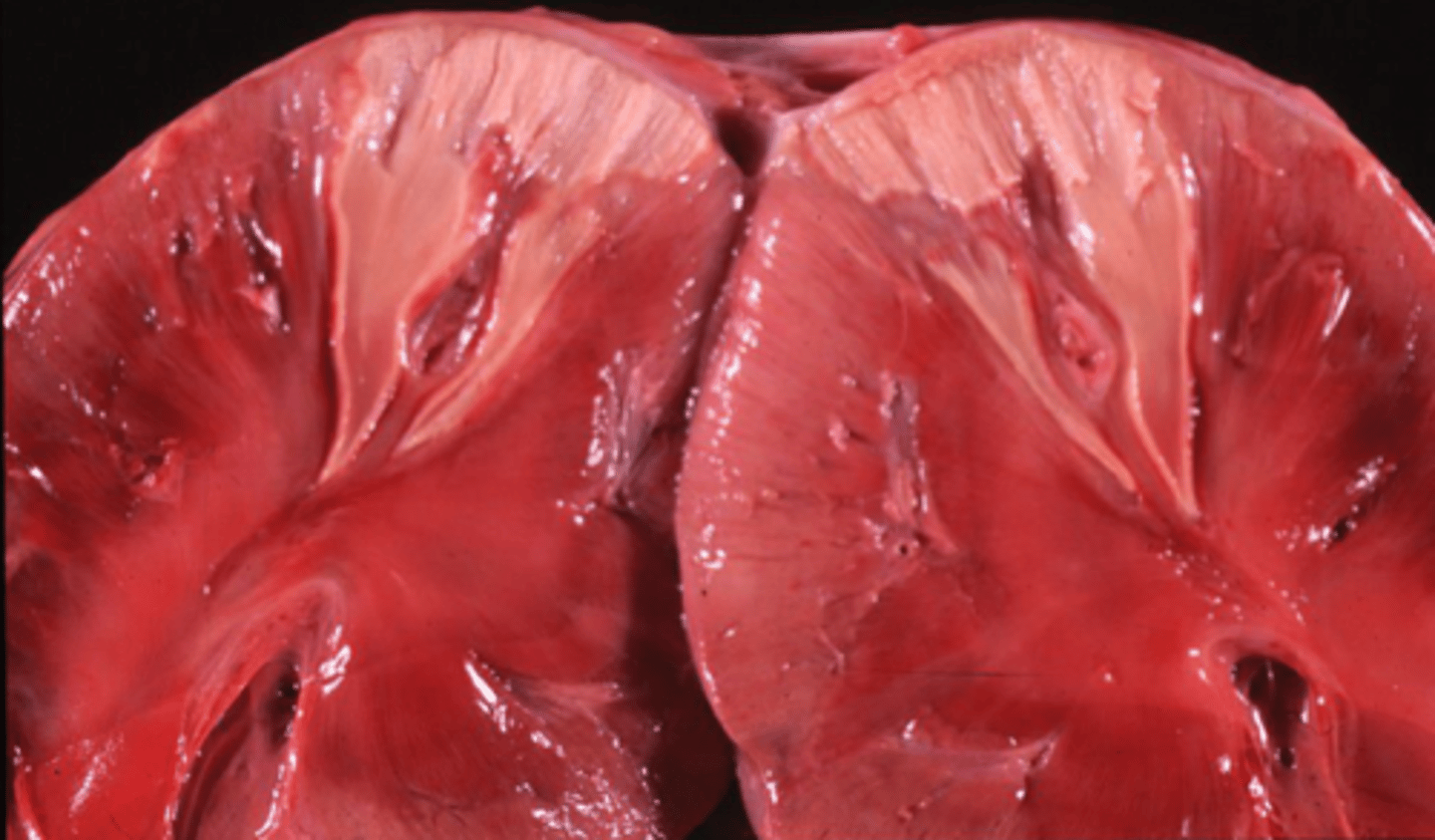
chronic infarct.
at the beginning, it was red+necrotic, but has been replaced with CT, so now is whiter and harder
what happened to these kidneys?
acute
TNF and IL-1 have a bigger impact in ______ inflammation