Looks like no one added any tags here yet for you.
12-Lead EKG
Printout of the heart's electrical activity viewed from 12 different angles as seen in 12 different leads
What is a lead?
electrocardiographic picture of the heart's electrical activity
Rhythm Strip
Printout of only one or two leads at a time
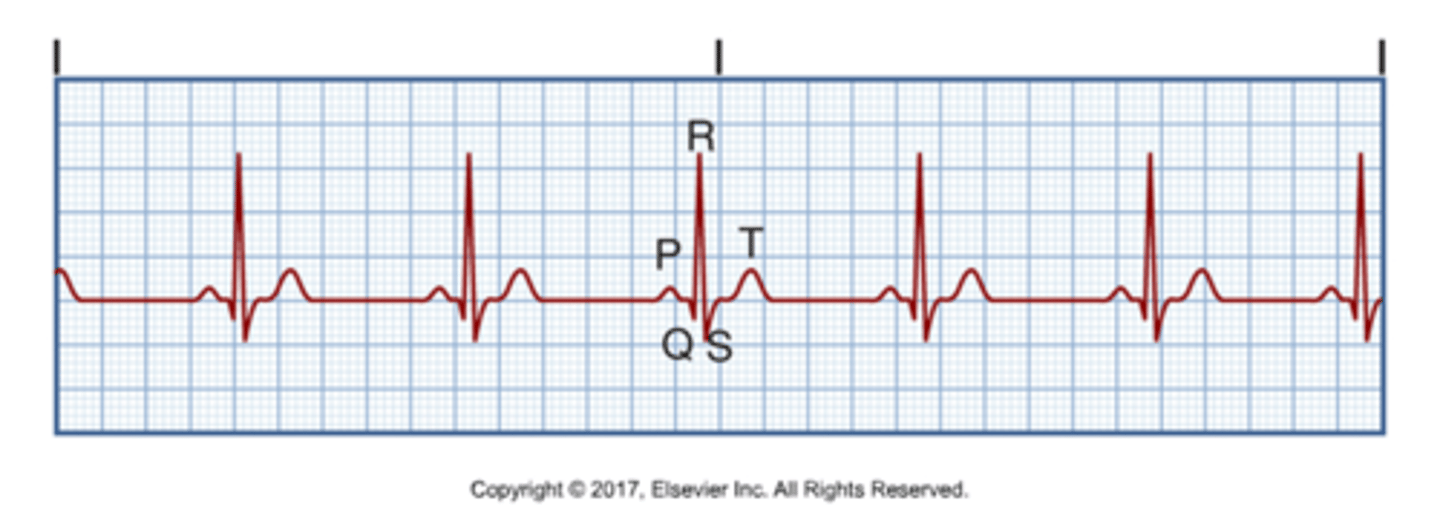
Isoelectric line
Baseline where every wave starts and comes back
Rhythm regularity is determined by
comparing R-R intervals
R-R interval
Distance between consecutive QRS complexes
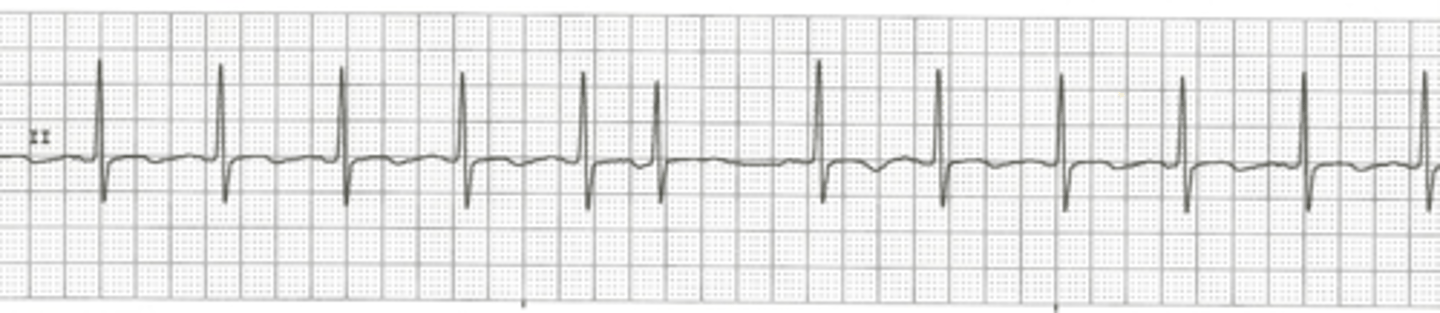
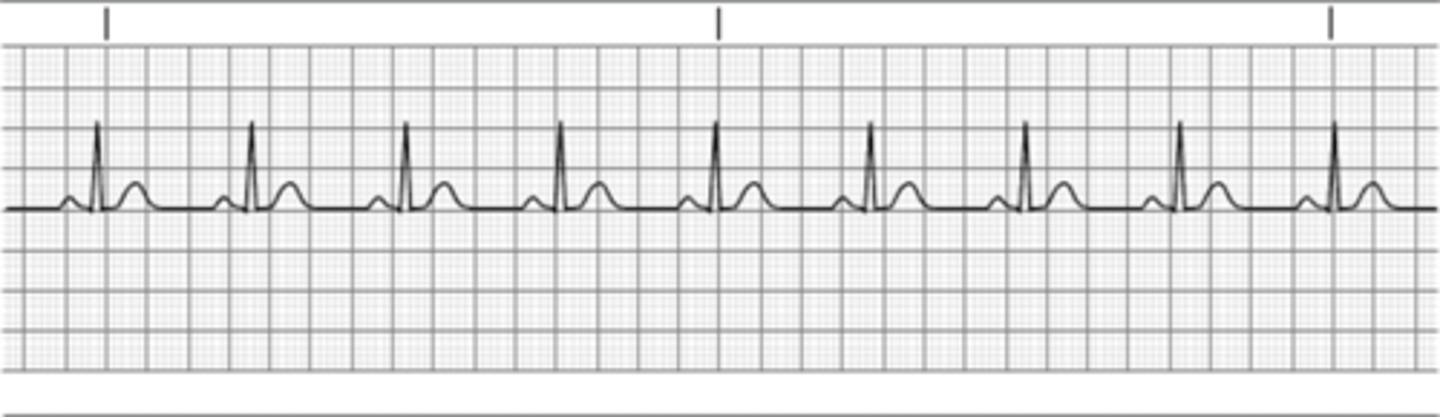
Regular rhythm
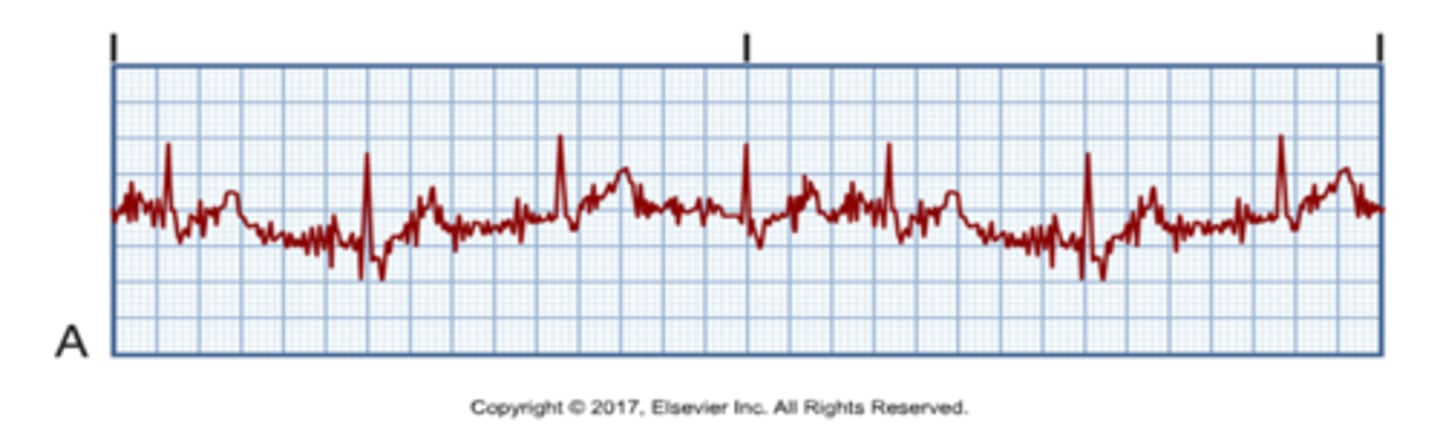
Irregular rhythm (A-Fib)
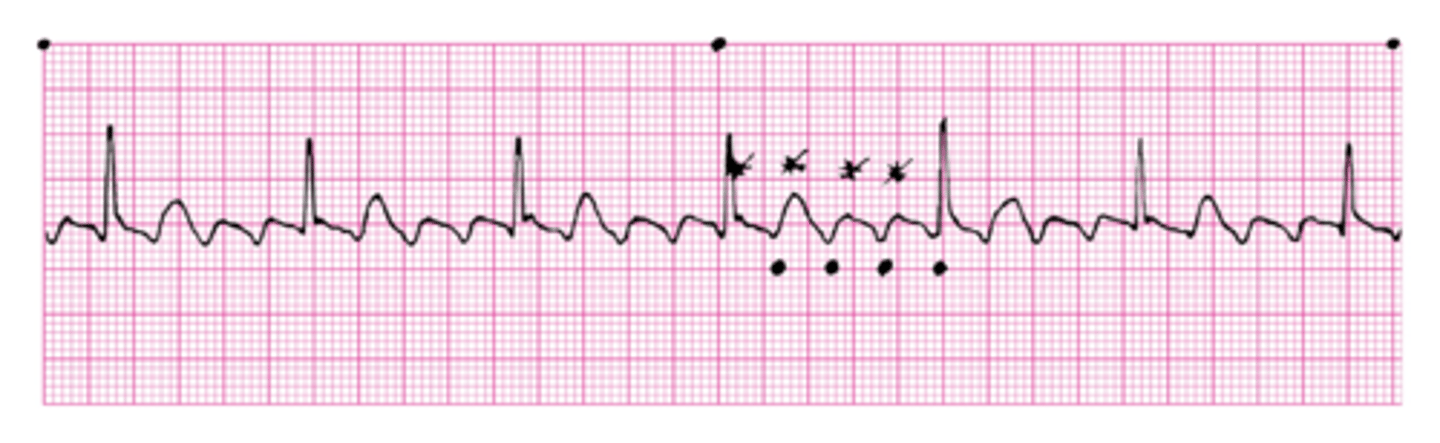
Regular Rhythm w 1 abnormal beat
Regular but interrupted by premature beats
Regular but interrupted by pauses
Artifact (pt could be moving/ coughing)
Heart rate is determined by
# of QRS complexes per minute
Atrial rate is determined by
# of P waves per minute
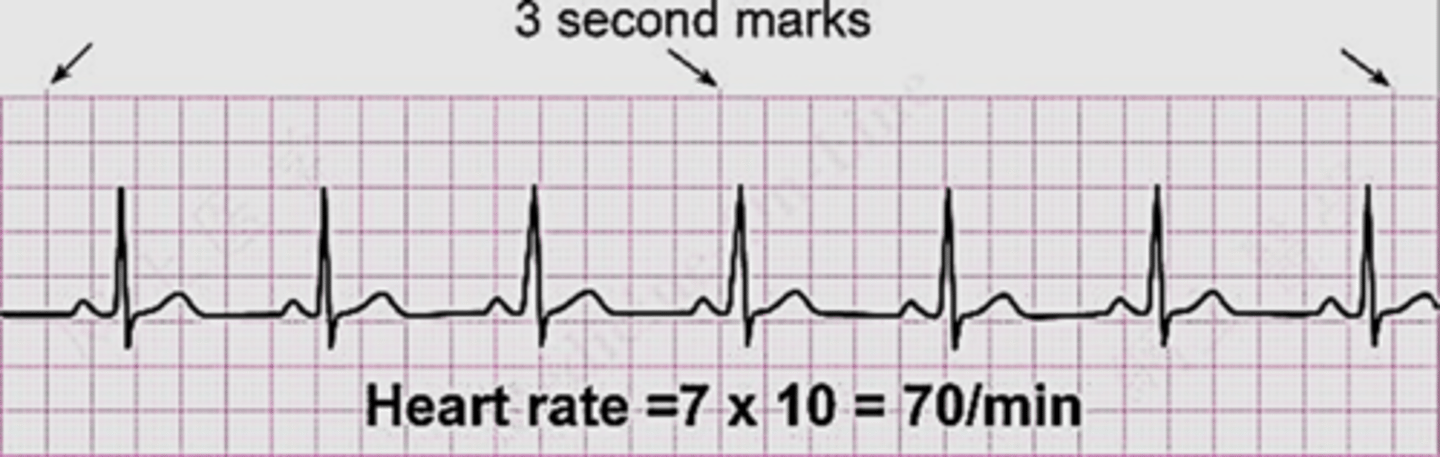
6 second strip method
count the # of complexes within 6 seconds and multiply by 10
Large block method
Count the # of big blocks between QRS complexes then divide into 300.
Ex. 300/3.5= 86
Little Block Method
Count the # of little blocks between QRS complexes and divide into 1500.
Ex. 1500/11= 136
Normal Intervals
PR Interval= 0.12-0.20 secs
QRS Interval= <0.12 secs
QT Interval= 0.34-0.43 secs
Normal Sinus Rhythm (NSR)
Rate: 60-100
P waves: upright, matching previous ones
PR: 0.12-0.20 secs
QRS: < 0.12 secs
Sinus Bradycardia
Rate: <60
Cause: Vagal stimulation of vagus nerve, MI, Digoxin toxicity, well-trained athlete
Manifestations: Dizziness, pallor, weakness, syncope, diaphoresis, hypotension
Treatment: Atropine (if symptoms & given IV), O2, pacemaker, hold and meds that are bradycardia inducing
Anticholinergics (Atropine)
Action: bind w muscarinic receptors to block cholinergic effects on the heart and smooth muscles of the bronchi and intestines
Uses of Anticholinergics (Atropine)
Bradycardia, cardiopulmonary resuscitation
Nursing considerations when giving Anticholinergics (Atropine)
tachycardia, restlessness, irritability, hallucination, delirium, increased intraocular pressure, urinary retention, dilated pupils, decreased salivation and gastric secretions, decreased GI motility
CAN'T SEE, SPIT, SHIT
Contraindications associated with giving Anticholinergics (Atropine)
Given in narrow closure glaucoma, caution with renal and liver dysfunction, and various GI/ intestinal disorders
A patient's cardiac rhythm is sinus bradycardia with a heart rate of 34 beats/minute. If the bradycardia is symptomatic, the nurse would expect the patient to exhibit?
Shortness of breath (SOB)
Sinus Tachycardia
Rate: 101-160
Cause: Atropine, emotions, PE, MI, CHF, fever, vagus nerve inhibition, thyrotoxicosis
Manifestations: Decreased Cardiac Output
Treatment: Treat cause if symptomatic/ at risk for myocardial damage. Vagal maneuvers, consider beta-blockers
Atrial Dysrhythmias are a problem in what wave of an EKG
P wave
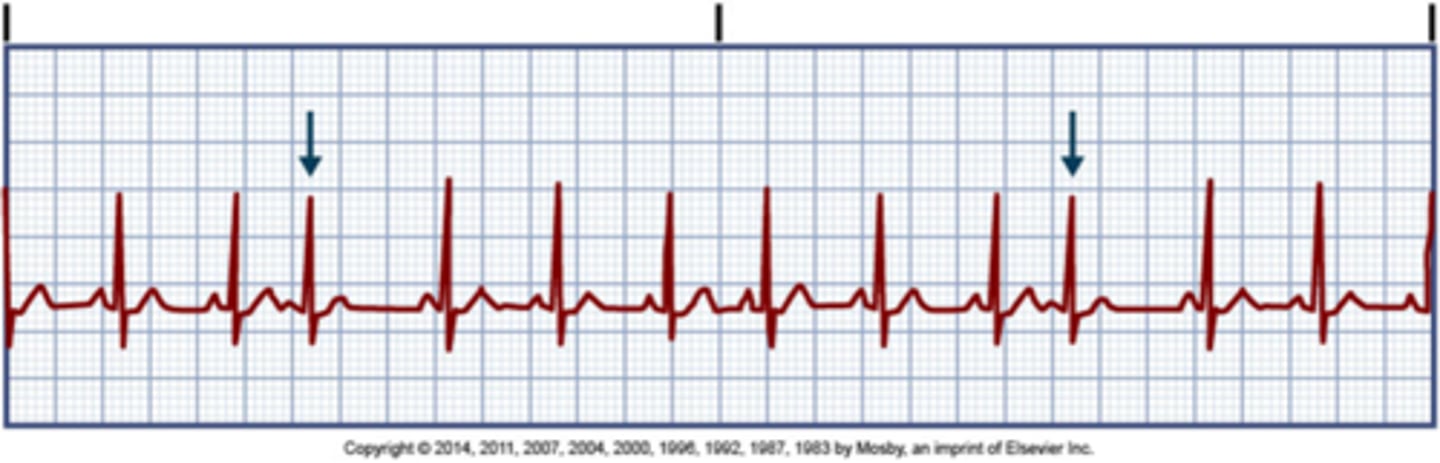
Premature Atrial Contraction (PAC)
Causes: stress, fatigue, caffeine, tobacco, alcohol, hypoxia, electrolytes
Manifestations: palpitations, "skips a beat"
Treatment: monitoring, withhold stimulants, beta blockers
Supraventricular tachycardia (SVT)/ Atrial tachycardia
Rate: 151-220
P waves: differ from NSR P's
Causes: stress, fatigue, caffeine, tobacco, alcohol, hypoxia, electrolytes, digoxin toxicity, heart disease
Clinical significance: Decrease CO, hypotension, dyspnea, angina
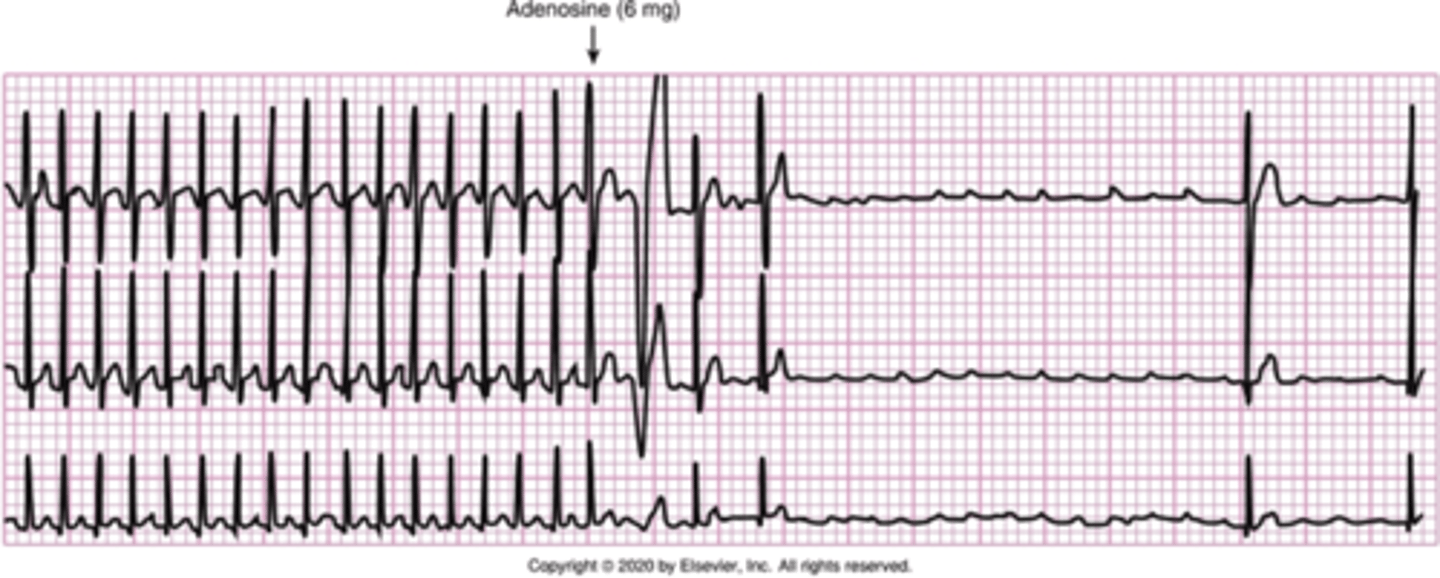
Treatment: Vagal maneuvers, calcium channel blockers, beta-blockers, amiodarone, oxygen, adenosine, cardioversion> ablation.
The primary function of adenosine is
Reset pt. HR and electrocontractility of the heart
Antidysrhythmic meds (adenosine)
Action: slows electrical conduction time through AV node
Uses: SVT
Side effects: Bradycardia or cardiac arrest, tachycardia, facial flushing
How do you administer Adenosine?
Rapid IV push (1-2 secs), followed by rapid normal saline flush, half life= 10 secs
Have crash cart in room with ECG monitoring
Nursing considerations: Monitor ECG continuously
Atrial flutter
Rate: 200-350
Cause: Pulmonary embolus, valvular heart disease, lung disease, thyrotoxicosis, heart failure
Clinical sig: Decreased cardiac output, heart failure, clots
Treatment: calcium channel blockers and/or beta-blockers first, adenosine, antiarrhythmics (amiodarone, flecainide) cardioversion, ablation (tx of choice)
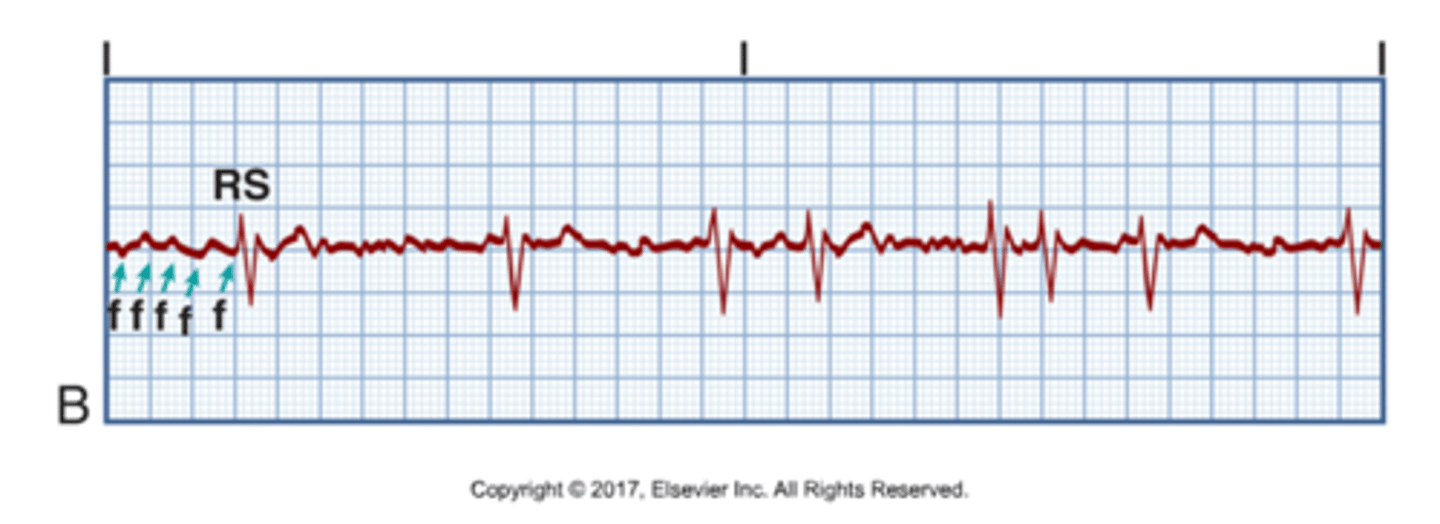
Atrial fibrillation= (irregular/blood clot)
Can be paroxysmal or persistent
Most common type of dysrhythmia
Rate: 350-600
Cause: MI, lung disease, valvular heart disease, hyperthyroidism
Clinical sig: Decreased cardiac output, blood clots causing stroke or pulmonary embolus
If duration <48 hours: Digoxin, calcium channel blockers, beta-blockers, amiodarone, cardioversion
If duration >48 hours: Anticoagulation , TEE, cardioversion
Cardiac Glycosides (Digoxin)
Digoxin
Action: Positive inotropic effect (increases contractility) & negative chronotropic effect (decreases HR) causing an increase in cardiac output (CO)
Use: CHF & Atrial dysrhythmias (Atrial Fib, atrial flutter)
Side effects of Cardiac Glycosides (Digoxin)
Nausea
Loss of usual appetite
Headache
Administration consideration for Cardiac Glycosides (Digoxin)
Never give IM: can cause tissue irritation/sloughing
Watch for Digoxin Toxicity
Lots of drug interaction
Cardiac Glycosides (Digoxin) toxicity increases with?
Hypokalemia
Signs & Symptoms: Headache, Visual disturbances, Nausea, Diarrhea, Vomiting
Nursing care for someone who is taking Cardiac Glycosides (Digoxin)
Assess BP, HR, ECG
Assess serum drug level
Monitor K, Mg, Ca levels
Monitor I&O along w daily weights
Teach S&S of toxicity
Potassium Channel Blocker Antidysrthmic (Amiodarone)
Action: Blocks potassium from re-entering cell to repolarize causing a prolonged refractory period and decrease automaticity
Uses: Vtach, Vfib, SVT, Atrial Fib, Atrial Flutter
Side effects: dizziness, fatigue, hypotension, bradycardia, nausea/vomiting, ataxia, paresthesia
How to administer Potassium Channel Blocker Antidysrthmic (Amiodarone)
May take with food (stay consistent if you take it w food or not)
Avoid grapefruit juice and direct sunlight
Avoid alcohol, caffeine, and tobacco
Nursing Considerations for Potassium Channel Blocker Antidysrthmic (Amiodarone)
Monitor BP, HR, and ECG
Monitor liver and thyroid function
Assess for pulmonary & neuro toxicity
Report HR <60
Ventricular dysrhythmias
HR ranges 0-250
Most lethal of all rhythms
Most will cause symptoms of decreased cardiac output
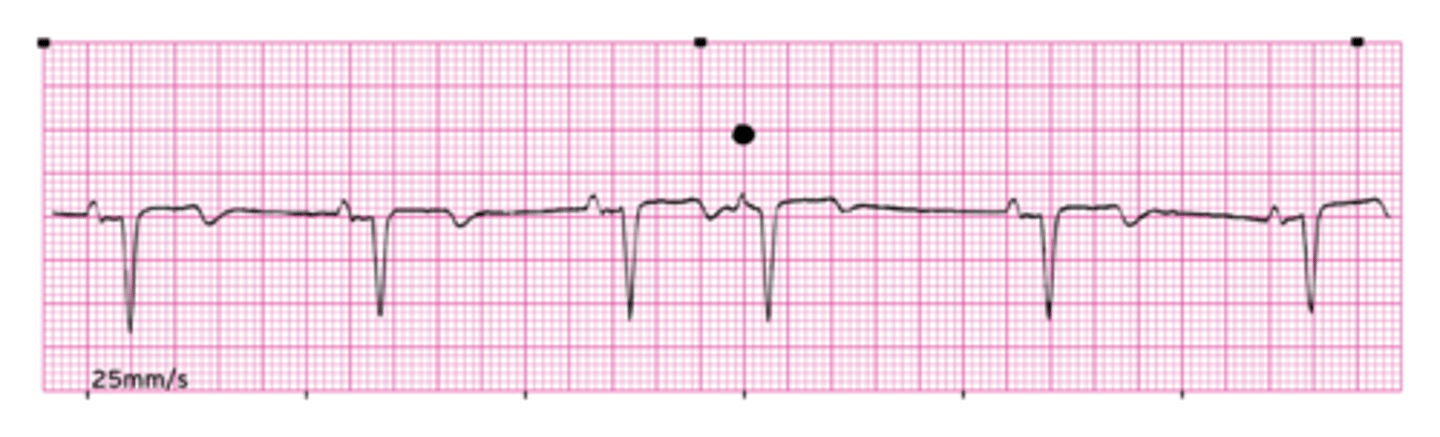
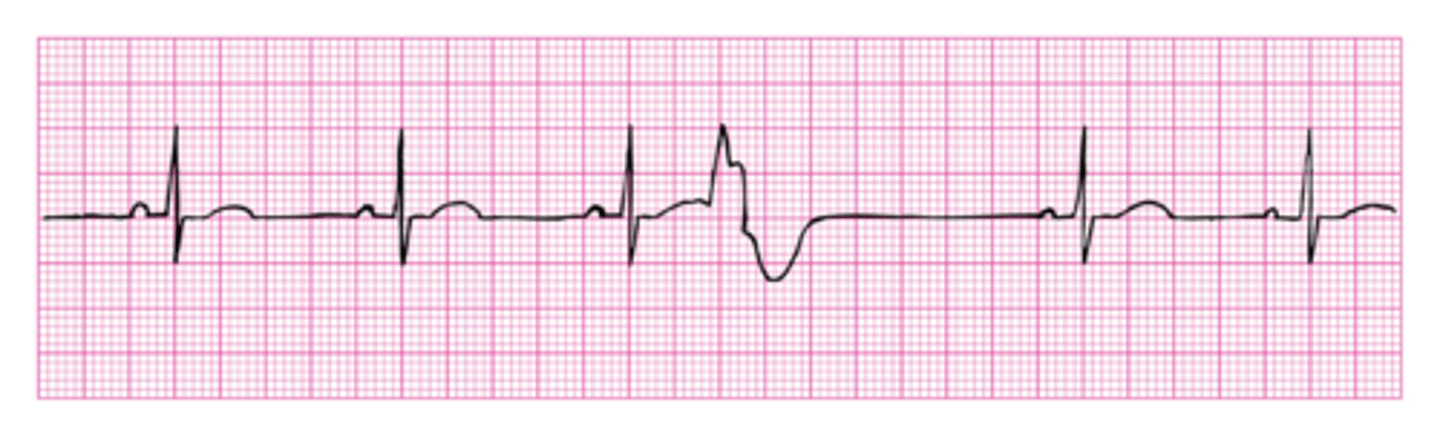
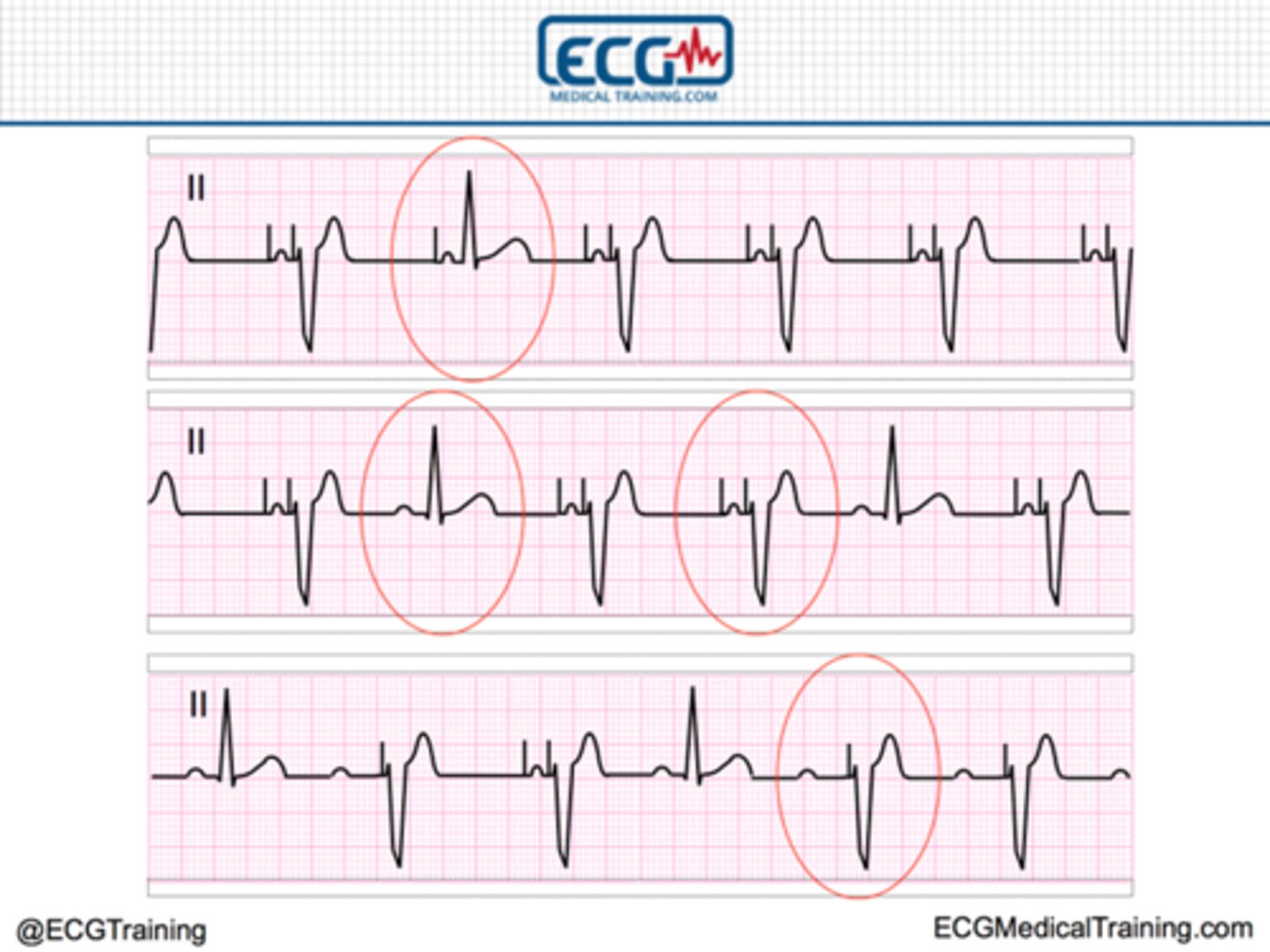
Premature ventricular contraction (PVC) (AKA: BIG NASTY)
Ventricular bc QRS is affected
Cause of Premature ventricular contraction (PVC) (AKA: BIG NASTY)
Heart disease, hypokalemia, hypoxia, hypomagnesemia, stimulants, caffeine, stress
Clinical Sig: reduced CO, angina
Treatment for Premature ventricular contraction (PVC) (AKA: BIG NASTY)
Treat cause (supplemental oxygen/potassium), amiodarone, procainamide, beta blockers
A patient has a diagnosis of acute myocardial infarction, and his cardiac rhythm is sinus bradycardia with 6 to 8 premature ventricular contractions (PVCs) per minute. The pattern that the nurse recognizes as the most characteristic of PVCs is ?
A wide, distorted QRS complex
Monomorphic ventricular tachycardia
QRS complexes that are the same shape, size, and direction
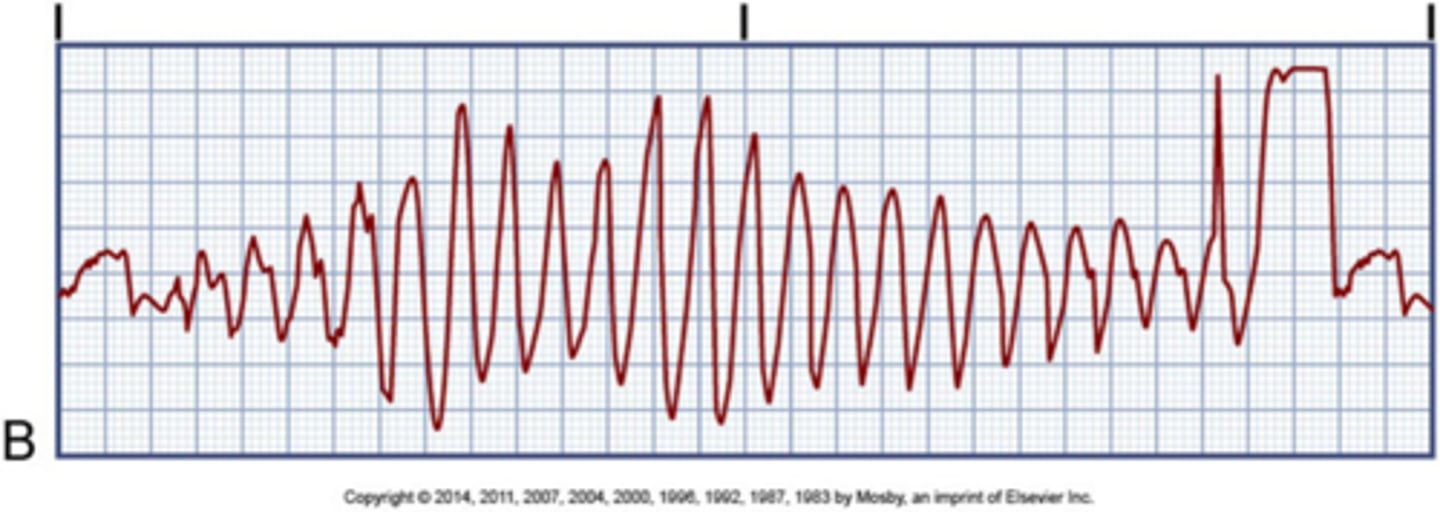
Polymorphic Ventricular Tachycardia (Torsades de Pointes)
constant change on QRS complex (usually Mg problem)
Causes of Ventricular Tachycardia
MI, CAD, hypoxia, hypokalemia, hypomagnesemia, stimulants
Clinical Sig: pulse (stable VT) or no pulse, Dec CO, Shock, unconsciousness, death
Treatment for Ventricular Tachycardia
Treatment w pulse: procainamide, amiodarone, lidocaine
Treatment wo pulse: CPR & rapid defibrillation (only if DEAD)
Treatment for Polymorphic VT: Mg, isoproterenol, cardioversion
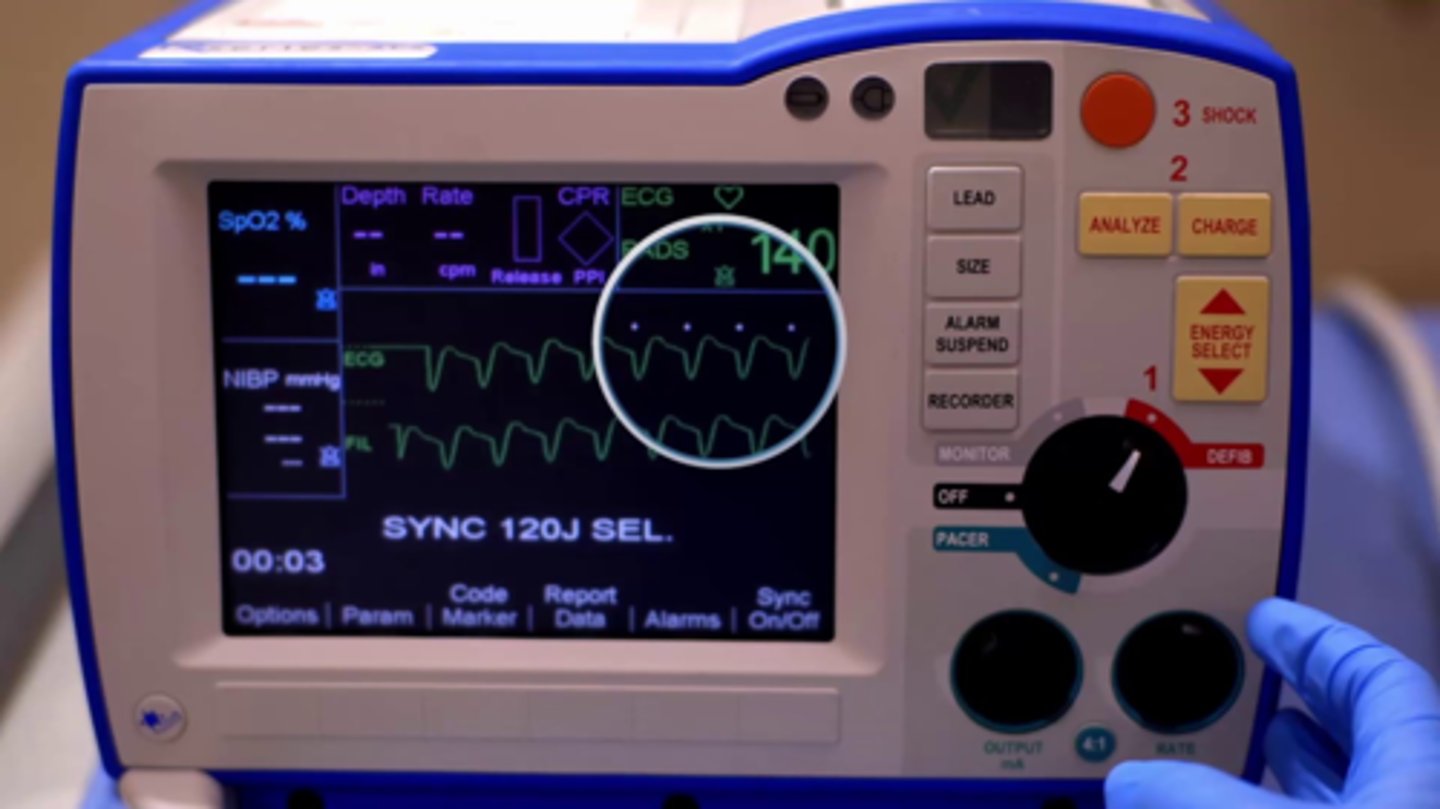
Cardioversion (MUST HAVE A PULSE)
Used for supraventricular dysrhythmias and VT w pulse
Usually small shock w less electricity bc pt is alive
Requires synchronization w cardiac cycle= must have PULSE
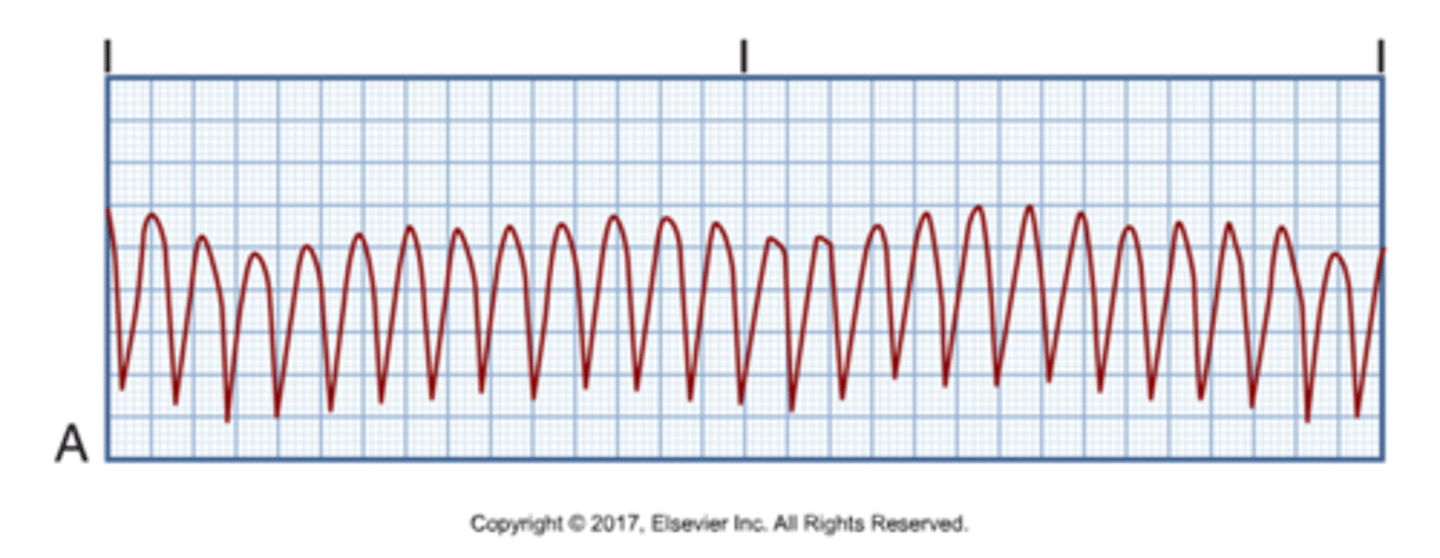
Ventricular fibrillation
Pulseless, unresponsive, apneic (death if untreated)
Cause of Ventricular fibrillation
MI, hypoxia, hypokalemia, hyperkalemia, drowning, OD, accidental electric shock
Treatment for Ventricular fibrillation
Immediate CPR, defibrillation, epinephrine, amiodarone, oxygen
Defibrillation (MUST BE PULSELESS)
Larger shock= more electricity
NOT synchronized
Treatment of choice for Vfib and pulseless Vtach
3 ways to deliver a shock
1. Monitor/defibrillator
2. AICD (implanted)
3. AED
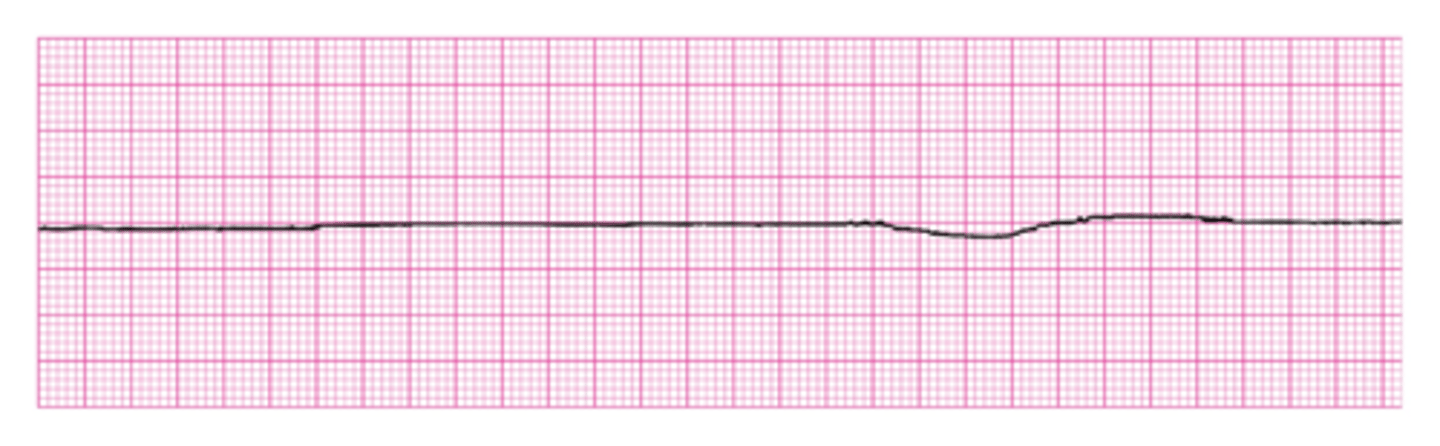
Asystole (pulseless & DEAD)
Pt. is dead but must go in room to verify
Cause and treatment for Asystole
Cause: Hypoxia, advanced cardiac disease, severe cardiac conduction problem, end stage heart failure
Treatment: CPR, epinephrine, O2
Pulseless Electrical Activity (PEA)
Electrical activity can be observed on the ECG, but no mechanical activity of the ventricles is evident, pt has no pulse
Poor prognosis unless underlying cause is quickly identified and treated
Pacemakers
Electronic devices implanted into or attached to a patient
Sends out electrical signal causes heart to depolarize
Used to maintain reasonable HR in pt who's HR is too slow
Can pace atrium, ventricle, or both
Indications for pacemakers
Symptomatic sinus bradycardia
Junctional rhythms
Slow ventricular rhythms
AV blocks
Tachydysrhythmias
3 ways to pace w a pacemaker
1. Transcutaneous pacing (thru skin)
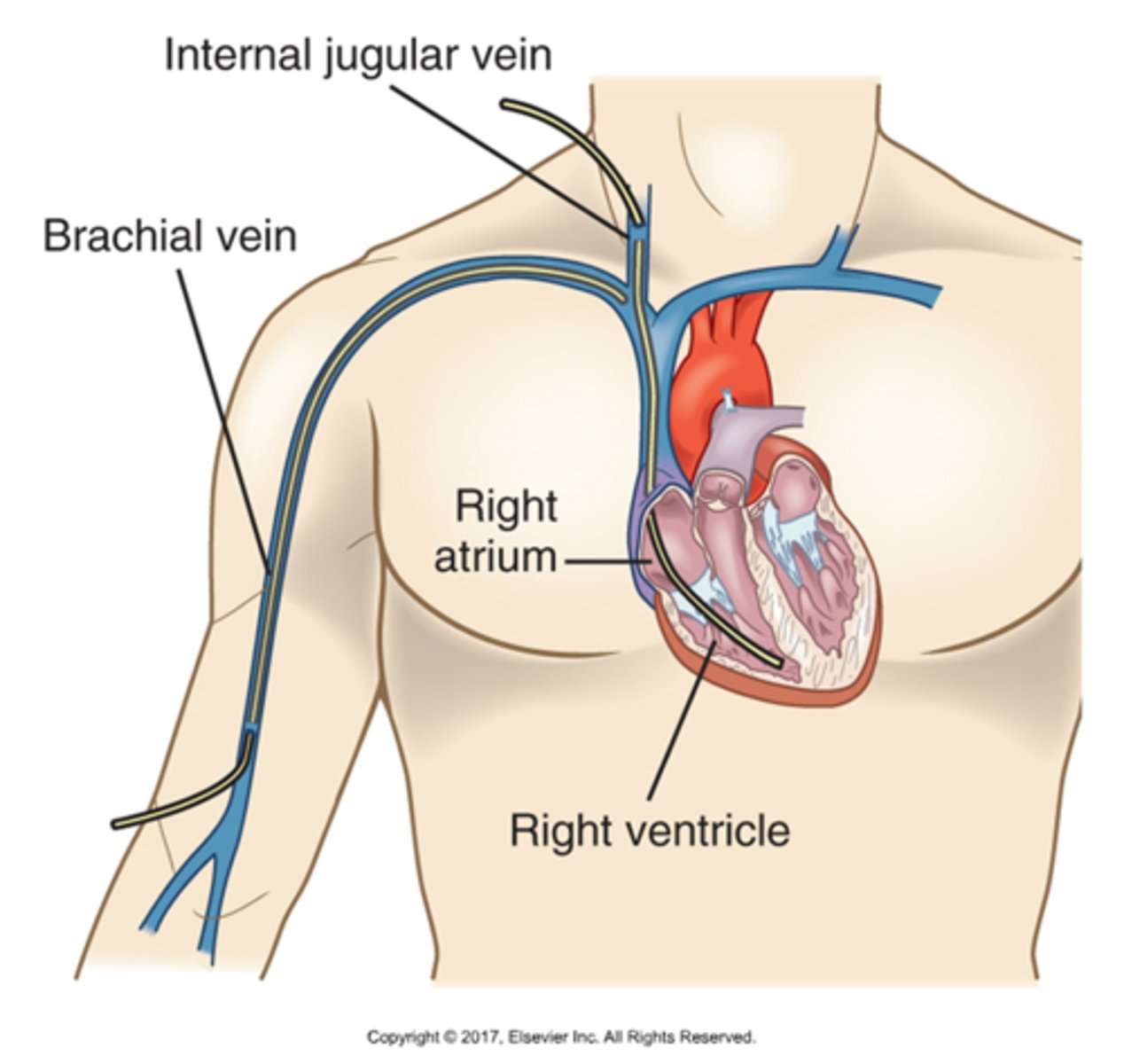
2. Transvenous pacing (catheter in heart)
3. Permanent pacer (implant)
Temporary pacemakers
Used when dysrhythmia is likely to last only a few days
Most common types: Transvenous & Transcutaneous
Pulse generator at bedside
Permanent Pacemaker
Used when dysrhythmia is thought to be permanent
Implanted surgically
Can be used to pace atrium, vernticle, or both
Components: Battery (last 5-10 yrs), pacing catheter
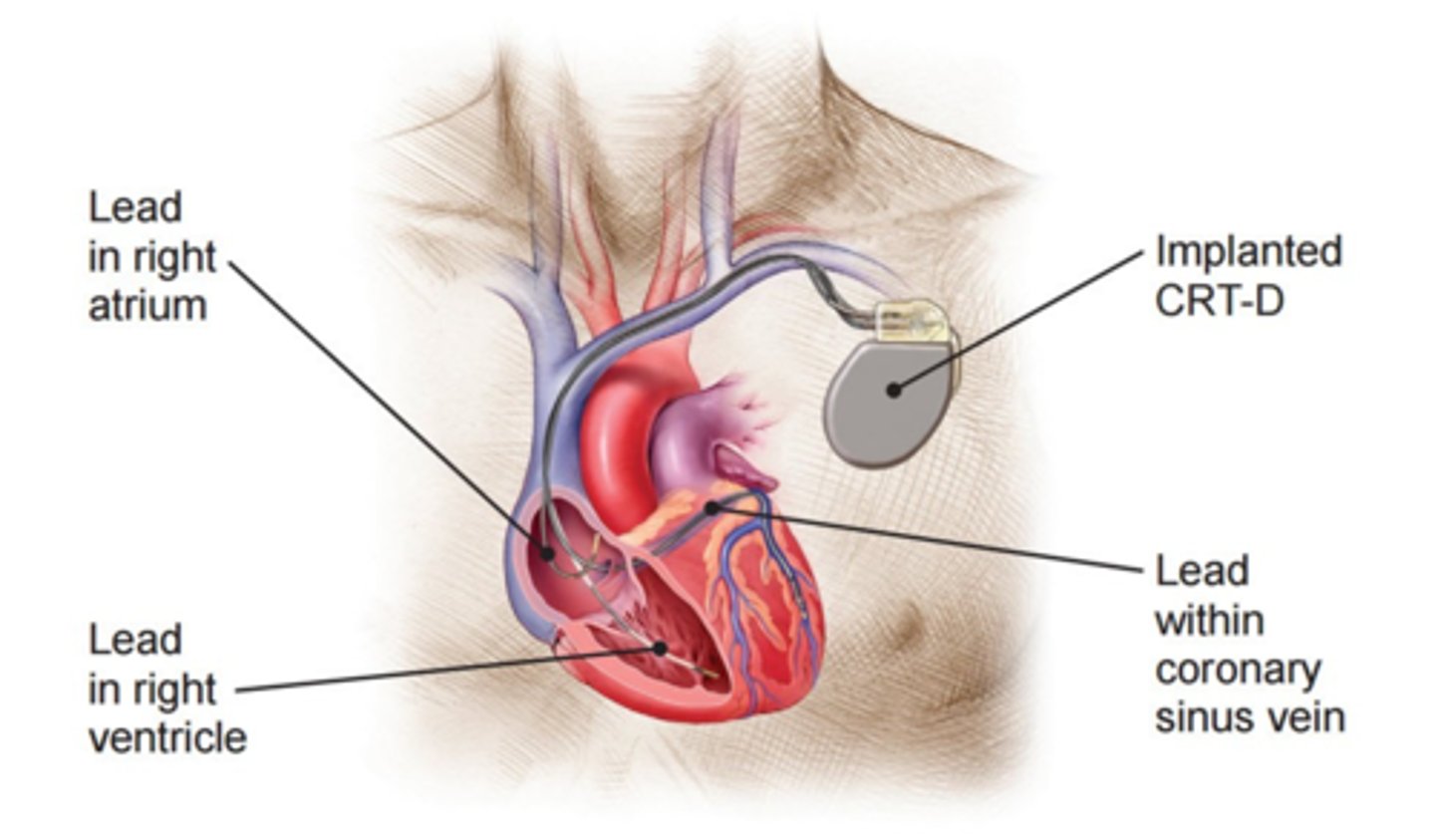
Cardiac resynchronization therapy (CRT)
Pacing technique that paces both ventricles to promote ventricular function in HF pts
Pacing: Atrial, Ventricular, Dual Chamber
Dual chamber: both atrial and ventricular are paced
Implantable cardioverter defibrillator (ICD)
Treatment for life-threatening ventricular arrhythmias
Lead system placed via subclavian vein to endocardium
Pulse generator is implanted over pectoral muscle
Batteries must be changed ab every 5-10 years