7/8- direct and indirect resto
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
What are direct restorations?
Can be fabricated and completed inside the mouth- don’t need lab
Can do in single appointment with no provisional or temp resto
What are indirect restorations?
Cannot be fabricated inside the mouth- crowns, bridges, implants, inlays/onlays, veneers
Need 2 appointments
What are 7 disadvantages of direct composite restorations?
Fatigue
Wear
Polymerization shrinkage (indirect composites avoid secondary problems like infiltration, gaps, fracture of enamel, cuspal deflexion)
Must be biocompatible- pulp and periodontal tissues
Degree of conversion is about 70% (vs indirect is 95%)
Colour changes over time associated with external dyes (can polish indirect better)
Surface roughness of direct composite leads to retention of plaque and abrasion of the antagonist teeth
What are 6 advantages of using indirect restorations?
Better polymerisation than direct composites- 95% degree of conversion
Better physical and aesthetic properties.
Restoration-tooth discrepancy supplied by cement (better dual cure cement)
Better contact point (avoid food packaging problems)
If fracture can be restored in the clinic with composite
In patients with bruxism- ceramic wears less than the resin as it is hard
What are 3 disadvantages of using indirect restorations?
Complex prep
Usually 2 visits required (even if 1 visit- longer)
Higher cost to the patient
5 Indications of using indirect restorations?
Restorations in the posterior sector of large cavities-
MOD of premolars and molars (inlays)
Onlays in premolars and molars
Simultaneous restorations (multiple teeth)
Endodontic teeth reconstruction (recommended to do cuspal coverage here)
Posterior aesthetics
4 Contraindications of using indirect restorations?
Prep that exceed the enamel-cement limit→use glass ionomers
Poor oral hygiene
Severe parafunction (bruxism) NEVER
Short and non-retentive crowns
What are some common radiopaque adhesive systems and some characteristics?
Clearfil universal bond quick- contains fillers, fast application
Optibond universal- increases bond strength and layer thickness
G-Premio bond- better visibility under x ray
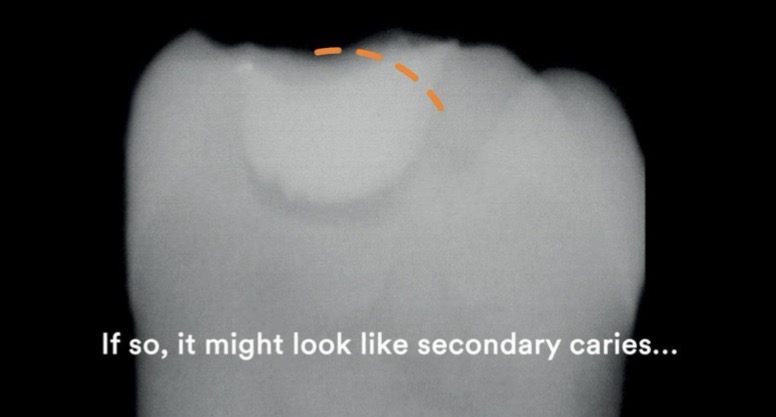
Radiolucent adhesive- invisible on x ray- contains nano fillers (silica), could be mistaken for secondary caries
What are the 5 steps of Stratification technique for posterior composites?
Isolate + prep cavity
Etch + adhesive
Build proximal wall first- place thin layer against the matrix to create enamel wall- converts to class 1 (layering easier)
Layering- use dentin shade composite in 2mm increments
b. Cusp by cusp build up- better anatomy, less finishing needed, better stress distribution
c. Final enamel layer- apply more translucent shade, keep thin- natural and wear resistance
Occlusal anatomy and finishing- carve primary grooves, triangular ridges, fossae before final cure, after curing- check occlusion
What is the oblique layering technique?
Each increment only touches 1-2 walls, reduces polymerisation stress
Critical in posteriors to prevent marginal leakage and post op sensitivity
What are 5 common mistakes in posterior stratification?
Bulk filling- shrinkage and cuspal deflection
Skipping proximal wall step- poor contact
Flat occlusal surface- bad function
Thick increments- incomplete curing
Ignoring occlusion- post op pain
Why is flowable composite not suitable as a final layer?(4)
Material Properties: Flowable composites have:
. Lower filler content (not strong)
. Lower viscosity (they flow easily)
. Lower mechanical strength
. Higher wear rate
What happens if you use flowable composites as a final layer in posterior teeth (high load)? (4)
Rapid occlusal wear
Loss of anatomy (cusps flatten)
Increased risk of fracture
Poor occlusal stability
What happens if you use flowable composites as a final layer in anterior teeth? (4)
Poor polish retention
Surface becomes rough over time
Staining and discoloration
Inferior translucency control vs enamel composites
Why should you not over etch dentin?(3)
Collagen network collapses
Poor resin infiltration
Leads to weak bond, post op sensitivity
Why are composite resin inlays and onlays a good choice for teeth with wide proximal occlusal cavities?(6)
Aesthetics and high quality function compared to porcelain or direct
Structural- returns nearly all original strength
Abrasion- wear at same rate as natural tooth- but also new ceramic material like E max (ivoclar vivadent) good option too
Conserve tooth structure
Supragingival margins
Chair side repairs
5 Advantages of porcelain inlays?
Good esthetics– color harmonious with that of tooth structure
Low thermal conductivity
High tolerance of the soft tissues to its presence
Chemically inert and relatively insoluble in oral fluids
A coefficient of thermal expansion close to that of natural tooth
6 Disadvantages of porcelain inlays
Expensive and timely compared to direct resto
Technique sensitive
Some newer ceramic restorations need special and expensive lab equipment
Brittle, if inadequate thickness- can fracture during try-in or post cementation, esp if high forces
High hardness- can cause abrasion of the opposing teeth or restorations
Lack of perfect adaptation to cavity walls exposes the cement line
Why is the use of non eugenol cements like TempBond recommended for Cementation?
Eugenol has plasticising effect on resin cements and bonding agent
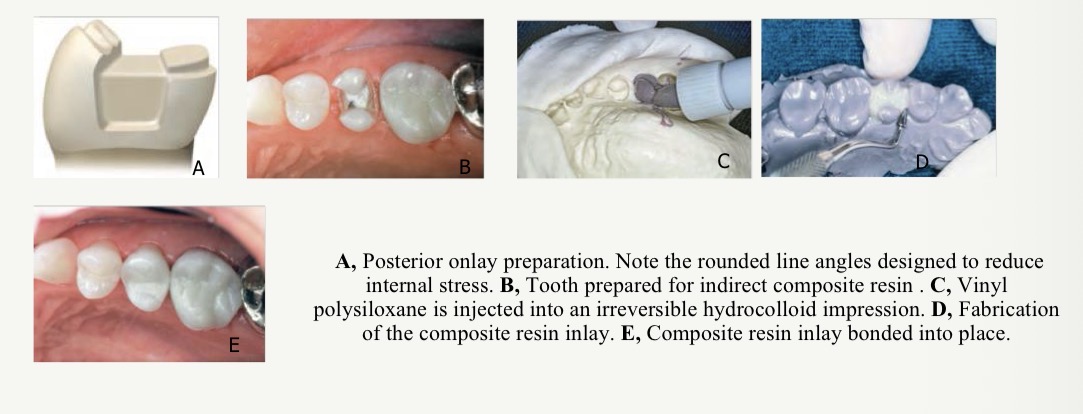
What is a flexible cast fabrication?
A completely indirect technique, performed in 1 appointment, doesn’t require a provisional restoration can be accomplished using a flexible cast technique
What are the 6 steps in the clinical technique to make a flexible cast?
Prep same as direct/indirect technique
Make an irreversible hydrocolloid impression to see margins of prep
Inject a firm setting vinyl polysiloxane impression material into the alginate to form a flexible cast
Fabricate inlay using light cured hybrid composite resin
Heat treat resto and place