Antibiotic use for ocular conditions
1/149
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
150 Terms
internal hordeolum
What condition does this patient most likely have?
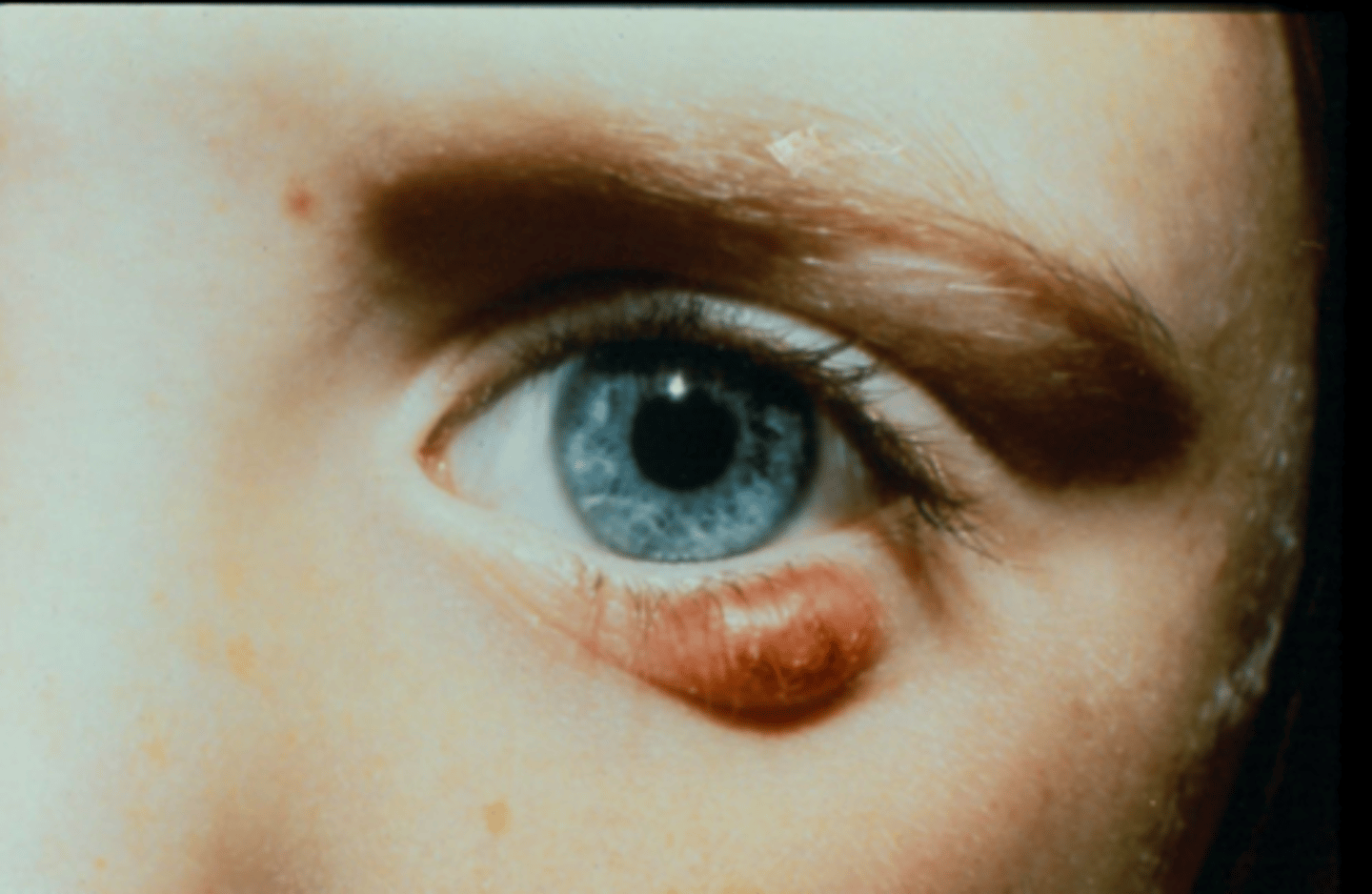
active infection of meibomian gland
What is an internal hordeolum?
localized redness and swelling, soft and warm to touch, quiet eye and lid margin
What are presentations of internal hordeolum?
external hordeolum
What condition does this patient most likely have?

active infection of gland of zeiss/moll
What is an external hordeolum?
protrusion (puss point) at the lid margin
What presentation differentiates an external hordeolum from an internal?
preseptal cellulitis
What condition shown here must we consider with a hordeolum?

diffuse redness that extends from canthus to canthus (entire lid)
What presentation differentiates a preseptal cellulitis from an internal hordeolum?
chalazion
What condition shown here must we consider with a hordeolum?

localized bumb of coagulated lipid within meibomian gland (NOT an active infection)
What is a chalazion?
hard nodule, NOT warm to touch, NOT red
What presentation differentiates a chalazion from an internal hordeoolum?
No predilection for age or gender
What is the epidemiology for an internal hordeolum?
acute and can be recurrent if associated with blepharitis
What is the temporal pattern for an internal hordeolum?
unilateral, swollen eyelid with localized redness and edema within a MG that is soft and warm to touch
What is the syndrome statement for an internal hordeolum?
systemically
Do we treat a worsening internal hordeolum topically and/or systemically?
Augmentin 500 mg tablets
What penicillin is the DOC for an internal hordeolum?
BID for 10 days
How often do we Rx Augmentin 500 mg for a patient > 88 lbs (40 kg)?
TID for 10 days
How often do we Rx Augmentin 500 mg for a standard adult patient > 115 lbs?
ability to swallow a pill? weight?
What should we ask our pediatric patients when Rx'ing Augmentin?
beta lactamase inhibitor
What is the MOA of clavulanic acid to help amoxicillin with staph protection?
cefprozil or Keflex (cephalexin) 500 mg BID for 10 days
What cephalosporin are DOC for an internal hordeolum in adults?
cefprozil 250 mg BID for 10 days
What cephalosporin is DOC for an internal hordeolum in kids?
Bactrim DS 800/160 mg BID for 10 days
What is the backup medication for infectious lid disease in adult patients with PCN or Ceph allergy?
azithromycin 500 mg QD for 3 days
What is the backup medication for infectious lid disease in pediatric patients with PCN or Ceph allergy?
stays at MIC due to slow metabolism and long half-life
Why can we Rx azithromycin for 3 days only?
bad GI effects (can be worse than eye problem)
Why do we not use Bactrim DS for pediatric patients?
azithromycin has a lot of staph resistance
Why do we NOT use azithromycin instead of Bactrim DS for adult patients?
diarrhea (warn patient and advise to stay hydrated)
What is the main GI effect from Bactrim DS?
MRSA of skin around eye
What is Bactrim DS DOC for?
MRSA of ocular surface
What is Polytrim DOC for?
do not try to express!!
warm compress to increase blood flow and more abx to target site (some palliative care)
What are other management plans for an internal hordeolum patient?
No
Is a follow up required for an internal hordeolum or bacterial conjunctivitis?
if they get worse or not healed by end of abx therapy
When can you tell a patient with an internal hordeolum or bacterial conjunctivitis to return to clinic?
may take a couple days to improve, but if completely resolved within 10 days still ALWAYS finish course of treatment (scare them by saying secondary infection will be worse)
What do we need to educate patients on that are taking an oral abx?
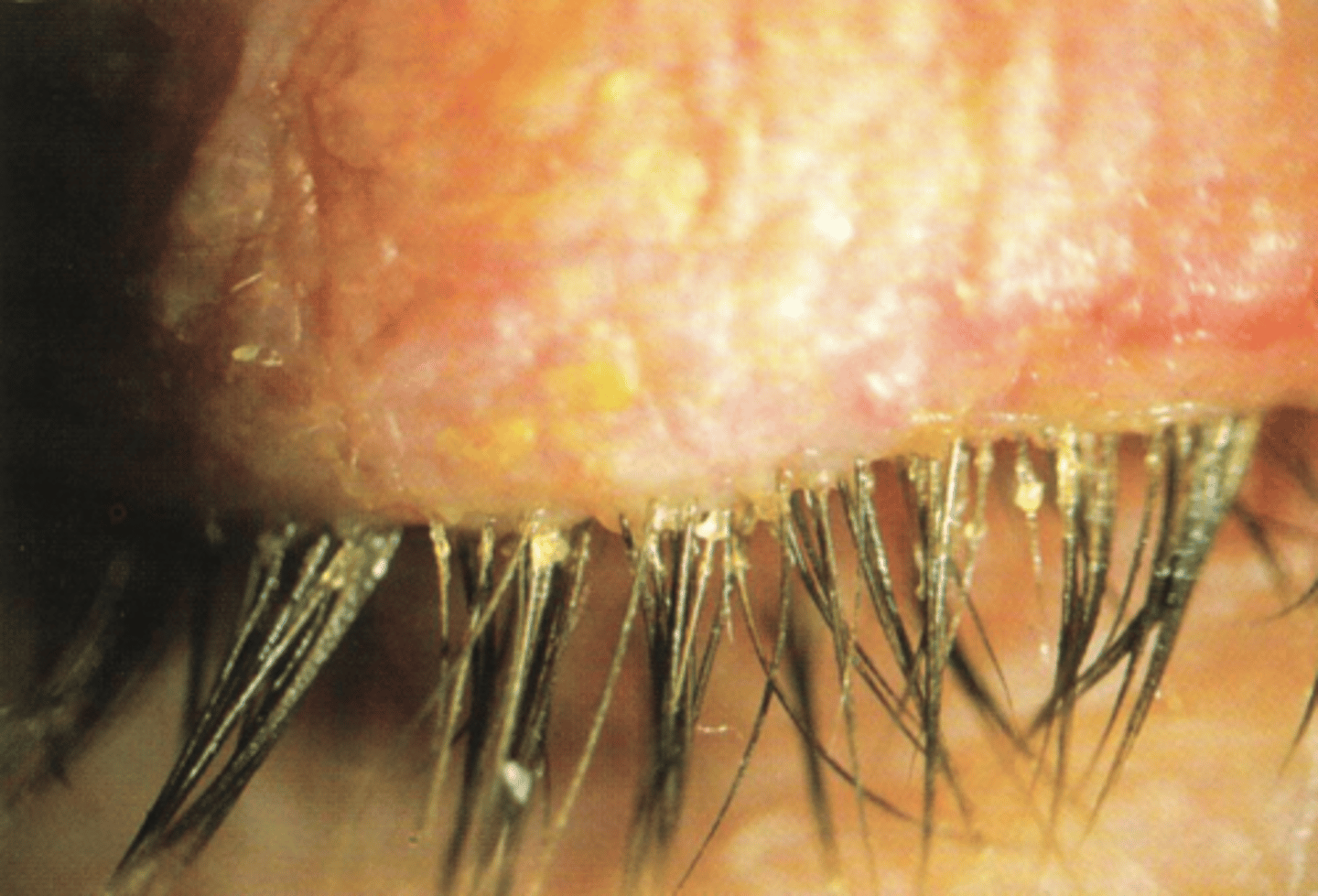
blepharitis
What ocular condition is shown here?
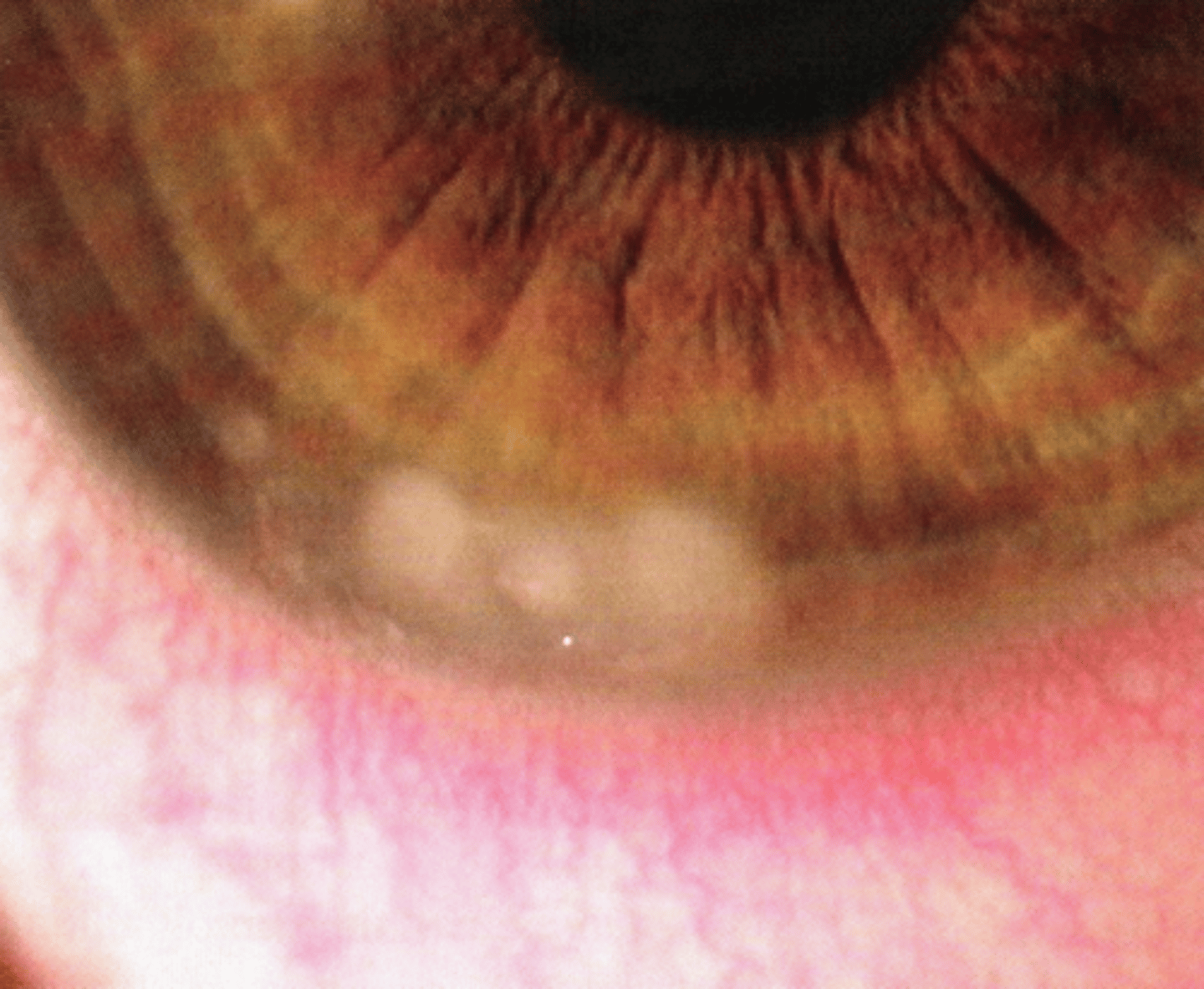
keratitis and uveitis
What ocular conditions are we concerned when a patient complains of photophobia (light sensitivity)?
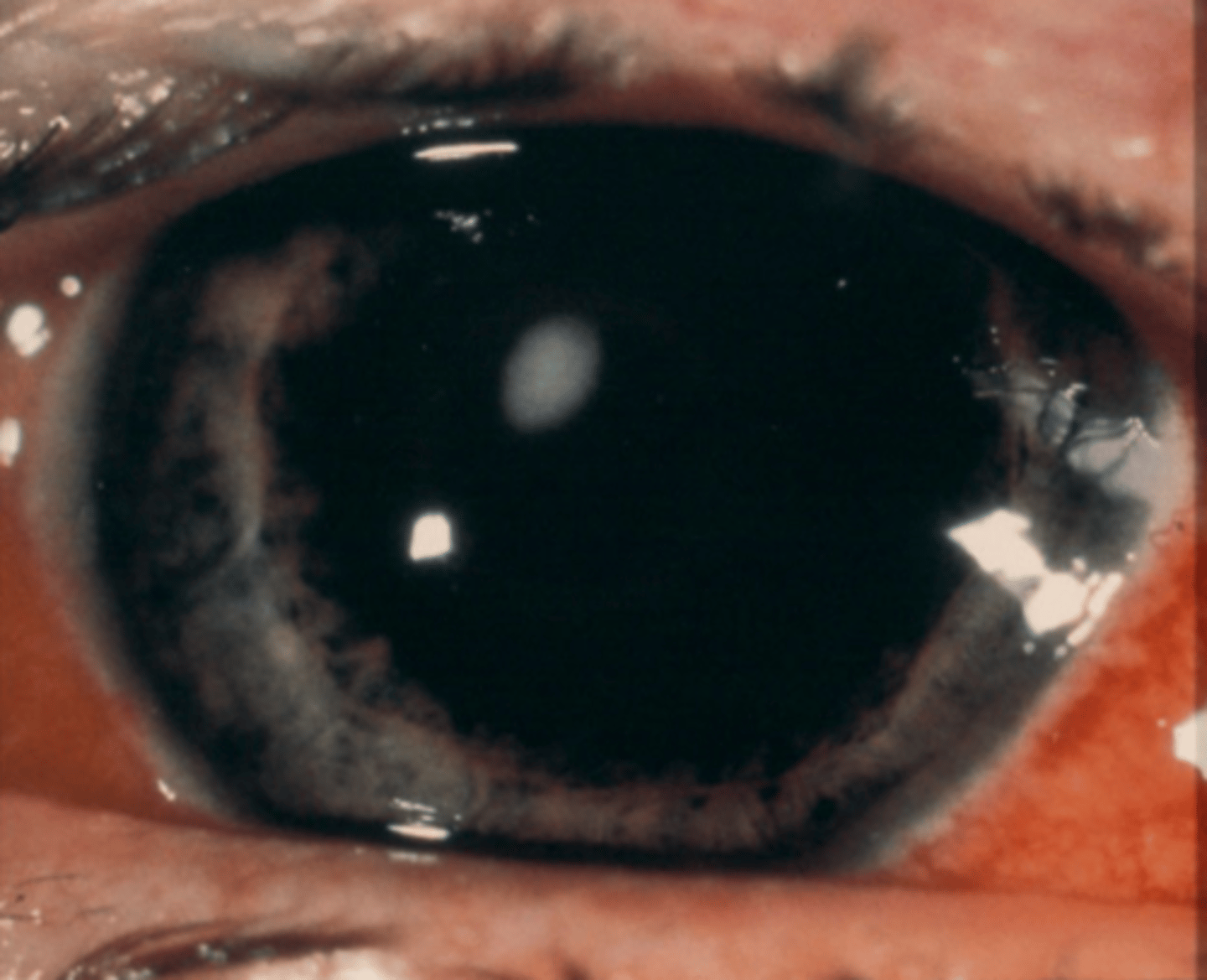
multiple, peripheral corneal infiltrates with localized paralimbal injection
How would you describe what we see on slit lamp here?
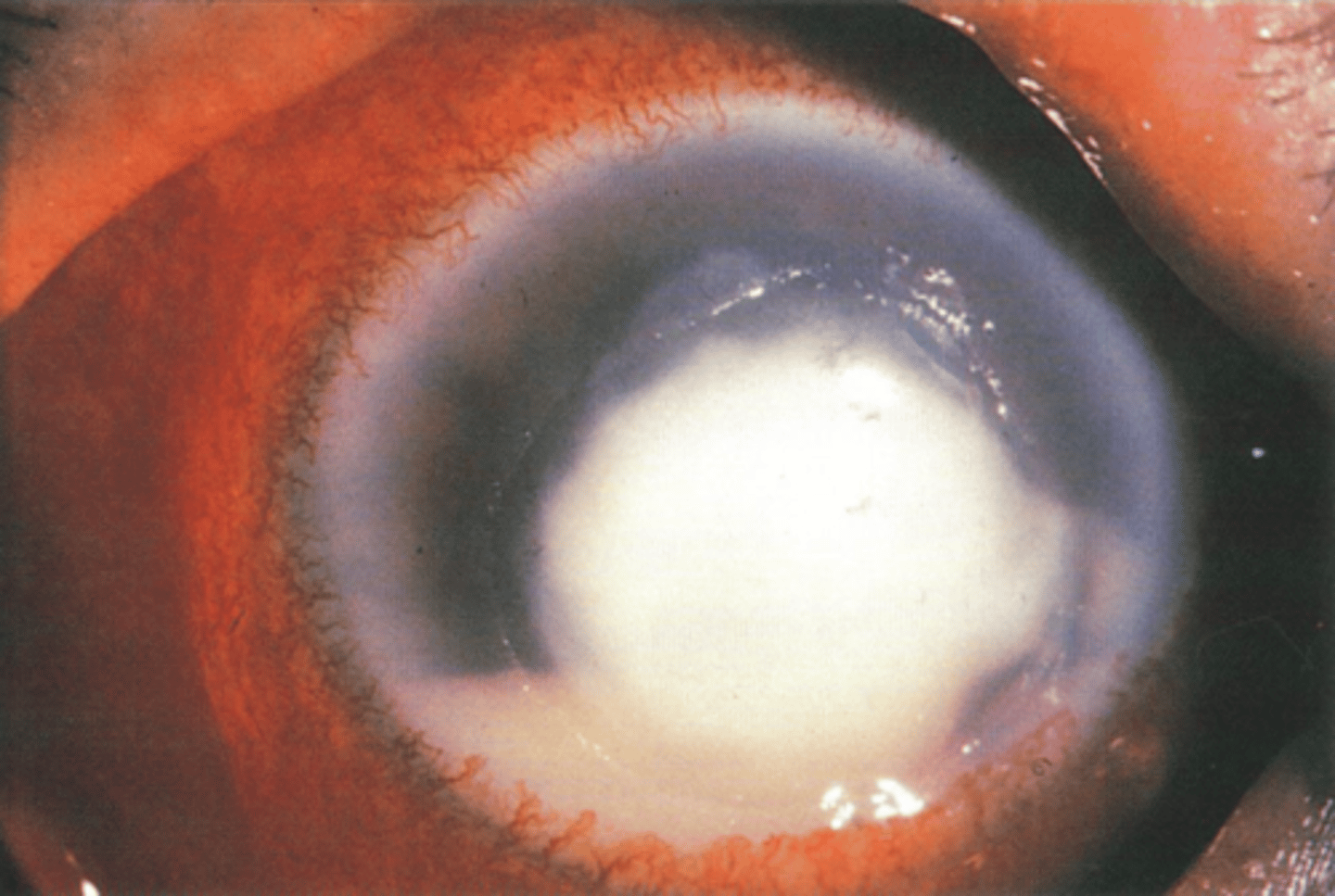
ulcer
What does this staining pattern over the corneal infiltrates indicate?
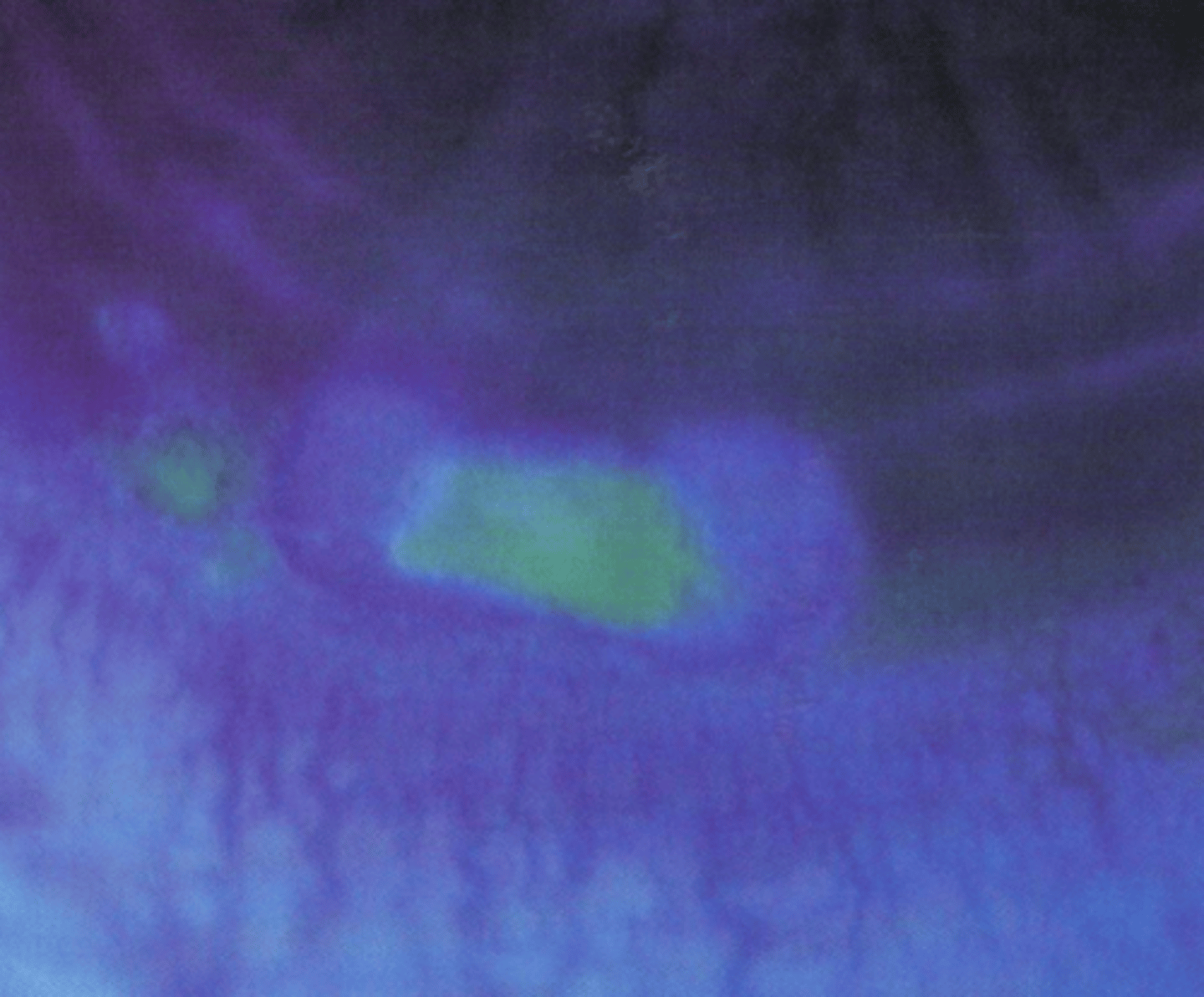
infiltrates (erode the epithelium to create an ulcer)
Do infiltrates or ulcers come first?
marginal keratitis
What is most likely the diagnosis of the patient shown here? (not a CL wearer)
staph hypersensitivity reaction (inflammatory) due to poor lid hygiene
What is the cause of marginal keratitis?
exotoxins (from staph) deposit on cornea where the lid margin intersects
What causes corneal infiltrates (collection of WBCs) in marginal keratitis?
single lesion
What # of corneal lesions are more likely to be infectious?
central 6 mm
What location of a corneal lesion are more likely to be infectious?
entire lesion stains
What degree/size of staining of a corneal lesion is more likely to be infectious?
severe
What pain level is more likely to be infectious?
diffuse (360) injection
What pattern of redness is more likely to be infectious?
cells (look for hypopyon)
What AC reaction is more likely to be infectious?
culture
What is the only way to get a definitive diagnosis if a corneal lesion is infectious or sterile (inflammatory) in nature?
sensitivity
What other test is usually done with the culture to determine what antibiotic the bacteria is susceptible to?
1+ or greater AC cells
2 mm dense infiltrate
edge of infiltrate within 3 mm of central cornea (within pupillary zone)
What is the "1, 2, 3 rule" when predicting the likelihood of vision loss after resolution of infection? *Need to culture if ANY of the following exist
yes
Should we culture this lesion shown here?
yes
Should we culture this lesion shown here?
no
Should we culture this lesion shown here? *staining less than infiltrate size
adults
What is the epidemiology of marginal keratitis?
acute and recurrent with ongoing blepharitis
What is the temporal pattern of marginal keratitis?
typically unilateral red eye with mild to moderate symptoms of pain, tearing, irritation, and photophobia, exam reveals multiple corneal infiltrates or ulcers with minimal staining, localized conjuntival injection near lesion on limbus, no or minimal AC reaction, typically seen with staph blepharitis
What is the syndrome statement for marginal keratitis?
yes, topical (combo steroid/abx)
Does marginal keratitis warrant pharmaceutical treatment? If so, do we need to treat topically and/or systemically?
anti-inflammatory
What is the steroid component used for in marginal keratitis?
remove stimulus that caused bacterial colonization
What is the abx component used for in marginal keratitis?
Zylet ophthalmic suspension (0.3% tobramycin, 0.5% loteprednol)
What is our brand name DOC for marginal keratitis?
0.3% tobramycin/0.1% dexamethasone ophthalmic suspension
What generic is our DOC for marginal keratitis?
1 gtt q2hr for 2 days, then QID for 5 days
What is the dosing pattern for Zylet and generic Tobradex?
SHAKE WELL PRIOR TO USE
What do we have to remember to include on the Rx for Zylet and generic Tobradex?
daily lid hygiene
What are our other management plans for a patient with marginal keratitis?
OcuSoft Plus Lid Scrubs
What is a good soap-based lid hygiene product to recommend?
hypochlorous acid
What do medicinal-based lid hygiene products contain?
preservative free
What is a benefit of hypochlorous acid?
yes, due to corneal involvement
Do we need to follow up with a marginal keratitis patient?
emphasize compliance to drops and lid hygiene and check IOP due to steroid component
What are other benefits of following up with our marginal keratitis patient?
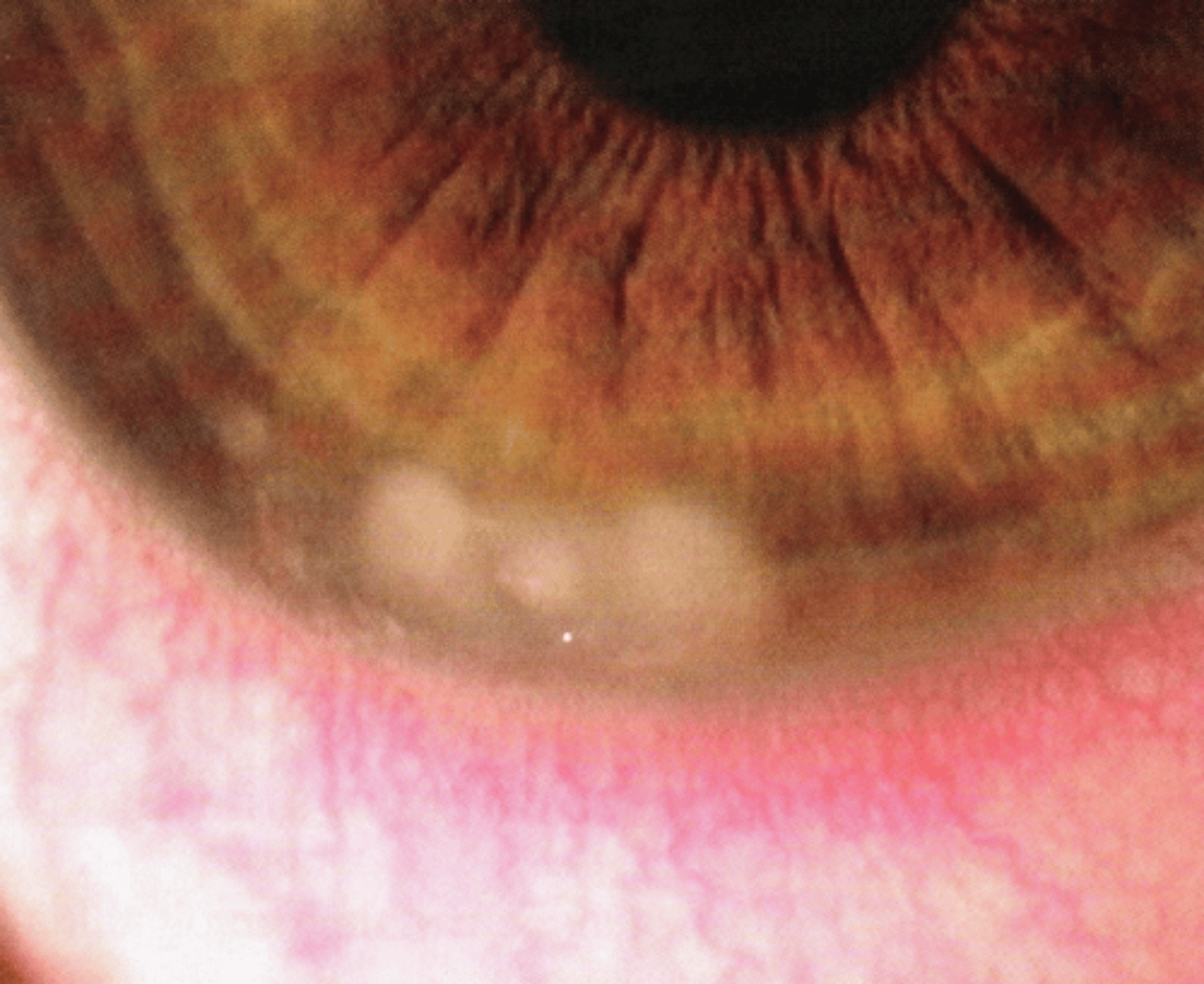
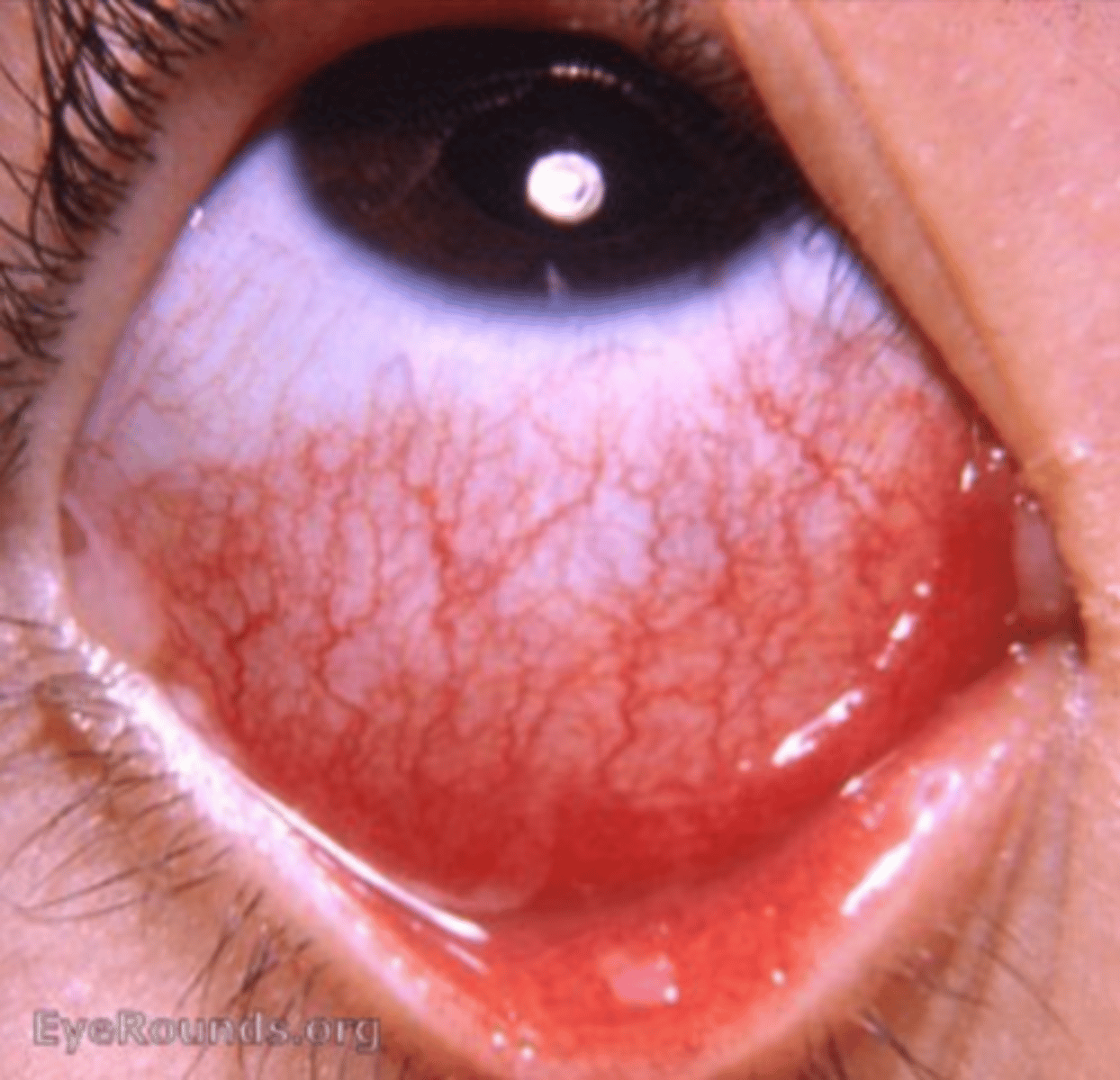
bacterial conjunctivitis
What ocular condition is most likely diagnosis shown here?

mucopurulent discharge
What is pathognomonic for bacterial conjunctivitis?
eyes stuck shut upon waking
What is the most common complaint from mucopurulent discharge?
Neutrophils (PMNs)
What white blood cells are found in mucopurulent discharge?
inferior conjunctiva
Where does redness most commonly occur in bacterial conjunctivitis?
papillae
What is a common finding on the inferior palpebral conj in bacterial conjunctivitis?
toxicity of PMNs
What may cause inferior corneal staining in bacterial conjunctivitis?
adult inclusion conjunctivitis
What ocular condition can have ongoing mucopurulent discharge and is secondary to chlamydia?
follicles on superior palpebral conj
What is pathognomonic for adult inclusion conjunctivitis?
EKC
What viral ocular condition can have a "mucopurlent discharge" with other symptoms such as profuse watering, chemosis, and lid edema?

pseudomembrane
What mimics mucopurulent discharge in EKC?
hyperacute conjunctivitis (onset of 6 hours)
What do we always need to rule out in a bacterial conjunctivitis, as shown here?
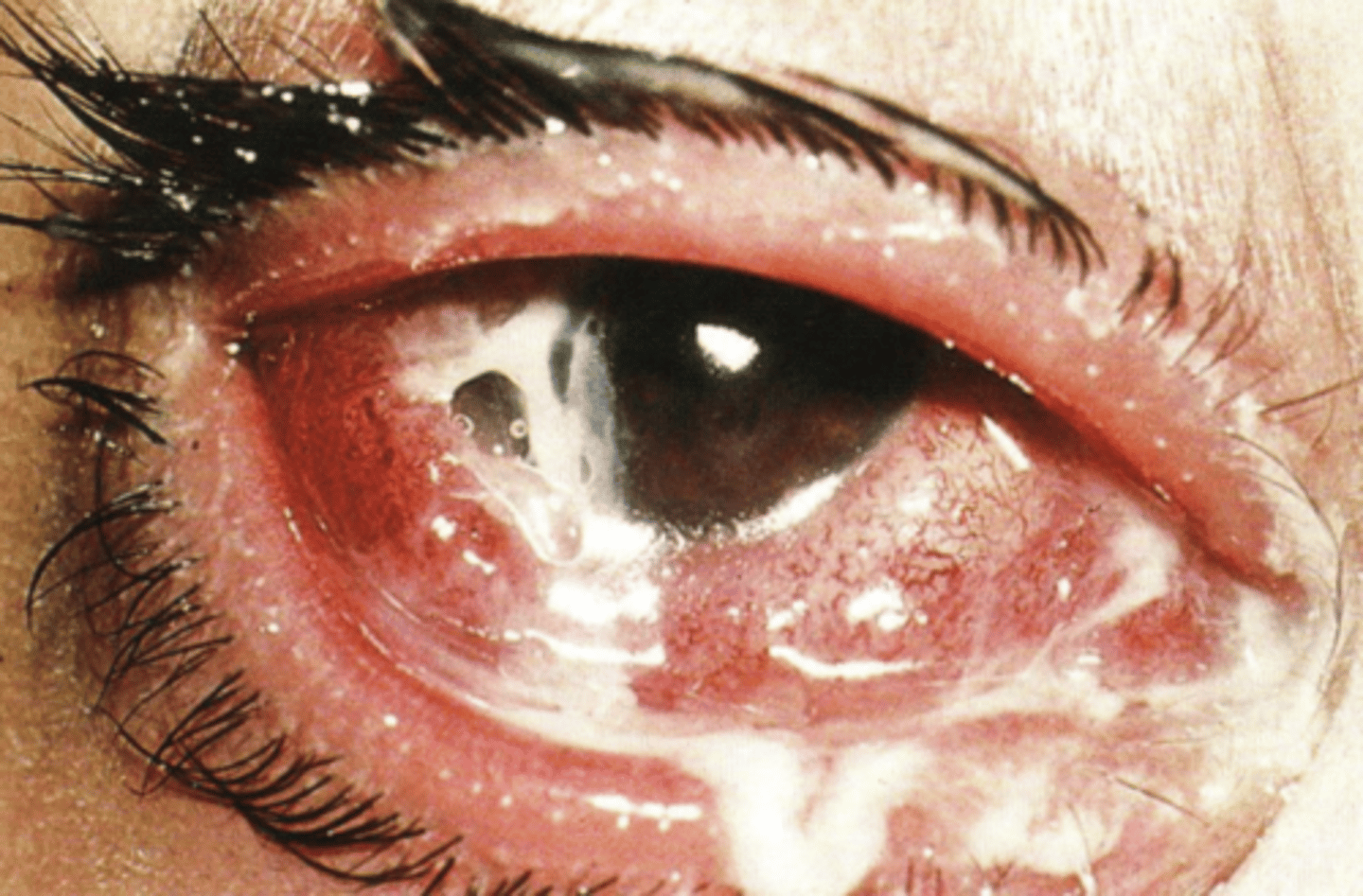
neisseria gonorrhoeae
What is the #1 cause of hyperacute conjunctivitis?
can penetrate an intact epithelium and perforate the globe
Why is hyperacute conjunctivitis a medical emergency?
true purulent (snow white)
What type of discharge does hyperacute conjunctivitis have?
1g IM Ceftriaxone (3rd gen ceph) and 1g azithromycin
What is the systemic treatment for hyperacute conjunctivitis?
Ciloxan (ciprofloxacin) q1-2 hrs and irrigation q1hr to clean out discharge
What is the topical treatment for hyperacute conjunctivitis?
No predilection for gender or age
What is the epidemiology for bacterial conjunctivitis?
acute
What is the temporal pattern for bacterial conjunctivitis?
burning
What is the most common symptom of bacterial conjunctivitis?
complaints of burning, FB sensation, lids stuck shut in the morning due to mucopurulent discharge, signs of meaty redness that is worse in inferior bulbar conj and papillae in inferior palpebral conj
What is the syndrome statement for bacterial conjunctivitis?
gradient of redness
What do we call the transition of white eye to red eye in bacterial conjunctivitis?
yes, topical antibiotic only
Does bacterial conjunctivitis warrant pharmaceutical treatment? If so, do we need to treat topically and/or systemically?
assist immune system to lower bacterial count and get better faster
Why would we treat a bacterial conjunctivitis patient and how do antibiotics do this?
3-5 days
When does our peak immune response occur after infection?
after 24 hours on drops
When are bacterial conjunctivitis patients no longer contagious if being treated?
after discharge resolves
When are bacterial conjunctivitis patients no longer contagious if not being treated?
tobramycin 0.3% ophthalmic solution
What is our topical DOC for bacterial conjunctivitis due to dosing schedule?
1 gtt QID for 7 days
What is the SIG for tobramycin in treatment of bacterial conjunctivitis?
tobramycin and gentamycin
What topical antibiotics are available as ung for bacterial conjunctivitis in kids?