Visual Field Assessment
1/52
Earn XP
Description and Tags
The essential elements and terms of visual field assessments
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
53 Terms
The Visual Field
Sensitivity of different retina areas to light stimuli > peripheral vision
All the space that one eye can see at any given instant.
Tate and Lynn 1977
‘Space’ to highlight that eyes look at three-dimensional volume rather than two dimensional surfaces
Three -dimensional space is often translated into two dimensions
photographs
The sensitivity of the retina varies
Macula most sensitive
Periphery less sensitive
ONH – blind spot
The sensitivity of the retina varies with light level
Light conditions
Dark conditions
Low light conditions
The measurement of this sensitivity is also dependent on the stimulus used while measuring it
Normal extent of the visual field (monocularly)
More temporally than nasally
More inferiorly than superiorly
Facial contours influence extent
Limited by the bridge of the nose and the extent of the brow
The visual field is tested ________ and is more temporally and inferior.
Monocularly
The Visual Field
Both eyes open
Horizontally field has an extent of 200º
Overlap of 120°
Binocular Field
Where both eyes can see the stimulus
60 degrees either side of the vertical midline
60 degrees up
75 degrees down
Inferiorly the binocular field is affect by the nose
The overlap field is _______.
120 degrees
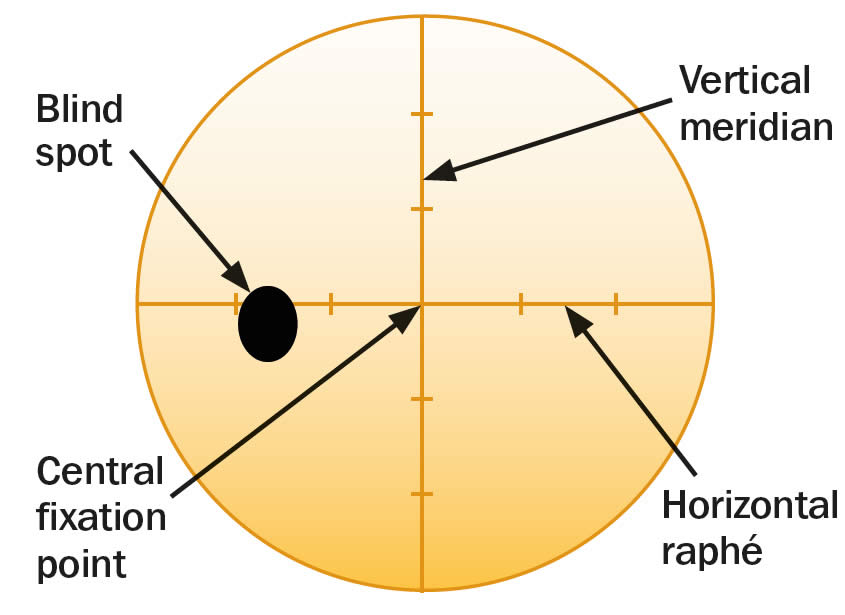
Hill of Vision
Most sensitive
Fovea
Least sensitive
Blind spot (black bar)
This slice is along the horizontal
High point of the hill is the ______ and it is located closer to the nasal side.
Fovea
Blind Spot
Vertical oval 8.5 x 5.5 degrees
Located 15.5 degrees temporal to fixation and 1.5 degrees below the horizontal midline
Absolute
Relative
The blind spot is an area in your field of vision where you cannot_____.
See
Why Measure VF?
Evaluation of the peripheral retinal function
Evaluation of the neural pathway function
Evaluation of function of higher centres of the brain which process visual information
Functional problems anywhere on the visual pathway can have a pattern which is indefinable and specific
As part of a comprehensive eye examination
Retina lesions
Glaucoma
Toxic amblyopia
Optic nerve lesions (e.g., optic neuritis)
Diseases affecting visual pathway
Stroke, tumours, inflammation
Conditions exhibit specific VF patterns
Evaluation of normal vision
Evaluation of abnormal vision
Monitoring normal or abnormal vision for change
Improvement
Deterioration
Finding the island of vision for each eye
If there is damage to the right cortex it will be apparent in the left visual field of both eyes
If there is damage to the left cortex it will be apparent in the right visual field of both eyes
Measuring the visual field is important is it evaluates peripheral retinal function, ________ function, and brain centres for visual processing.
Neural Pathway
Factors Affecting VF Results
Facial contour
Thick spectacle frames
Myopia, Hyperopia
Pupil size
Media opacity
Px fatigue
Malingering
These are all things that could affect visual field results. True or False?
True
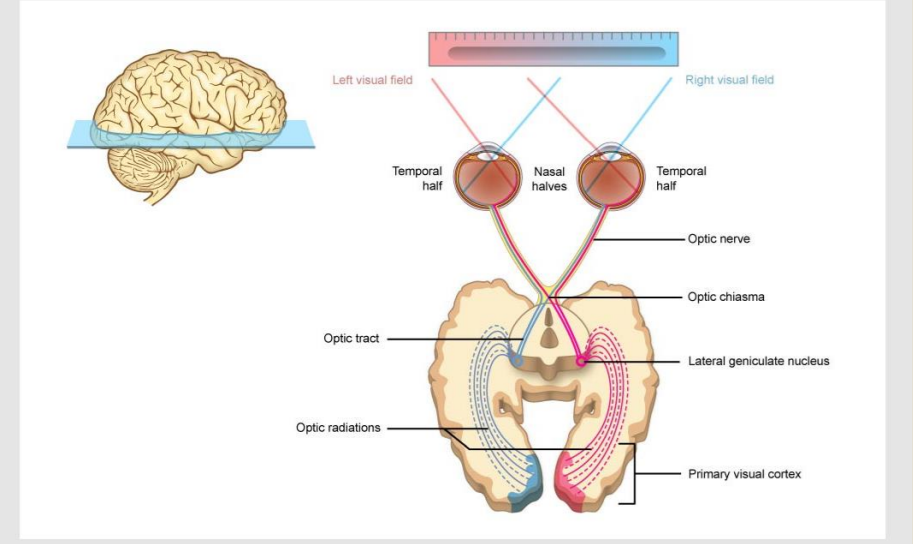
The Visual Pathway
Information collected by the retina exits the eye through the optic nerve
The optic nerve leads to the optic chiasm where the optic nerves meet
Information from the left visual field passes to the right lateral geniculate nucleus
Information from the right visual field passes to the left lateral geniculate nucleus (LGN)
From the LGN the information goes via the optic radiations to the primary visual cortex
The optic chiasm sorts nerves according to the information they will carry
The left visual cortex receives information from both eyes but one visual field
The right visual cortex receives information from both eyes but one visual field
This sorting of nerves helps us locate where visual field defects originate from
Each visual cortex receives information from both eye but only ______ visual field.
One
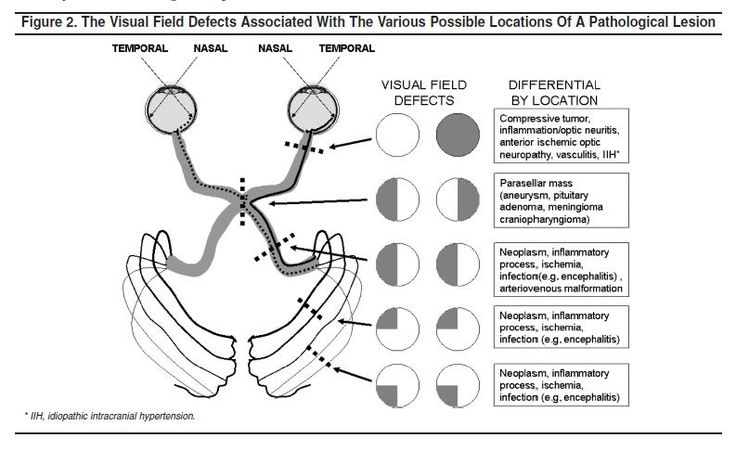
Origin of defects
Anterior to the chiasm field defects respect the horizontal midline
Posterior to the chiasm field defects respect the vertical midline
The exceptions
Macula sparing - the preservation of central vision, specifically the macula, despite damage to the visual cortex
In the retina
In the cortex
The _______, ________ & _______ are exceptions to being origins of VF defects.
Macula Sparing; Retina; Cortex

Central Scotoma - a blind spot or area of reduced vision that appears in the central part of the visual field
Monocular Vision Loss - the inability to see with one eye
Bitemporal Hemianopia - a condition where vision is impaired in the outer (temporal) halves of both visual fields.
Contralateral Homonymous Hemianopia - a visual field loss where the same half of the visual field is affected in both eyes
Contralateral Superior Quadrantopia - a visual field defect where a person loses vision in the upper quadrant of their field of view (on the same side)
Contralateral Inferior Quadrantopia - a visual field defect where a person loses vision in the lower quadrant of their field of view (on the same side)
Contralateral Homonymous Hemianopia with Macular Sparing - a visual field defect where vision is lost in one half of the visual field on both eyes (same side), but the central vision (macula) is preserved.
Contralateral VF defects are normally on the same side. True or False?
True
Strategy Types:
Kinetic perimetry: Stimuli of a set size and intensity moves through the field.
The size of the stimuli can be varied
The intensity of the stimuli can be varied
The presentation time can vary
Speed of movement of the stimuli through the field
Goldmann perimetry (1945) is a manual, kinetic visual field test that assesses an individual's peripheral vision by having them indicate when a moving light stimulus enters their field of view
Static perimetry: Each stimulus is at a fixed point on the background
The size of the stimuli can vary (generally doesn’t)
The intensity of the stimuli can vary
The presentation time can vary
Flicker-perimetry (less common nowadays)
‘Frequency doubling technology (FDT) perimetry is based on a flicker illusion created by counterphase flickering of a low spatial frequency sinusoidal grating at a high temporal frequency. This phenomenon essentially creates an image that appears double its actual spatial frequency.’
Goldmann perimetry is a ______ VF tests.
Kinetic
Photometric Background
Units of illumination
How much light is falling on a surface
Not perceived by the eye
Units of luminance
How bright something appears (perceived by the eye)
How a surface emits or reflects light
Units for luminance cd/m2 or apostolibs (1cd/m2=3.14 asb)
Photopic conditions
Mesopic conditions (dusk) – reduces cone activity and flattens peak
Scotopic conditions (night)-external isopter widens due to increased rod response and a central depression due to lack of rods
Modern perimeter use a background luminance in the low photopic range
Visual deficits are not all apparent at the same light levels
Retinal sensitivity fluctuates even when stabilised
Fluctuation more with a shallow profile
Time to adapt to dark condition (scotopic) takes longer that for photopic conditions
Ambient light levels in clinical areas are difficult to control
Brighter background luminance is insensitive to these fluctuations
Higher background luminance (photopic) have a shorter time to adapt to
Most tests have chosen 10cd/m2=31.5abs
______ is how bright something appears to the eye
Luminance
How the Visual Field is Measured
Stimulus intensity against a background intensity
The stimulus can be varied
Position in the field
Size
Intensity (brightness)
Presentation time
Colour
The stimulus can be varied (SCIPP). True or False?
True
Insensity vs Sensitivity
When measuring fields we are interested in how bright the stimulus and background appear to the eye
For a stimulus to be visible, the luminance of the stimulus has to be greater than the luminance of the background
The intensity of the stimulus that is detectable from a background is described as sensitivity
The stimulus has intensity
The eye has sensitivity
The stimulus has _______ and the eye has ______.
Intensity; Sensitivity
Position of Stimuli
Described by eccentricity from the fixation point
Where the patient looks when performing the test
Fixation point relates to the fovea
The eccentricity from the fixation point is the distance from the fixtion point. True or False?
True
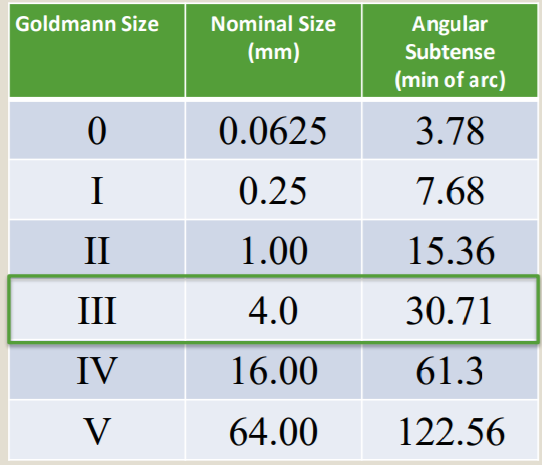
Size of Stimuli
Can be described in terms of
Equivalent to Goldmann bowl perimeter target size
Diameter in mm
the angle subtended at the eye
Is situated in the background surface
Flat
Bowl (curved)
Converting stimulus diameter into the angle subtended the testing distance needs to be known (usually around 33cm)
There is a simple relationship between a stimuli size and the sensitivity needed for the eye to see it
Spatial summation
The larger the size the easier it is to see
The lower the threshold
Neural elements in the retina sum information
Bright small stimulus
Large dim stimulus
Spatial summation varies across the retina
In the dark adapted eye
30 minutes of arc at the fovea
60 minutes of arc in the periphery
In the light adapted eye summation and eccentricity are linear in relationship
Ricco’s Law - Luminance x Area = Constant
______means the the larger the size the easier it is to see and the lower the threshold. Bright ______ stimulus and Dim ______stimulus.
Spatial summation; Small; Large
Stimuli Presentation Time
A stimulus can appear brighter the longer it is presented
Critical duration time summation
This time has a limit though
Critical Duration of Vision
Human eye ~100ms
Luminance and duration relationship according to Bloch’s law
There is no addition to the brightness of the stimulus to presenting it for longer after this critical duration
Bloch’s Law - Luminance x Duration = Constant
Most stimuli have a presentation time of 200ms
Temporal summation and critical duration vary
stimulus size
Background luminance
Retinal location
The larger the stimulus the shorter the critical duration
The higher the background luminance the shorter the critical duration
If the presentation time of a stimulus is longer than the critical duration then it is only necessary to specify a stimulus luminance
We have strong reactions to look at stimuli
A reflex
The orientating reflex
This saccade takes about 250ms
The ideal presentation time
Longer than 100ms
Shorter than 250ms
Most fields tests use a presentation time of 200ms
If the stimulus is too fast or too slow it can be missed and seem smaller than it is.
The ideal stimulus presentation time is longer than ______ but shorter than _____.
100ms; 250ms
Stimulus Sensitivity
Intensity = how bright a stimulus is
Given as luminance • How much light is given out
The intensity of a stimulus tells us about how sensitive the retina the light is falling on, is able to detect it
As the stimulus gets dimmer the eye needs to be more sensitive to be able to detect it
Sensitivity within the visual field is the inverse of stimulus intensity
As the sensitivity of the eye goes up it is capable of seeing dimmer and dimmer stimuli
Sensitivity of the eye is therefore described in terms of how dim the stimulus is
By the stimulus intensity (i.e., luminance)
Unit: decibel (dB)
0dB=10,000asb to 51dB=0.08asb (stimulus intensity)
Sensitivity is described as the dimmest stimulus (1dB) seen according to that stimulus’s intensity
The limit of sensitivity is described as the threshold
The Fovea is most sensitive in normal room illumination
Limit of foveal vision: 40 dB
Limit Normal vision range: 20 dB to 38 dB
Limit Typical range of abnormal vision: 0dB to 30 dB
Limit Maximum perimeter brightness: 0dB
Sensitivity is the dimmest stimulus or smallest _______ seen according to the stimulus’ intensity.
Decibel
Why Decibels not Apostilbs?
Luminance
Stimulus intensity
Apostilbs
Sensitivity
Retinal locations
Decibels (dB)
Sensitivity scale (dB)
Decibel scales go up as the intensity scale goes down
High sensitivities are therefore represented by higher numbers
Eye works in a log not linear manner
Decibel scales go up as the intensity scale ______.
Goes Down
Standard ________ are commonly used in automated static
perimetry and have two reversals.
Standard Staircase
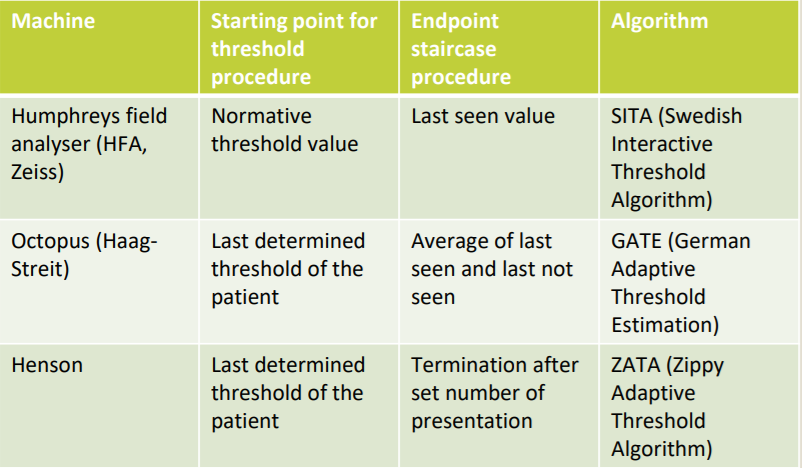
Visual field machines use either full threshold or supra threshold algorithms
The HFA uses _________ algorithm and the staircase endpoint is __________.
The Octopus uses _________ algorithm, and the staircase endpoint is _________.
The Henson uses ________algorithm, and the staircase endpoint is _________.
SITA (Swedish Interactive Threshold Algorithm); Last Seen Value; GATE (German Adaptive Threshold Estimation); Average of Last Seen and Last Unseen; ZATA (Zippy Adaptive Threshold Algorithm); Termination After a Set of Numbers
Single or Multiple Stimulus:
Single stimulus
Locations change
Stimulus intensity changes
Full threshold tests present single stimulus and gather information at a location at a time
Suprathreshold tests are estimating field ‘goodness’ or ‘badness’
Suprathreshold tests lend themselves to screening
Sifting the (probably) normal from the (probably) abnormal
Speed is of the essence
Multiple stimuli strategies take half the time for the same number of stimuli
The price of a quicker test is accuracy
The price of accuracy is an increased testing time
Multiple stimulus strategies have to balance
The extent of the supra threshold increment
The accuracy of the initial threshold element
The time taken for the initial threshold measurement
Suprathreshold tests are mostly for ________.
Screening
Static visual fields are either ______ or _______.
Full threshold; Suprathreshold
Monocular Vision Loss - the inability to see with one eye
Bitemporal Hemianopia - a condition where vision is impaired in the outer (temporal) halves of both visual fields.
Contralateral Homonymous Hemianopia - a visual field loss where the same half of the visual field is affected in both eyes
Contralateral Superior Quadrantopia - a visual field defect where a person loses vision in the upper quadrant of their field of view (on the same side)
Contralateral Inferior Quadrantopia - a visual field defect where a person loses vision in the lower quadrant of their field of view (on the same side)
Neoplasm and inflammatory process cause _______, _______ and _______.
Contralateral Homonymous Hemianopia; Contralateral Superior Quadrantopia; Contralateral Inferior Quadrantopia
The neural organisation in the retina is relative to the ________.
Horizontal
Glaucoma
The most common reason for a visual field defect is glaucoma
Progressive optic nerve damage with characteristic visual field changes
Nasal step -a relative depression or loss of vision in the nasal (towards the nose) part of the visual field, especially along the horizontal meridian (the imaginary line running across the center of the field
Arcuate - a specific pattern of visual field loss, often associated with glaucoma, where there's a "step" or a sudden drop in vision along the horizontal meridian
Paracentral - a specific pattern of vision loss where a "step" or "drop" in sensitivity occurs near the center of the visual field, within about 10 degrees of the point of fixation
Overall depression of the field (in the end stages)
Typically first evident within the central 30o
In the binocular visual field the locations of defects are usually ..
Where the information from the two eyes overlap, and therefore ..
Symptomless until advanced
The most common reason for a visual field defect is _______.
Glaucoma
Disc Edema shows an enlarged _______.
Blind Spot
For diabetic macula edema a 10-2 can be done. It is a type of full-threshold test thatassesses the central 10 degrees of the visual field with 68 closely spaced points. True or False?
True
For _________, ________ and _________ a full threshold 30-2 test could be done
Central Serous Chorioretinopathy; Diabetic Retinopathy; Optic Neuritis
Optic Neuritis can cause a ____________ VF defect.
Central Scatoma
A _____________ can cause a bitemporal hemianopia.
Pituitary Adenoma
3rd Cranial Nerve Palsy and Pituitary Adenoma can cause a bitemporal qaundrantanopia. True or False?
True
Metastasis can cause Left Contralateral Homonymous Hemianopia and it can be assessed using the full threshold _________ test.
30-2
A stroke can cause a Homonymous superior quadrantanopia (pie in the sky) visual field defect.True or False?
True
Confrontation VF
Gross fields test, manual method
Kinetic/static strategy
Gross field defects
Recent onset hemianopia
Recent onset quadrantanopias
Field results that don’t make sense
Artefacts
Poor witnesses
Confrontation procedure
Examiner sits directly opposite patient, 1m away
One eye should be occluded
Examiners eye on the same side should be occluded
Examiner introduces a target and compares own field with patient’s field
Finger counting (static)
Hat pin (kinetic)
Quick screening and domiciliary exams
Examiner compares own VF to that of patient
Target moved in flat plane
Note any changes in fixation
Can be performed anywhere
Can detect extinction phenomenon
Sensitivity is low 50-60%
Confrontation VF has low sensitivity. True or False?
True
Assessment of the Central 10 Degrees (Amsler)
Paper or electronic based
Central defects can be mapped
High rate of false positives
Distortion reported with no active pathology
Simple and quick
Good aide memoir for monitoring for change
10cm square subdivided into 20X20 square
Each box represents 1 degree at 30cm.
Wear NV spectacles
Sensitive to macular pathology
With the chart at 30cm away
Monocularly tested
Near correction used
Fixate on the central spot
Describe if any of the lines are distorted or broken
Questions: can you see the central dot? Can you see all four quadrants whilst looking at the dot? Looking at the dot- are any lines wavy or missing? Do any squares appear strange (blurry, moving, different colour)?
The amsler test is done at 30cm away. True or False?
True
Artefacts and Extraneous Factors
There are a number of common artefacts that confound field results
Test related
Defocus
Lens artefacts
Fixation
Adaptation
Patient related
Pupil size
Lids and Brows
Fatigue
Learning effects
There are a number of other factors to take into account
Age
Angioscotoma
The are numerous artefacts that affect VF results. True or False?
True
The abolsute scotoma is the _________ and it is 15 degrees temporally to fixation.
Blind Spot
The Henson 900 is a ___________ stimuli VF test.
Multiple
Humphrey Fields Analyser (HFA)
Automated
Patient presses the button when they see the light
HFA Screening Strategies
Central 40 Point Screening Pattern
C-40
Central 64 Point Screening Pattern
C-64
Central 76 Point Screening Test Pattern
C-76
Full Field HFA
HFA Central 81
HFA Central 120
HFA Central 135
HFA Central 246
HFA is automated. True or False?
True
Suprathreshold without Quantification
Seen
Missed
Suprathreshold with repeat
Real miss?
Suprathreshold with Quantification
Missed stimuli presented at a higher intensity increment
In specific categories (steps)
Full threshold strategy
Go to fullthreshold when no supra has passed. True or False?
True
Visual Field and Driving - Esterman
‘Functional scoring system' is the current gold standard for testing binocular visual fields
Used by many national driving authorities
UK: px declares eye condition according to ‘driving eyesight rules’ and will get a notification from DVLA
Esterman test
Automated suprathreshold test
Single very bright stimuli (10dB)
120 locations within the visual field
Spread over +/-75o horizontally
35o superiorly
55o inferiorly
Patient fixates centrally
Test time of around 4 to 5 minutes
Group 1 license
A minimum horizontal fields of vision of 120o , horizontally 50 degree left and right and 20 degree up and down
no significant defect within 20o of fixation
'Pass’ Esterman protocol
Scattered single missed points
A single cluster of up to three contiguous points
Significant central loss (Fail)
A cluster of four or more contiguous points that is either wholly or partly within the central 20o area
Loss consisting of both, a single cluster of three contiguous missed points up to and including 20o from fixation and any addition separate missed points with the central area
Central loss of any size that is an extension of an hemianopia or quadrantanopia
To pass you can’t miss more than a cluster of 3 points. True or False?
True
Testing Algorithims in Static Strategies
A process or set of rules to be followed in calculations or other problem solving operations
Visual fields use either threshold or supra threshold algorithms
Threshold
Measures the intensity of the dimmest stimulus which can be tested/seen 50% of the time at each test location
Full Threshold
Estimate of threshold at a whole series of different retinal locations
Monitoring extent of visual field loss
Suprathreshold
The intensity of the light at each location is pre determined at a level above threshold
Is the stimulus visible or not?
Screening
Supra threshold is for ______.
Screening
It takes half the time of a full threshold with SITA. True or False?
True
SITA uses staircase procedure based on predictive probability (knowledge of normal age-related controls)
Comes in 3 versions
SITA standard: 4-2 staircase (~7min); glaucoma diagnosis and monitoring progression
SITA fast: 6-3 staircase (less stimulus presentations needed, ~4min); tends to underestimate scotomas, also used for glaucoma monitoring
SITA faster: 6-3 staircase, no False Negative testing and no blind spot testing (~2min)
Sita standard 4-2 staircase is for glaucoma diagnosis and monitoring progression. True or False?
True
Automated Perimetry Advantages
Reproducibility results
Quantitative information
Results in a more timely manner
Experienced visual fields operator not require
Earlier detection of defects
There are many more advantages to automated perimetry than manual. True or False?
True
Reliability Indicies:
High Fixation loss 15% to 20% or more
Acceptable False Positive 5-10%
Acceptable 10-15% (patient not paying attention) False negative
False negatives increase when patients not paying attention. True or False?
True
A _________ can cause a generalised reduction in sensitivity.
Cataract
____________ value becomes more negative as field loss worsens.
Mean Deviation
____________ is useful in local loss progression and early glaucoma.
Pattern Standard DEviation (PSD)
______________ is similar to MD. 100% represents normal and it case be used as an indicator for progression.
Visual Field Index (VFI)
Glaucoma Hemifield Test:
Indicator of the differences between the superior and inferior halves of the field
Hemifield
Points on the field plots are clustered into 10 regions
Mirror of clusters in the top and bottom hemifield
Compared with the corresponding cluster in the opposite hemifield
GHT outcomes
Outside normal limits
Borderline
General reduction in sensitivity
Abnormally high sensitivity
Within normal limits
Outside normal limits
Matched pair difference only found in 1% of normal database
Two of matched pairs more abnormal than 99.5% of normal database
Borderline
Matched pair difference found in 3% of normal database
General reduction in sensitivity
Outside normal limits not met
Best region of plot depressed to level of 0.5% of normal database
Abnormally high sensitivity
Region of plot is better than 99.5% of normal database
Within normal limits
None of the above apply
This test compares the difference between the superior and inferior halves of hemifield. True or False?
True
The order to read a VF result sheet:
.Px (Name, DOB, age, eye), date of test
Strategy, stimulus
Reliability
Defect based on PD and TD plots
Interpretation global indices
DDx (what else could cause this defect)
Additional tests
This is true or False?
True
Need to know:
Kinetic vs static perimetry – stimulus moves vs stimulus stationary
Suprathreshold tests are for screening – they test increments brighter (3, 4 or 6dB)
high specificity but low sensitivity (true defects detected, shallow defects may be missed)
Saves time
Reliability of result judged on ..
Fixation loss <20%
False positive <10%
False negative <15%
Lesions up to chiasm are unilateral (often around the horizontal midline, but not always)
Lesions from chiasm up to occipital lobe show bilateral (i.e., VF of right and left eye) around the vertical midline
Fixation loss less than <20% is acceptable. True or False?
True