chap. 21 - heart, neck vessels
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
heart location
in mediastinum, between the lungs, behind sternum
heavier in males than females
superior + inferior vena cava
returns deoxygenated blood to right atrium
pulmonary artery
carries deoxygenated blood from right ventricle to lungs
pulmonary veins (4)
returns oxygenated blood to left atrium
aorta
carries oxygenated blood from left ventricle to body
cardiac cells
spontaneously generates electrical impulses
conduction
controls the cardiac cycle (filling + emptying of heart chambers)
SA node (pacemaker)
located in right atrium, fires 60-100 bpm, sends impulses across atria for atrial contraction
if node fails → other areas take over but at a slower rate of 40-60 bpm
AV node
sends impulses to bundle of his, slows impulse allowing ventricles to fill
P wave
atrial depolarization = atria contracts
QRS complex
ventricular depolarization = ventricles contract
much larger than P wave bc ventricles have more muscle mass
atrial repolarization occurs but hidden by QRS
T wave
ventricular repolarization = ventricles recover/relax
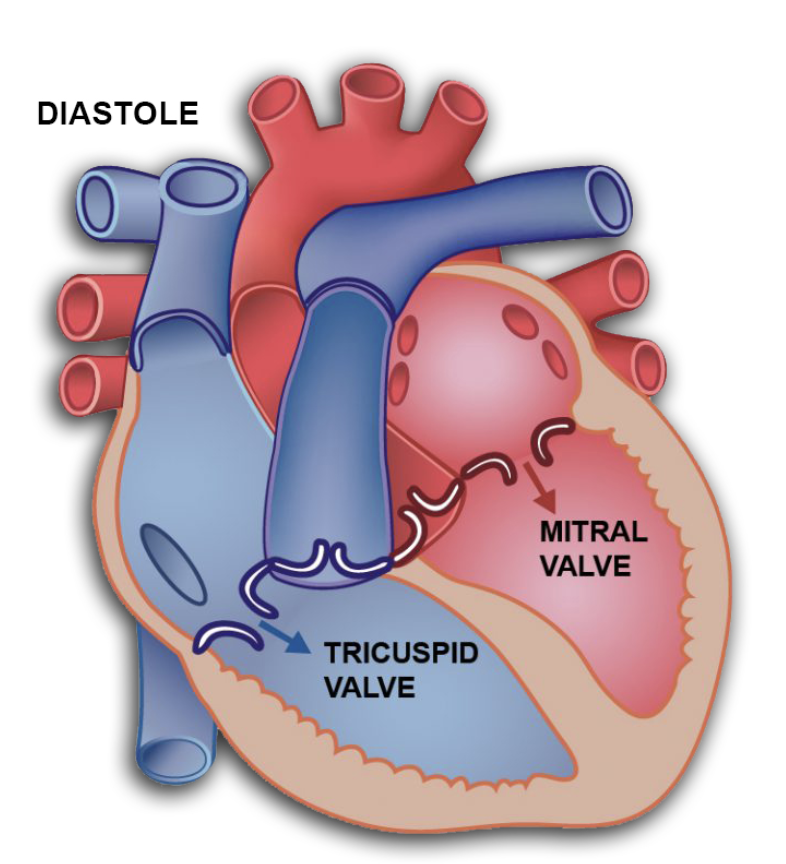
during diastole
AV valves open (mitral + tricuspid)
blood flows from atria to ventricles bc of higher atrial pressure
early filling = fast, passive flow
slow filling = mid-diastole
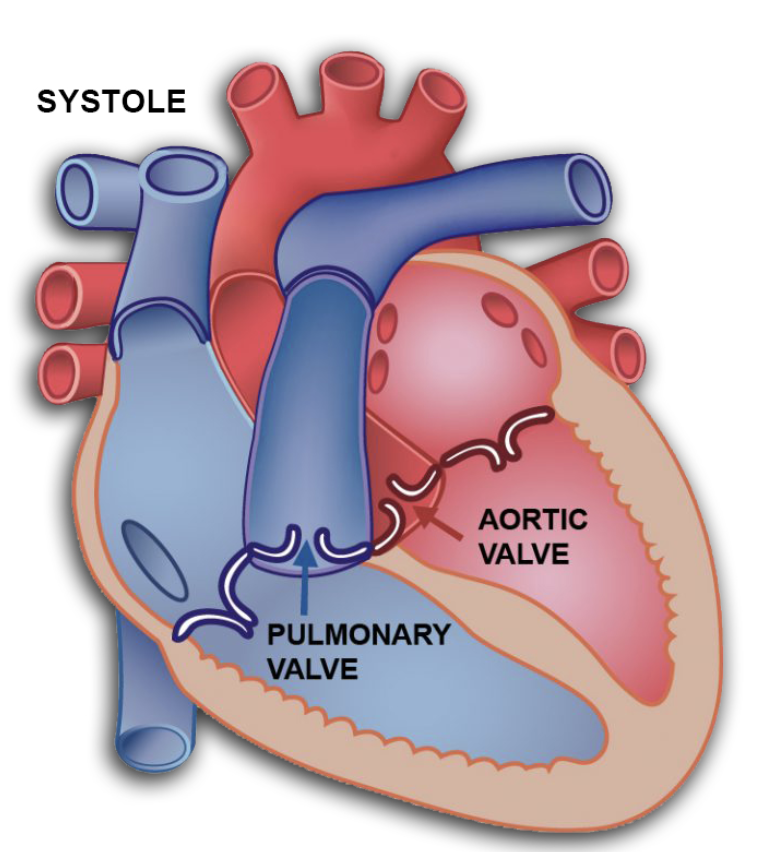
during systole
ventricles fill, pressure rises, and AV valves CLOSE — produces S1 “lub” sounds
ventricular pressure rises and semilunar valves open (aortic + pulmonic)
blood pumped out to body + lungs
ventricles empty, pressure drops, and semilunar vales close — produces S2 “dub” sounds
cycle restarts as AV valves open again
S1 “lub”
closure of AV valves (mitral + tricuspid)
marks the start of systole
heard loudest at APEX
S2 “dub”
closure of SEMILUNAR valves (aortic + pulmonic)
marks start of diastole
heard loudest at BASE
cardiac output
how much blood the heart pumps in 1 min
CO = HR x SV
changes based on body needs:
higher CO → exercise, stress, fever
lower CO → heart failure, shock
CO nervous system control
sympathetic (fight or flight) → increases HR → increases CO
parasympathetic (rest and digest) → decreases HR → lowers CO
stroke volume
amount of blood pumped from heart w/ each contraction
influenced by → stretch of heart muscle before contraction, pressure against which it has to eject blood during contraction, synergy of contraction, compliance or distensibility of ventricles, contractibility of myocardium
aortic area
2nd ICS at the right sternal border → base of heart
pulmonic area
2nd or 3rd ICS at left sternal border → base of heart
Erb’s point
3rd ICS at left sternal border
tricuspid area
4th or 5th ICS at left lower sternal border
mitral (apical)
5th ICS near left MCL → apex of heart
murmur
swooshing or blowing sound caused by turbulent, messy blood flow
murmurs happen due to …
fast blood flow (fever, growth spurts, anemia)
valve problems (too tight = stenosis, leaky = regurgitation)
valve malfunction
openings in the heart that shoudn’t be there (septal defects)
physiologic murmur
innocent murmur
pathologic murmur
congenital or acquired structural heart disease
regurgitation
valve doesn’t close tightly/properly, so blood leaks backward instead of moving forward
systolic murmur
mitral/tricuspid REGURGITATION, aortic/pulmonic STENOSIS
diastolic murmur
mitral/tricuspid STENOSIS, aortic/pulmonic REGURGITATION
DIASTOLIC = ALWAYS BAD
murmur symptoms
heart has to pump extra blood, leading to overload — chambers stretched (dilated)
lead to → fatigue, shortness of breath, decreased cardiac output
S3 - ventricular gallop
caused by rapid filling of the ventricles that are already stretched or overloaded
happens right AFTER S2 (lub-dub-ta) — “kentucky” (S1, S2, S3)
commonly seen in → heart failure, fluid overload, dilated ventricles
NORMAL → children, young adults, pregnancy
NOT normal → older adults
S4 - atrial gallop
caused by atria pushing blood into a stiff, non-compliant ventricle
happens right BEFORE S1 (ta-lub-dub) — “tennessee“ (S4, S1, S2)
common causes → long-standing hypertension, left ventricular hypertrophy, aortic stenosis
NOT normal → any age group
ejection clicks
high-pitched, short sounds during early systole
ex: mid-systole click — often linked to mitral valve prolapse
friction rub
grating or scratchy sound
occurs when inflamed pericardial layers RUB together
may be heard during systole, diastole, or both
heave or lift
visible or palpable movement of chest wall caused by heart pushing strongly against it
occur when heart is working harder than normal
pulse deficit
difference between the apical pulse + a peripheral/radial pulse
indicates heart is beating, but not all beats are generating a strong enough pulse to reach the extremities
seen in → atrial fibrillation, atrial flutter, PVCs, heart blocks
ALWAYS measure apical + radial pulse at the same time
bradycardia
HR <60 bpm → may decrease CO
tachycardia
HR >100 bpm → may decrease filling time + decrease CO
atrial fibrilation
quivering right atrium
atrial flutter
extra rhythmic beats in right atrium
ventricular fibrilation
quivering left ventricle
ventricular tachycardia
extra rhythmic beats in left ventricle
heart rates/rhythms can lead to…
decreased cardiac output
heart failure
risk for emboli (clots)
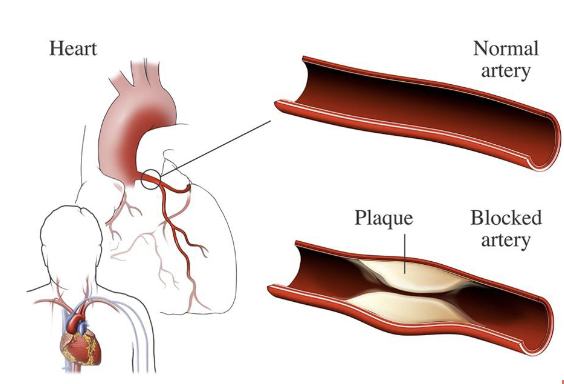
coronary heart disease
narrowing of the blood vessels that supply blood + oxygen to the heart
causing heart attack, chest pain, stroke, affecting heart muscles, valves, or rhythm
screening for risk → cholesterol + glucose level, C-reactive protein presence, BP, health history, PAD
screening starts at 20 for BP, fasting lipoprotein profile, body weight
screening at age 45 for blood glucose every 3 years
coronary heart disease inherited risks
increasing age, heredity (race), diabetes (type 1)
coronary heart disease factors
modifiable → smoking, high cholesterol/triglycerides, hypertension, physical inactivity, obesity, diabetes mellitus (type 2)
contributing → stress, excessive alcohol consumption, diet + nutrition, diabetes mellitus
coronary heart disease s/s
chest pain, shortness of breath, arrhythmia, nausea, dizziness, palpations, fatigue, weakness
coronary heart disease education
prevention, smoking secession, physical activity, weight/BP/cholesterol, alcohol, stress, nutrition
diaphragm of stethoscope
for HIGH-pitched sounds (S1, S2, most murmurs)
bell of stethoscope
for LOW-pitched sounds (S3, S4, some murmurs)
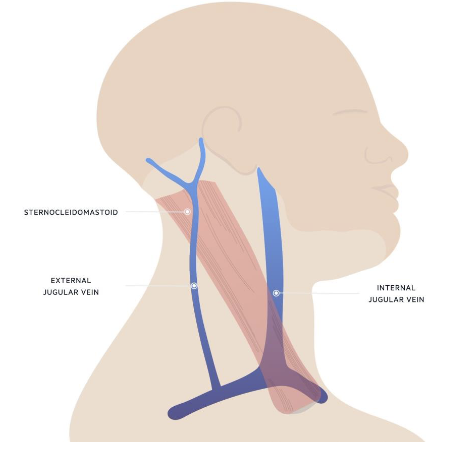
carotid arteries location
in the groove beside the trachea and under the sternocleidomastoid muscle
internal carotid artery
supplies the brain
external carotid artery
supplies the face + neck
normal carotid pulse feels …
smooth, rapid upstroke during early systole
gradual, smooth downstroke
strong + equal on both sides
internal jugular vein location
deep, next to sternocleidomastoid muscle
best for assessing right atrial pressure
jugular venous pressure (JVP)
gives clues about the right side of the heart
right atrial pressure
right ventricular filling
fluid status (volume overload or deficit)
bruit = hear
abnormal whooshing sound HEARD w/ stethoscope
happens when blood is flowing through a narrowed or partially blocked artery
water rushing through a pinched hose (gets noisy)
common causes → atherosclerosis (plaque buildup), narrowed carotid artery, AV fistulas (dialysis access)
thrill = feel
vibration FELT w/ fingertips
cat purring under skin
indicates very turbulent blood flow due to …
severe valve disease (murmurs strong enough to feel)
significant arterial narrowing
AV fistulas with high flow
jugular venous distention
the jugular veins look enlarged or bulging in the neck
common cause → right-sided heart failure
other causes → fluid overload, pulmonary hypertension, tricuspid valve problems, pericardial tamponade (pressure around the heart)
older adult considerations in neck
atherosclerosis may have caused obstruction and compression may easily block circulation
apical impulse may be difficult to palpate due to increased anteroposterior chest diameter