Lecture 34 - Chronic Spontaneous Urticaria
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
what timeline is considered urticarial vasculitis
> 48 hours
how often does a urticarial wheal usually take to resolve
24 hours
what are potential causes of acute urticaria
spontaneous
infection
food
medication
venom
latex
contact
what are potential causes of inducible chronic urticaria
dermatographism
cholinergic
cold induced
solar
aquagenic
exercise
delayed-pressure
what is urticaria driven by
Urticaria is driven by the release of inflammatory mediators from mast cells (histamine**, cytokines, etc.)
what is chronic urticaria characterized by
red , swollen(raised), itchy weals(hives), angioedema or both occurring intermittently for ≥6 weeks
Associated angioedema occurs in approximately 40% of patients
Recurrent angioedema may occur with or without weals
what is chronic spontaneous urticaria
CSU refers to a chronic form of urticaria with no identifiable trigger, with weals present on most days of the week
Can patients experience both spontaneous & inducible forms of urticaria at the same time
yes
what is an important medication to check if a patient is taking when assessing the cause of angioedema
ACEi - especially if they do not have wheals
what do wheals look like in chronic spontaneous urticaria
Can affect any part of the body and are usually widely distributed
Size ranges from a few millimeters to several centimeters and may coalesce
Characterized by central pallor with surrounding erythematous flare
Lesions are transient and typically last minutes to several hours
Individual wheals resolve or change shape within 24 hours
what is angioedema
Deeper swelling of dermis and subcutaneous tissue
More localized than wheals
Common sites include eyelids, lips, hands, feet, and genitalia
Severe cases may involve tongue, pharynx, uvula, or soft palate, posing airway risk
what are the 4 points of chronic spontaneous urticaria assessment
exclude differential diagnoses
assess disease activity and impact on QoL
identify possible triggers or underlying causes
know when to refer
what are important things to consider when trying to exclude differential diagnoses
Confirm lesions are transient wheals resolving within 24 hours and are typically pruritic
Consider alternative diagnoses if lesions last >24 hours, are painful/burning, or leave bruising or hyperpigmentation
what are examples of differential diagnoses
Urticarial vasculitis
Drug reactions (e.g., NSAIDs, ACE inhibitors, antibiotics)
Serum sickness–like reactions
Viral exanthems or infection-related urticaria
Dermatitis
what step therapy is recommended in guidelines for urticatia
standard dose 2nd gen antihistamines
up-dose 2nd gen antihistamines (up to 4x)
add biologic: omalizumab
consider cyclosporin if inadequate control
a short course of glucocorticoids may be considered in cases of severe exacerbation
what medications are associated with urticaria
NSAIDs
ACEi
antibiotics
what infections are associated with urticaria
viral illnesses
URTIs
what autoimmune conditions are associated with urticaria
thyroid disease
autoimmune urticaria
what physical triggers (inducible urticaria) can occur simultaneously with CSU
pressure
cold
heat
exercise
what lifestyle factors may trigger urticaria
stress
alcohol
sleep deprivation
what are s/s that warrant urgent referral
Signs of anaphylaxis
Airway involvement (tongue swelling, throat tightness, dyspnea)
Rapidly progressive angioedema
what are s/s that warrant specialist referral
Symptoms persist despite 4× antihistamine dosing
Suspected urticarial vasculitis (lesions >24 hours, painful, bruising)
Recurrent angioedema without wheals
what medications may be considered for patients who may require advanced therapy
Consider referral for omalizumab
Consider cyclosporine in refractory disease
do guidelines recommend 1st gen or 2nd gen antihistamines for urticaria
2nd generation
studies show efficacy and improved safety profiles
what are adverse effects of 1st gen antihistamines
CNS:
decreased alertness, cognition, learning, memory, psychomotor performance
increased impairment with or without sedation
Muscarinic: dry mouth, urinary retention, sinus tachycardia
Serotonin receptors: increased appetite, weight gain
alpha-Adrenergic receptors: dizziness, postural hypotension
Cardiac: increased QT interval, ventricular arrhythmias
do sedating first gen antihistamines improve sleep quality
No → Negatively Impact REM Sleep
no benefit in combining with 2nd gen antihistamines, and greater incidence of daytime somnolence
is it better to increase 1 antihistamine dose to 4x the typical dose OR stack different antihistamines
Guidelines recommend up dosing antihistamines (up to 4x daily)
what is the MOA of antihistamines in chronic spontaneous urticaria
Block H₁ histamine receptors on target cells (vascular endothelium, sensory nerves, smooth muscle)
Act as inverse agonists, stabilizing the inactive conformation of the H₁ receptor
Reduce histamine-mediated effects, including: vasodilation, increased vascular permeability, pruritus, wheal formation
Inhibit mast cell mediator effects, limiting downstream inflammatory signaling
Decrease sensory nerve activation, reducing itch
what is the overall effect of antihistamines in CSU
suppression of wheal formation and pruritus in CSU
what are Rx 2nd gen antihistamines
Bilastine (Blexten)
Cetirizine
Rupatadine (Rupall)
what are OTC 2nd gen antihistamines
Cetirizine
Desloratadine
Fexofenadine
Loratadine
what 2nd gen antihistamine has the highest risk of sedation
cetirizine (+rupatadine?)
what is the dose of bilastine
20mg daily
max: 80mg daily
Take 1 hour before or 2 hours after food
what is the dose of cetirizine
10mg daily
max: 40mg daily
what is the dose of deslortadine
5mg daily
max: 20mg daily
what is the dose of fexofenadine
180mg daily
max: 720mg daily
what is the dose of loratadine
10mg daily
max: 40mg daily
what is the dose of rupatadine
10mg daily
max: 40mg daily
Only antihistamine with PAF (platelet aggregating factor) blockade
what is omalizumab
SC injection
Anti-IgE monoclonal antibody → binds free IgE → ↓ mast cell & basophil activation
may take 4-12 weeks to work
what is the dose of omalizumab
150-300mg q4 weeks
what is cyclosporine
oral agent
Calcineurin inhibitor → ↓ T-cell activation → ↓ cytokine release
Reserved for severe refractory CSU; effective but limited by toxicity
what is the dose of cyclosporine
3-5mg/kg/day (divided)
how can antihistamine therapy be optimized
Counseling
Take daily (not PRN) for optimal control
May require up-dosing up to 4× standard dose per guidelines
Onset may take several days to weeks
what are safety counselling points for antihistamines
Generally well tolerated
Minimal sedation compared to first-generation agents
Avoid combining with first-generation antihistamines
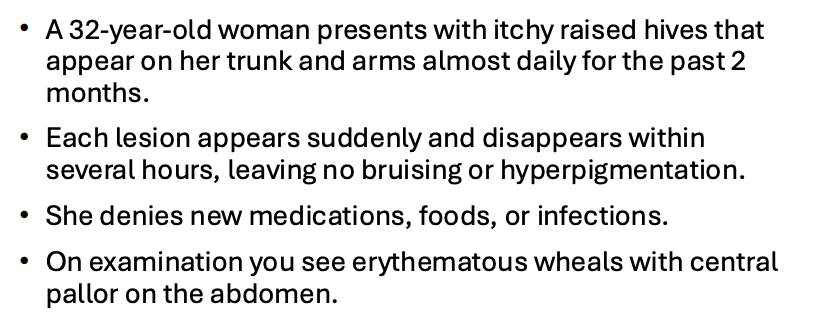
What is the most likely diagnosis?
A. Urticarial vasculitis
B. Chronic spontaneous urticaria
C. Contact dermatitis
D. Drug hypersensitivity reaction
B. Chronic spontaneous urticaria
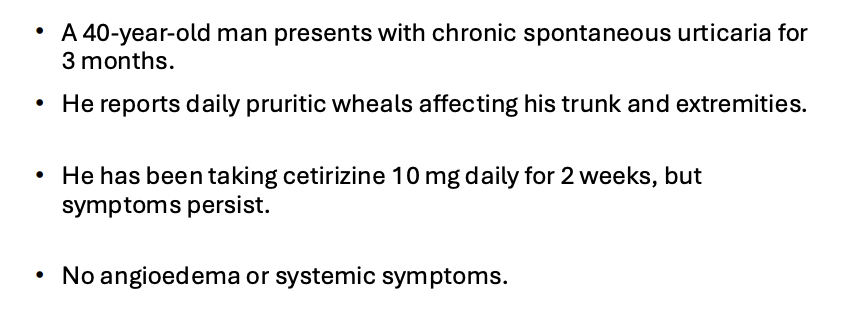
What is the next best management step according to international urticaria guidelines?
A. Add hydroxyzine at night
B. Increase cetirizine up to fourfold dose
C. Start systemic glucocorticoids
D. Add montelukast
B. Increase cetirizine up to fourfold dose
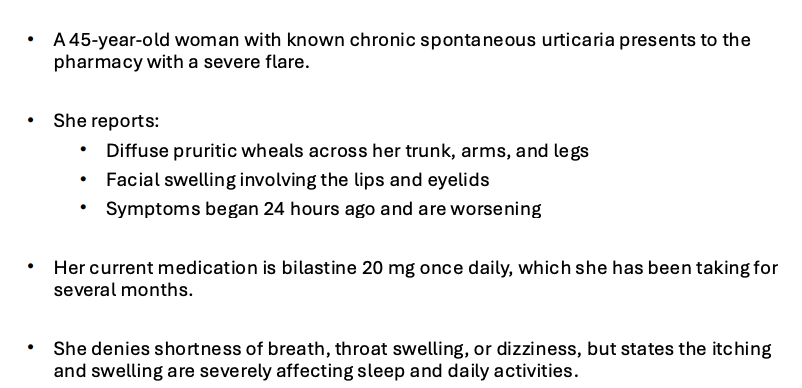
What is the most appropriate management recommendation at this time?
A. Add hydroxyzine at night
B. Increase bilastine up to fourfold dose and initiate a short course of oral glucocorticoids
C. Continue bilastine at the same dose and reassess in one week
D. Stop bilastine and switch to a different antihistamine
E. Increase bilastine up to fourfold dose
B. Increase bilastine up to fourfold dose and initiate a short course of oral glucocorticoids