BIOL204 EXAM 2 MATERIAL
1/67
Earn XP
Description and Tags
LEC6-11
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
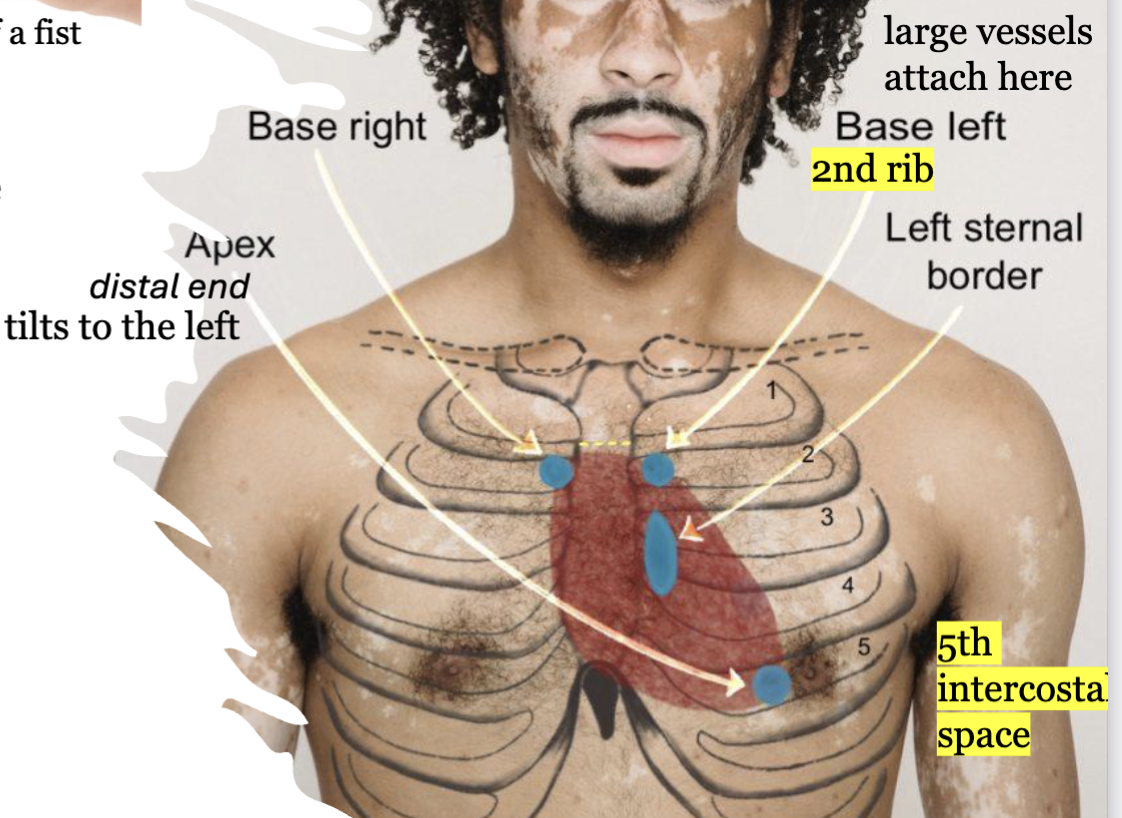
LEC 6: describe the general location, size, and shape of the heart
The heart is located in the middle mediastinum of the
thoracic cavity, within the pericardial cavity.
The heart is the size of a fist.
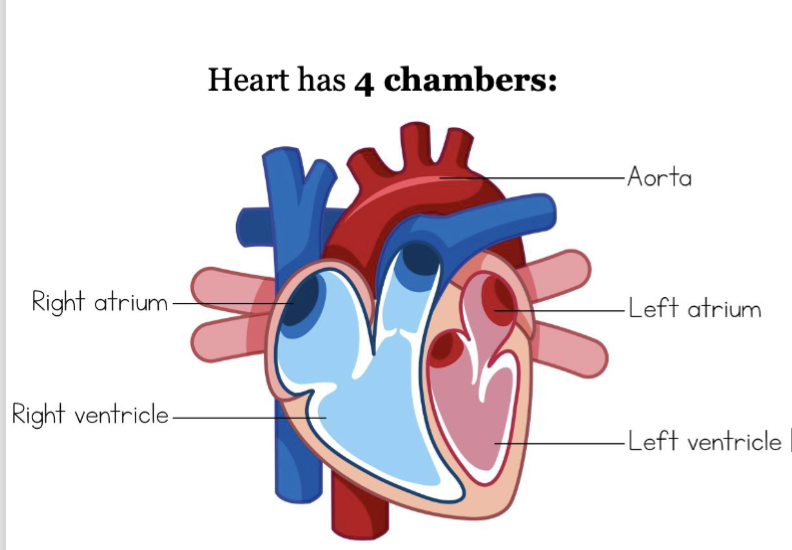
LEC 6: Identify the 4 chambers of the heart
left and right atria: thin upper chambers that receive blood returning to the heart through veins
left and right ventricles: thick, muscular lower chambers that pump blood out of the heart through arteries (away)
septa: muscular wall that divides the left and right side of the heart
functionally, the heart is a double pump
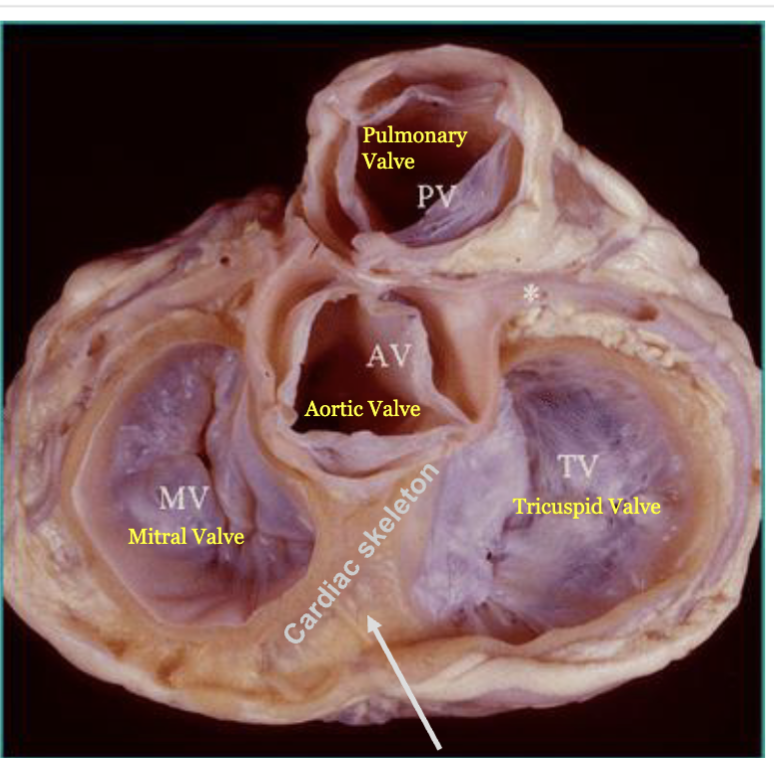
LEC 6: Identify the four heart valves, their structure, functions, and locations
Valves of the Heart – allow one-way flow of blood (respond passively to pressure gradients)
semilunar (SL) valves
function: prevent backflow into the ventricles when the ventricles are relaxing
1 heart valve: pulmonary valve
structure: honestly, like a round stomach with the beginning of big thighs (oval overall)
location: right ventricle - pulmonary artery
2 heart valve: aortic valve
structure: circle split equally into 3
location: left ventricle - aorta
atrioventricular (AV) valves
function: prevent backflow into the atria when the ventricles are contracting
3 heart valve: tricuspid valve
structure: honestly, gooch and thighs in a circle (3 cusps)
location: right AV valve
4 heart valve: mitral valve
structure: honestly, thick buns with a crack in the middle
location: bicuspid or left AV valve
4 valves are located within the cardiac skeleton (=fibrous skeleton) (connective tissue), stabilize their positions - prevents overdilation
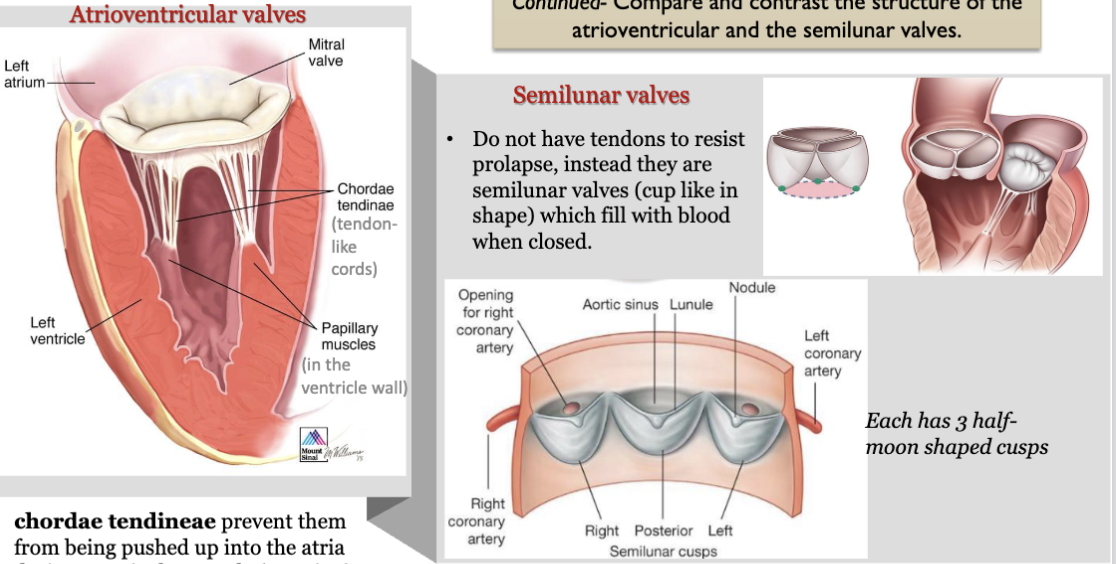
LEC 6: Compare and contrast the structure of the atrioventricular and the semilunar valves
AV valves: chordae tendineae prevent them from being pushed up into the atria during ventricular systole (eversion)
SL valves: do not have tendons to resist prolapse, instead they are SL valves (cup shape) which fill with blood when closed (each has 3 half moon shaped cusps)
pulmonary valve: it has 3 flaps/cusps that open and close to control blood flow (gooch and thighs), mediates flow between the right ventricle and pulmonary artery
LEC 6: Describe the pericardium and its two layers
pericardium: sac-like structure wrapped around heart, made up of the outer fibrous pericardium and the inner serous pericardium (parietal and visceral layers)
fibrous pericardium: encloses the heart (like a bag)
pericardial cavity: contains pericardial fluid reducing friction
visceral layer of serous: coronary blood vessels travel through this layer
LEC 6: State the three layers of the heart wall
pericardium/epicardium - outer
myocardium - middle
endocardium - inner, continuous with endothelium in vessels
LEC 6: Analyze the structural characteristics of cardiomyocytes
short, thick, branched cells… mass of glycogen, theres intercalated discs striations, nucleus
almost totally dependent on aerobic metabolism (need oxygen) for energy
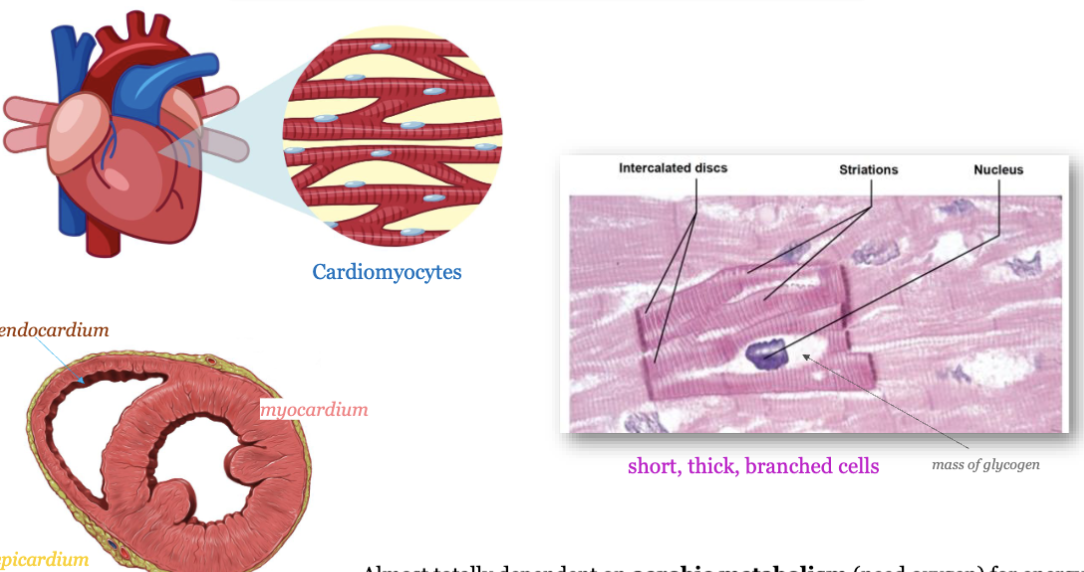
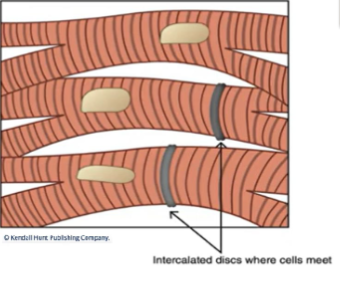
LEC 6: Analyze the role of intercalated discs connecting cardiomyocytes
specialized adhesive junctions - connect adjacent cardiac cells
specialized cell junctions - anchor cardiac muscle cells together
protein channels that connect the cytoplasm of neighboring cells allow electrical signals to pass directly from one cell to another, enabling rapid and synchronized contractions of the heart muscle - cells function together as single unit = functional syncytium
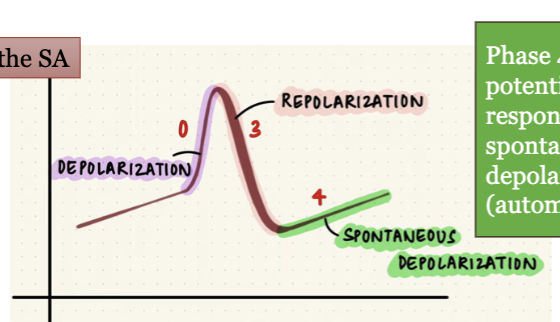
LEC 6: List the phases of the cardiac muscle action potential and explain the ion movements that occur in each phase
resting membrane potential
phase 0: rapid Na+ influx through open fast Na+ channels
phase 1: transient K+ channels open and K+ efflux begins to return the membrane potential to 0 mV
phase 2: influx of Ca2+ through channels balances the K+ efflux to create the plateau phase
phase 3: Ca2+ channels close and rectifier K+ channels remain open to return the membrane potential to -90 mV
phase 4: K+ rectifier channels maintain the negative resting potential (Na-K ATPase)
each phase results from a change in the balance of inward and outward ionic currents that become activated upon membrane depolarization
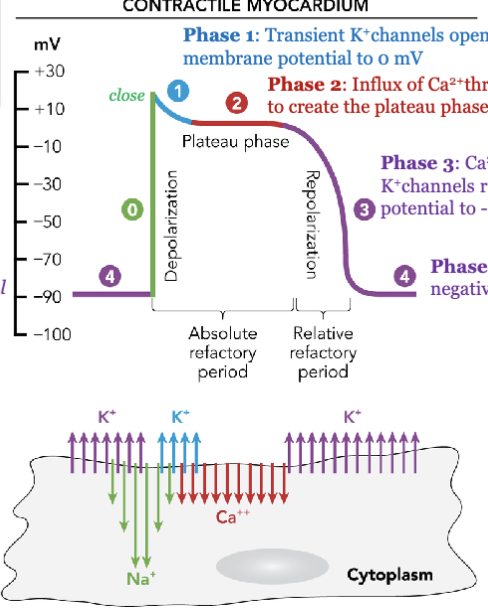
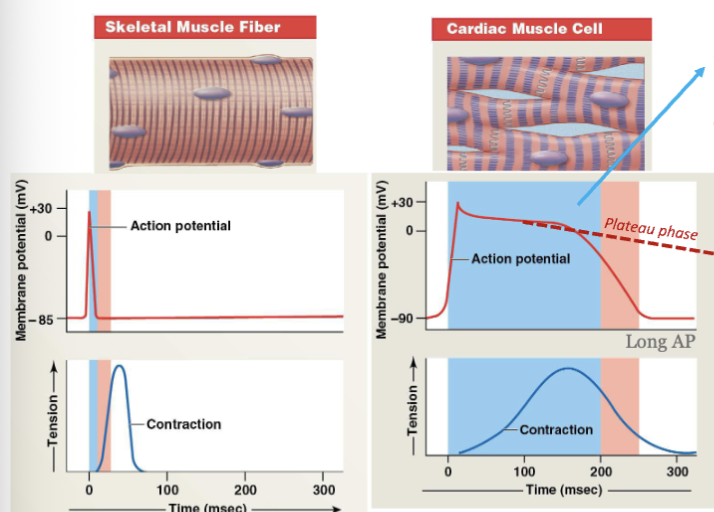
LEC 6: Explain the significance of the long absolute refractory period and the plateau phase in the action potential of a cardiac contractile cell
significance of long absolute refractory period: the interval of time during which a second action potential cannot be initiated → helps to prevent the heart from entering a state of rapid and disorganized contractions (fibrillation)
significance of plateau phase: unique for cardiac cells which allow enough calcium influx for a strong, sustained contraction to pump blood efficiently → this ensures that the ventricles have sufficient time to squeeze blood out efficiently with each beat
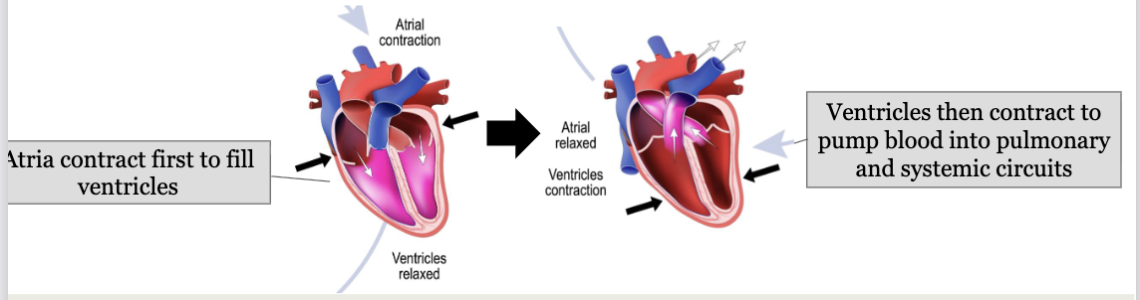
LEC 6: Describe in detail one complete cycle of heat contraction and relaxation (cardiac cycle)
cardiac cycle: the sequence of events that occur during one complete heartbeat
occurs in 2 phases:
contraction (systole) - blood leaves the chamber
relaxation (diastole) - blood refills chamber
pressure changes promote blood flow and valve opening and closing
-fluid will only flow if there is a pressure gradient (pressure difference)
-fluid flows from high-pressure to low-pressure joint
LEC 6: What is the cardiac cycle?
1) all chambers relaxed; AV valves open; ventricles fill passively to ~70%
2) atrial systole: atria contract together; finish filling ventricles
3) ventricular systole: first phase. contracting ventricles push AV valves closed but not enough pressure to open the SL valves
4) ventricular systole: second phase. increasing pressure opens SL valves; push blood into the pulmonary and systemic circuits; atria are relaxed (diastole) and filling
5) ventricular diastole: early. ventricles relax and their pressure drops; blood in aorta and pulmonary trunk backflows, closes SL valves
6) all valves closed; no volume change; blood passively filling atria
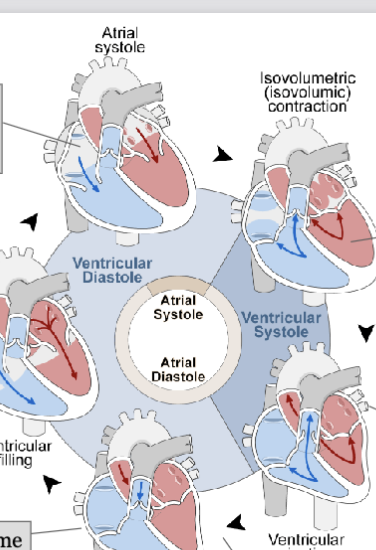
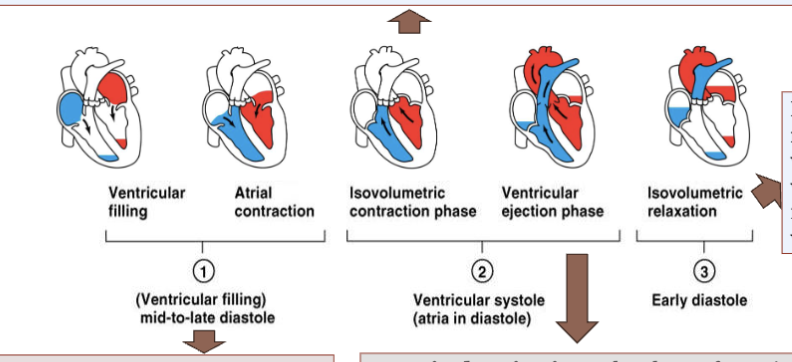
LEC 6: Explain the following concepts: end-diastolic volume, isovolumetric contraction, ventricular ejection, and isovolumetric relaxation
end-diastolic volume (EDV): the amount of blood in the ventricle at the end of diastole
isovolumetric contraction: the initial phase of ventricular contraction where the muscle fibers contract but the valves remain closed, resulting in no change in ventricular volume. it builds tension in the heart muscle, preparing it to eject blood
ventricular ejection: the phase of ventricular contraction where the aortic and pulmonary valves open, allowing blood to be ejected from the ventricles into the aorta and pulmonary artery (blood is pumped throughout body)
isovolumetric relaxation: the ventricles relax, but valves remain closed, resulting in no change in ventricular volume
LEC 6: Indicate what causes the sounds of the heartbeat
the closing valve cusps DO NOT make sound → the sound is made by TURBULENCE OF BLOOD HITTING a closed valve or RAPIDLY FILLING a chamber
when AV valves close; marks start of ventricular contraction = lubb (louder and longer)… when SL valve close = dupp (softer and sharper)… ventricular filling sound… inaudible (normal) audible (usually abnormal) = atrial gallop, occurs during active LV filling when atrial contraction forces blood into a noncompliant LV ← last 2 very faint
abnormal heart sounds, MURMURS, indicate problem with heart valves
valve problems cause valves to LEAK (regurgitation) or to NARROW (stenosis), which can lead to turbulent blood flow and create abnormal sounds

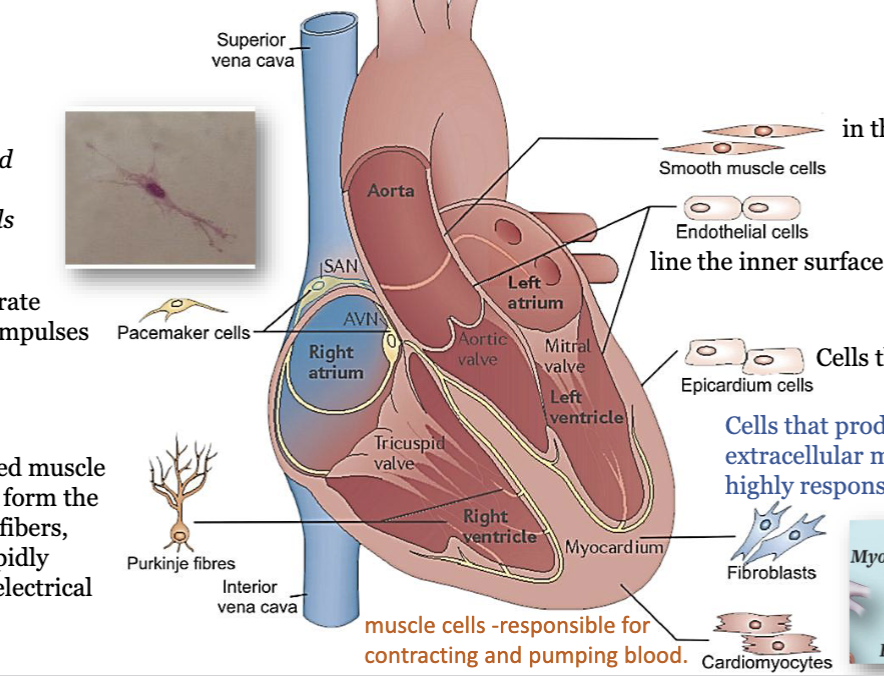
LEC 7: Identify the various cell types in the heart
smooth muscle cells: in the walls of blood vessels
endothelial cells: line the inner surface of heart and blood vessels
epicardium cells: cells that form the epicardium
fibroblasts: cells that produce and maintain the extracellular matrix (ECM). they are highly responsive to cardiac injury
cardiomyocytes: muscle cells, responsible for contracting and pumping blood
purkinje fibres: specialized muscle cells that form the Purkinje fibers, which rapidly conduct electrical impulses
pacemaker cells: they generate electrical impulses, spider- and spindle-shaped cells
LEC 7: Explain why the SA node normally paces the heart
auto-rhythmicity: cardiac muscle’s ability to contract at its own pace independent of neural or hormonal stimulation
conduction system consists of CONDUCTING CELLS which are nerve-like conduction pathways (made of modified cardiomyocytes) through the myocardium
PACEMAKER aka sinoatrial node (SA): sets the rate of the heartbeat (sinus rhythm), firing at 100 bpm, SA has fastest rate of spontaneous depolarization
LEC 7: List the parts of the electrical conduction system of the heart in the correct sequence for one contraction and explain how the electrical conduction system functions
1) PACEMAKER/SA: generates electrical impulse, spreads through the atria
2) BACHMANN BUNDLE/INTERATRIAL BUNDLE: helps spread the impulse to the left atrium
3) AV node: impulse reaches the AV node, which delays the impulse
4) bundle of His: delayed impulse travels through the bundle of His
5) Purkinje fibers: then through Purkinje fibers to the ventricles, causing them to contract
speed of depolarization AV > bundle of His > Purkinje fibers
LEC 7: Understand the differences between the two types of cardiac action potentials (muscle cells vs. pacemaker cells), including the role of the pacemaker potential in the SA node’s automaticity
the heart has 2 types of AP:
1) muscles of atria and ventricles where they got plateau, contractile cells
2) in the pacemaker of heart aka SA, conducting cells
phase 4: “pacemaker potential,” bc it is responsible for the spontaneous repetitive depolarization (automaticity)
certain NONcontractile cardiac muscle cells exhibit automaticity and rhythmicity and can independently initiate APs bc their resting mb potential (RMP) is unstable bc it never “rests” = pacemaker potential
automaticity is due to the fact that these cells start leaking Na+ into cell as soon as they return to resting state
LEC 7: Define electrocardiogram (ECG or EKG)
electro - electrical activity
cardio - heart
gram - written record
ECG recording = sum of all the electrical potentials generated by all the cells of the heart at any instance in time
creates tiny voltage changes that are picked up by electrodes
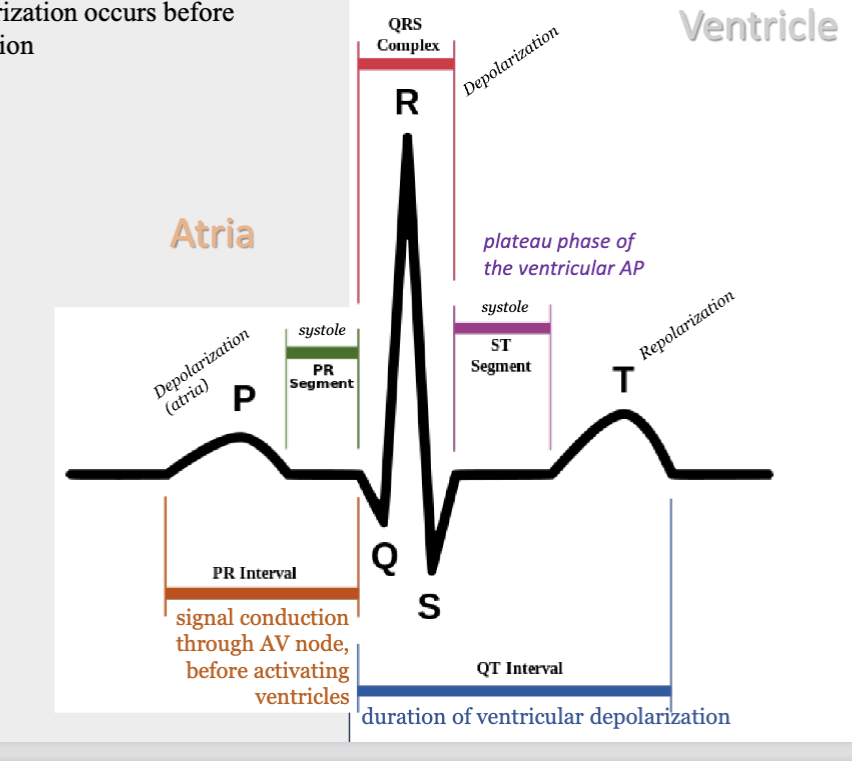
LEC 7: Name the waveforms in a normal ECG and relate the electrical events to the normal mechanical events of the cardiac cycle
P wave = corresponds to the atrial depolarization phase of the cardiac AP
PR segment - atrial systole
PR interval - signal conduction thru AV node before activating ventricles
QRS complex = indicates ventricular depolarization and some atrial repolarization
ST segment - ventricular systole
T wave = represents ventricular repolarization
DEPOLARIZATION BEFORE MECHANICAL CONTRACTION
LEC 7: Define HR, heart rhythm, heart beat, fibrillation
heart rate (HR): calculated from R wave to R wave. a normal resting HR is 60-100 bpm
heart rhythm: electrical activity that underlies the mechanical function of heart
heartbeat: physical contraction and relaxation of heart muscle, which pumps throughout the body. its the mechanical action of heart
arrhythmia: extra or missed beat or FIBRILLATION when atria/ventricles contracting in uncoordinated fashion
sinus tachycardia >100 bpm
sinus bradycardia <60 bpm
sinus arrythmia: unequal time btwn beats
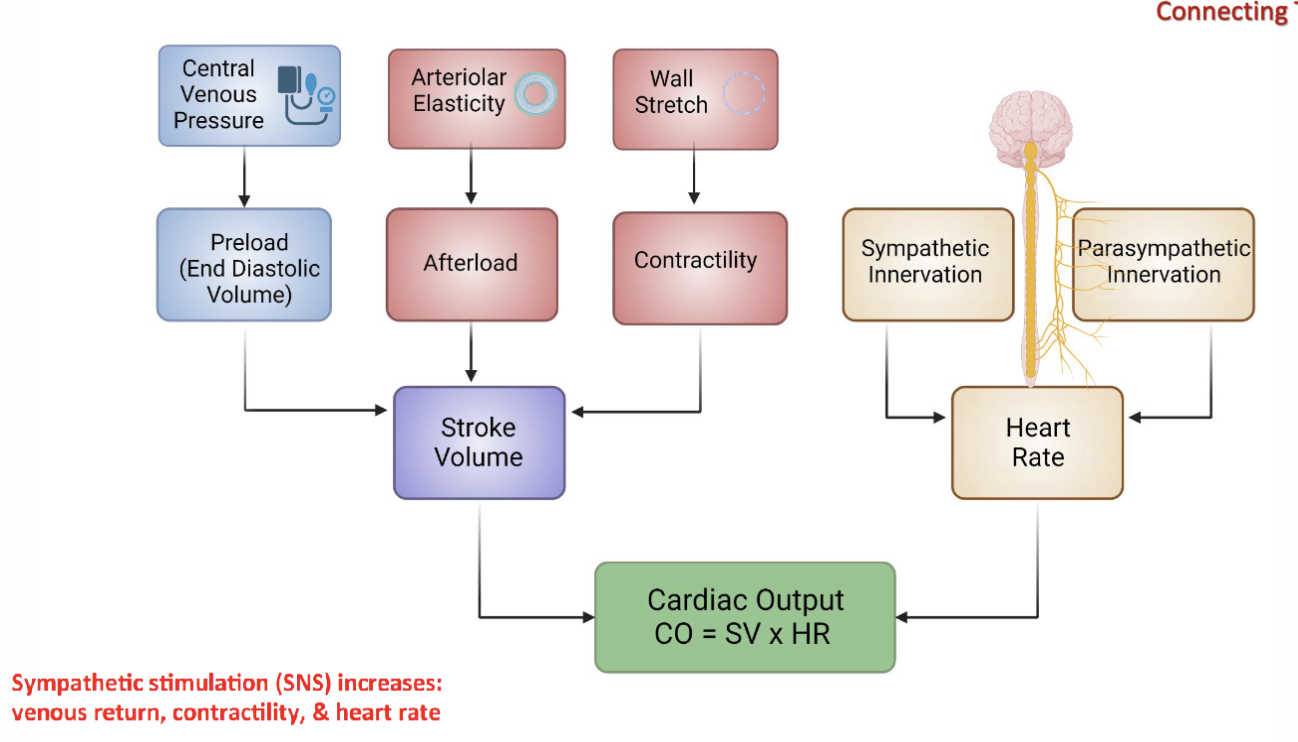
LEC 7: Explain the regulation of heart rate by autonomic nervous system
sympathetic NS: positive chronotropic effect → inc HR via SA node; positive inotropic effect by increasing intracellular Ca2+; positive dromotropic effect → inc AV conduction velocity (via beta1 adrenergic receptors)
parasympathetic NS: vagus nerve directly innervates SA node and dec HR; inhibits AV node conduction velocity w/ little effect on myocardial contractility
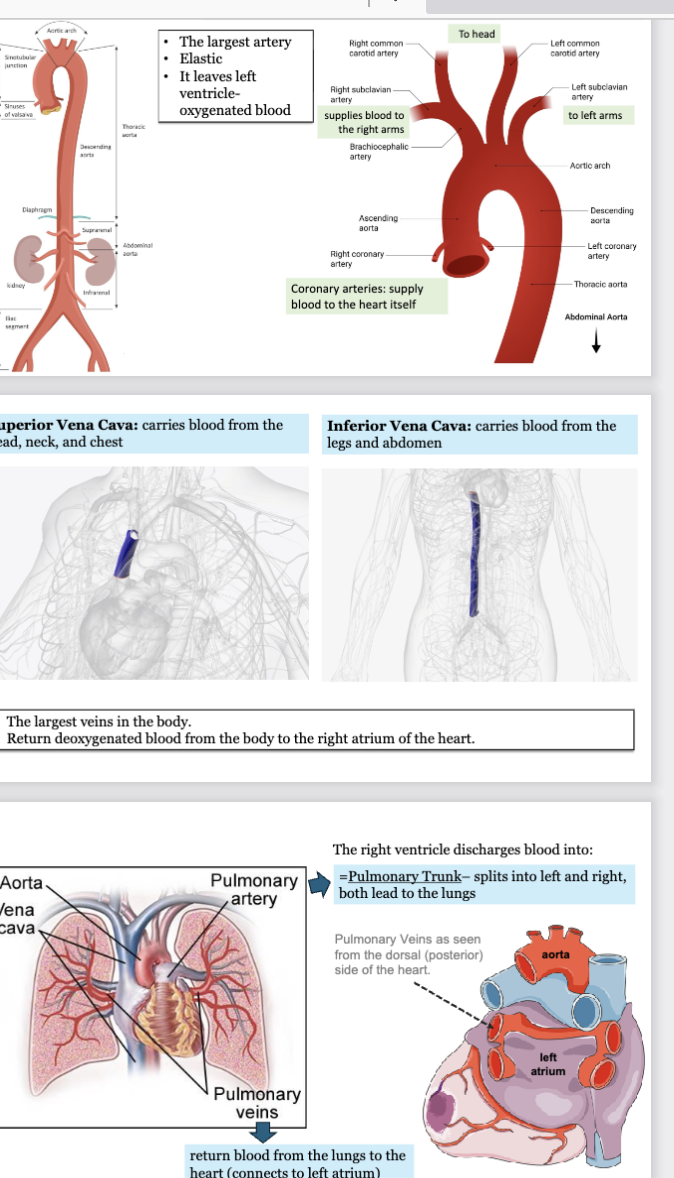
LEC 8: Identify the major blood vessels entering and leaving the heart
aorta: largest artery, most elastic, leaves left ventricle-oxygenated blood
ascending aorta: right and left coronary arteries supply blood to the heart itself
aortic arch: brachiocephalic artery emerges
right subclavian artery supplies blood to right arms
left subclavian artery supplies blood to right arms
right and left common carotid artery supplies blood to the head
—
vena cavae: largest veins in body, return deoxygenated blood from body to right atrium of heart
superior vena cava: carries blood from head, neck, and chest
inferior vena cava: carries blood from legs and abdomen
—
right ventricle discharges blood into → pulmonary trunk - splits into left and right and both lead to lungs
pulmonary veins return blood from lungs to heart (connects to left atrium)
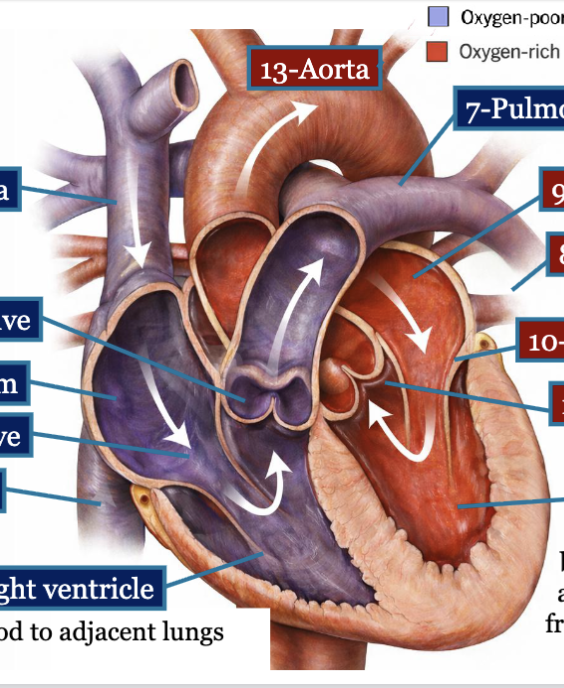
LEC 8: Trace the path of blood through the right and left sides of the heart, including its passage through the heart valves, and indicate whether the blood is oxygen-rich or oxygen poor
blood flow within heart is unidirectional
1-superior vena cava = oxygen poor
2-inferior vena cava = oxygen poor
3-right atrium = oxygen poor
4-tricuspid valve = oxygen poor
5-right ventricle = oxygen poor, thinner wall; sends blood to adj lungs (pulmonary circuit)
6-pulmonary valve = oxygen poor
7-pulmonary arteries = oxygen poor
8-pulmonary veins = oxygen rich
9-left atrium = oxygen rich
10-mitral valve = oxygen rich
11-left ventricle = oxygen rich, blood enters and leaves the ventricles at base → ventricles must contract from bottom (apex) up to expel blood from base
12-aortic valve = oxygen rich
13-aorta = oxygen rich
—
force propelling the blood: pressure gradient, created primarily by the contraction and relaxation of the heart muscle
p1 left ventricle → p2 aorta
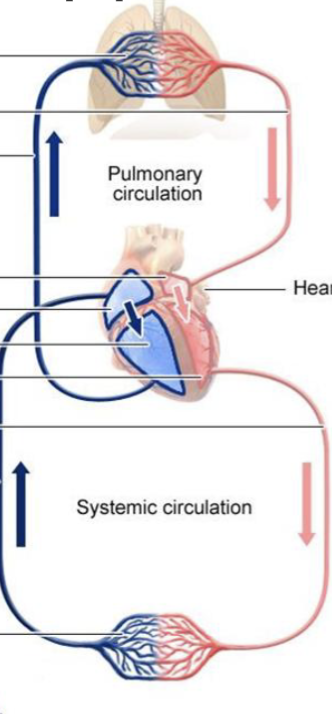
LEC 8: Explain how the heart is a double pump and why this is significant
the heart consists of 2 separate pumps:
pulmonary circulation - pumps blood thru lungs, where blood picks up oxygen and dumps CO2, and then blood travels back
systemic circulation - pumps blood thru body’s tissues, supplying them w/ oxygen and nutrients and removing CO2
—
left side of heart has thicker muscular wall (must generate much force)
LEC 8: Define end diastolic volume (EDV) and end systolic volume (ESV), and calculate stroke volume (SV) given values for EDV and ESV
end diastolic volume (EDV): total volume of blood in ventricle right at the end of diastole, avg M 160ml, avg F 132ml
end systolic volume (ESV): remaining blood in the ventricle after contraction (systole), avg M 54ml, avg F 44ml
stroke volume (SV): volume of blood pumped out (ejected) of ventricle per contraction or beat (systole), avg 50-100 ml
SV = EDV-ESV
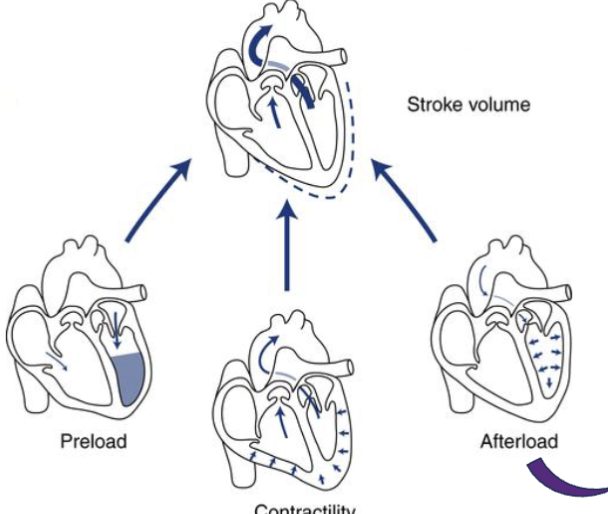
LEC 8: Describe the 3 primary factors that influence stroke volume (SV): preload, afterload, and contractility
preload: the degree of myocardial stretch at the end of diastole, directly proportional to EDV (described by Frank-Starling Law),
affecting factors: venous return and rate of filling after diastolic phase
afterload: the pressure against which the ventricle must contract to eject blood
affecting factors: systemic vascular resistance (SVR) and pulmonary vascular resistance (PVR)
vascular resistance: force that opposes flow of blood thru circulatory system
contractility: intrinsic strength of myocardial contraction (force with which ventricular ejection occurs)
affecting factor: autonomic innervation
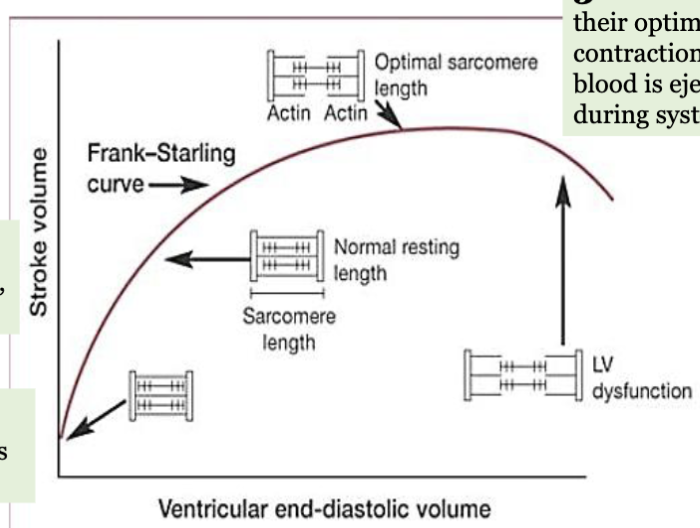
LEC 8: State the Frank-Starling Law of the heart
Frank-Starling Law: highlights intrinsic ability of the heart to adjust the force of its contraction in response to changes in ventricular filling (EDV)
1-when venous return inc, more blood fills heart during diastole
2-this inc volume stretches ventricular walls, lengthening sarcomeres
3-as sarcomeres approach optimal length, force of contraction inc → greater volume of blood ejected from heart during systole (SV)
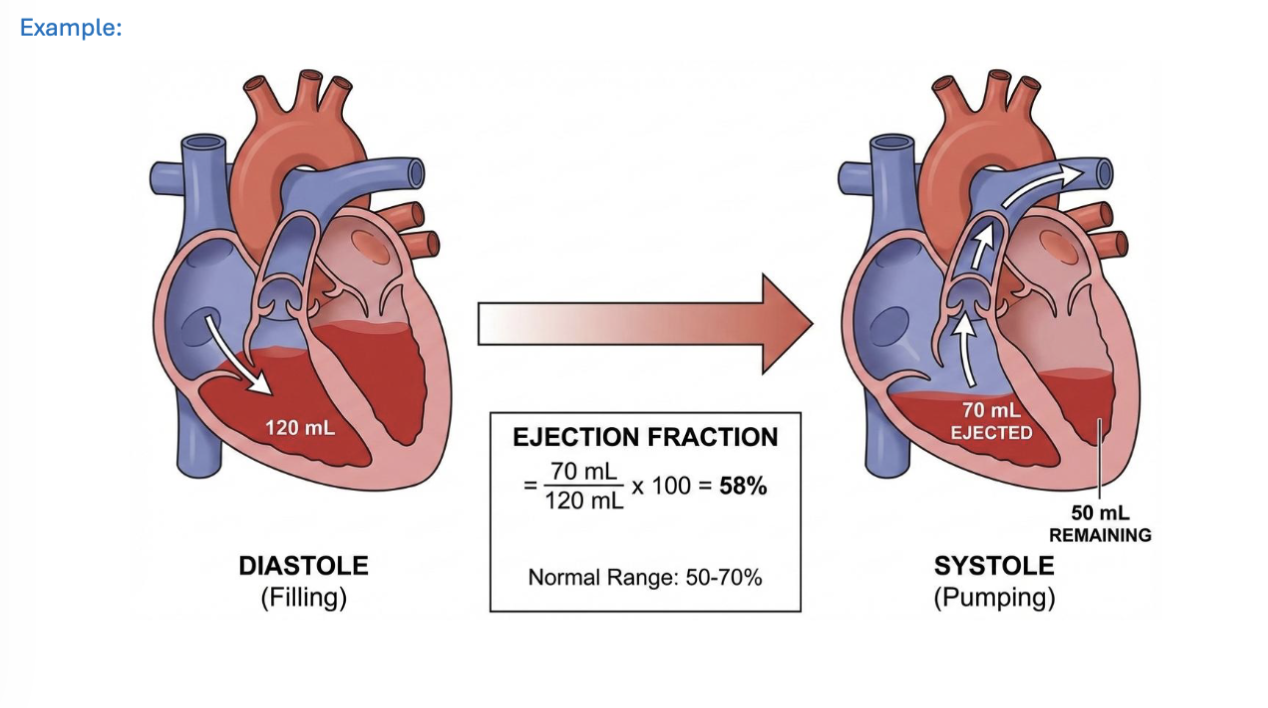
LEC 8: Explain ejection fraction (EF)
ejection fraction (EF): the % of blood pumped out of the ventricles at every contraction- describes the efficiency of heart
EF normalizes SV for heart size by expressing it as % of EDV
avg EF is 50-70%
EF(%) = SV/EDV * 100
SV = EDV-ESV
—
heart failure (HF): heart’s inability to pump blood effectively to meet body needs
EF is used to classify HF into categories:
HF with reduced ejection fraction (HFrEF) = impaired contractile function
HF with preserved ejection fraction (HFpEF)
LEC 8: Define cardiac output (CO). Predict how heart rate (HR) and/or SV changes will affect CO
cardiac output (CO): volume of blood pumped out of the ventricles in ONE MINUTE
normal range: 5-6 L/min
SV: volume of blood pumped out of left ventricle in single heartbeat
normal range: 50-100 mL
CO = SV * HR
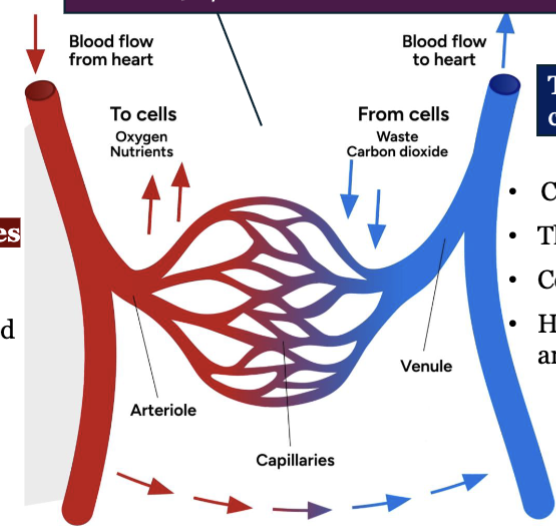
LEC 9: Define the terms artery, capillary, and vein
artery: strong elastic vessels which carry blood moving away from the heart, artery regulates blood flow to an organ
smallest ones: arterioles - connect to capillaries, arterioles regulate blood within organs
capillary: allow exchange of materials (oxygen nutrients) between blood and tissues
vein: thinner, less muscular vessels carrying blood toward the heart
capacitance vessels (hold high volume blood)
thin-walled and flaccid
collapse when empty, expand easily
have steady blood flow (unlike pulses in arteries)
small veins merge to form larger and larger one as they approach heart
types of veins: postcapillary venules, muscular venules, medium veins, large veins
LEC 9: List the three tunics associated with most blood vessels and describe the composition of each tunic
outermost-
tunica externa → adventitia
tunica media → [external elastic lamella (veins absent) > thick smooth muscle]
tunica intima → [internal elastic lamella (veins thin/absent) > basement membrane > endothelium]
→ lumen
innermost-
![<p>outermost-</p><p>tunica externa → adventitia</p><p>tunica media → [external elastic lamella (veins absent) > thick smooth muscle]</p><p>tunica intima → [internal elastic lamella (veins thin/absent) > basement membrane > endothelium]</p><p>→ lumen</p><p>innermost-</p>](https://assets.knowt.com/user-attachments/51a62c5a-fb52-4b71-9c55-9a7b6314d992.png)
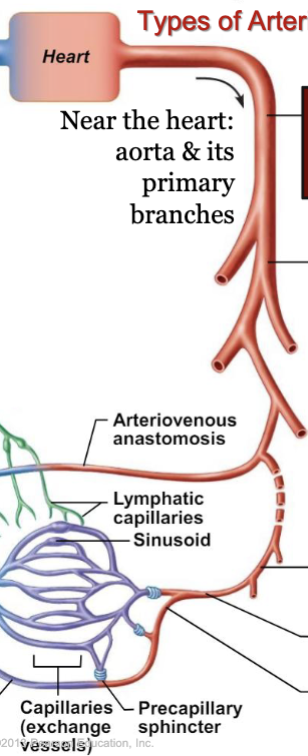
LEC 9: Indicate the function of specific types of arteries and arterioles
types of arteries
near the heart: aorta and its primary branches:
conducting (elastic or large) arteries: conduct blood away from heart, inc elastin: expand during systole and recoil during diastole which lessens fluctuations in BP
distributing (muscular or medium) arteries: distribute blood to body organs and tissues, thickest tunica media of all blood vessels
resistance (small) arteries: resistance vessels offer greatest resistance to blood flow due to small diameter, control amount of blood to various organs
smallest resistance arteries are the arterioles which lead directly into capillary beds, regulate flow by Vd/Vc
types of arterioles
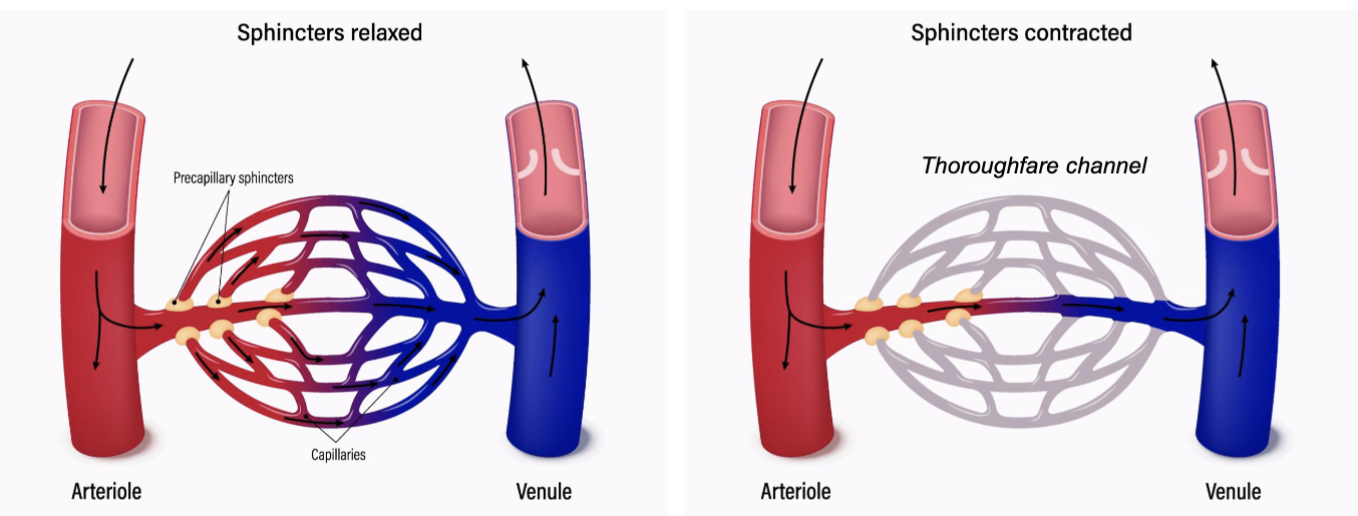
metarioles: link arterioles to capillaries, muscle cells form precapillary sphincter about entrance to capillary
LEC 9: Define capillary bed and its components
capillary bed: organized network of 10 to 100 capillaries that are supplied by single metarteriole
components:
arteriole on artery side…capillary bed... venules on vein side
capillary bed is site of exchange between blood and surrounding tissues
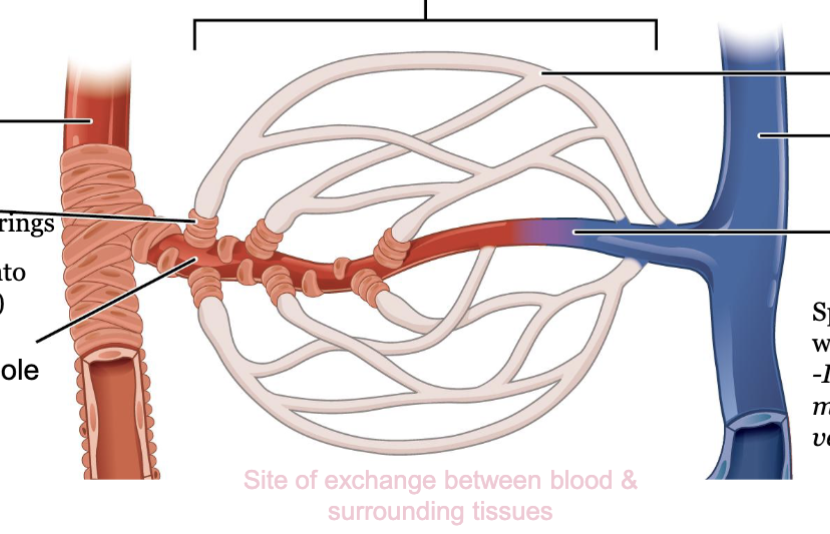
LEC 9: Explain the role of precapillary sphincter in autoregulation
precapillary sphincters: control blood flow into individual capillaries
when sphincters RELAXED/OPEN: blood flows through capillaries
when sphincters CONTRACTED/CLOSED: blood flows through thoroughfare channel, bypassing capillaries
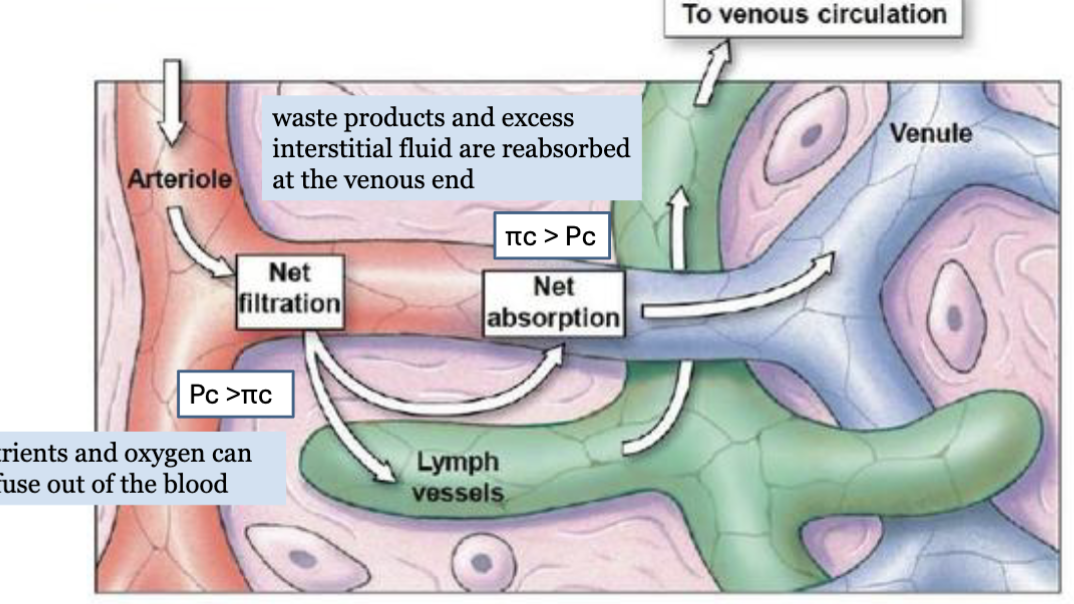
LEC 9: Describe the forces that create capillary filtration and reabsorption (Starling Forces)
Starling Forces → 4 forces
capillary hydrostatic pressure (Pc) → pushes fluid OUT of capillary → filtration
interstitial fluid pressure (Pi) → pushes fluid INTO capillary → reabsorption
capillary oncotic pressure (πc) → proteins pull water INTO capillary → reabsorption
interstitial oncotic pressure (πi) → proteins pull water OUT of capillary → filtration
net filtration pressure (NFP) = (Pc + πi) - (Pi + πc)
positive NFP → filtration
negative NFP → reabsorption
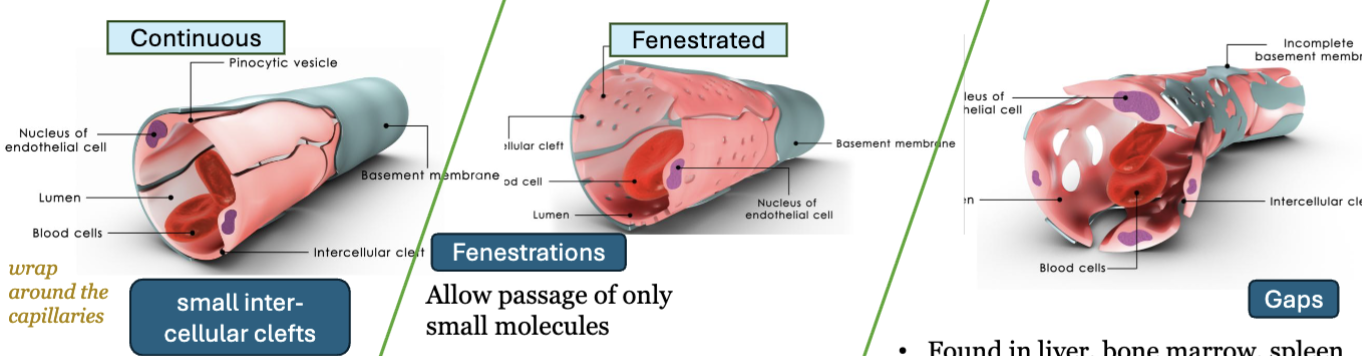
LEC 9: List types of capillaries, state where in the body each type is located, and correlate their anatomical structure with their functions
continuous capillaries
structure: tight junctions, small intercellular clefts
location: most tissues and organs
function: allows small molecules only
fenestrated capillaries
structure: fenestrations/pores in endothelial cells
location: kidneys, small intestine, choroid plexus
function: rapid absorption and filtration **HINT like holes on sports bra
sinusoidal capillaries
structure: large gaps, incomplete basement membrane
location: liver, bone marrow, spleen
function: allow proteins and blood cells pass
LEC 9: Indicate the factors aiding venous return
venous return = volume of blood flow returning to heart from veins
pressure gradient (veins → heart) - blood flow HIGH PRESSURE vein to LOW PRESSURE heart, venous blood TO heart
thoracic (respiratory) pump - inhalation: diaphragm contract and move down, chest pressure NEGATIVE, vacuum effect pull blood TOWARD heart
venous valves and muscle pump - veins have one-way valves → prevent backflow
LEC 9: Indicate variations in the circulatory pathways
simplest circulation pathway
heart → arteries → arterioles → capillaries → venules → veins → heart
portal system
blood flows thru 2 capillary beds in a row before returning to heart (hepatic portal system, hypothalamus-pituitary portal system)
anastomosis
connection where two blood vessels merge
arteriovenous anastomosis (shunt) → bypass capillaries
arterial anastomoses → artery to artery connection
venous anastomoses → vein to vein connection
fetal circulation: deliver most oxygenated blood quickly to brain and heart
oxygenated blood come from placenta → umbilical vein
3 fetal shunts
ductus venosus → bypass liver
foramen ovale → RA to LA
ductus arteriosus → pulmonary artery to aorta
LEC 9: Define blood flow, blood pressure, and peripheral resistance
blood flow: volume of blood moving thru vessels, an organ, or whole body per unit time, mL/min, total blood flow = CO at rest (5-25 L/min)
perfusion: blood flow per unit mass or volume of tissue, mL/min/g
blood pressure: force blood exerts on vessel walls, systolic/diastolic pressure
peripheral resistance (SVR/TPR): resistance to blood flow created by blood vessels
BP = Blood Flow * Resistance
LEC 9: State and interpret the equation that relates fluid flow to pressure and resistance
equation: Q = ΔP/R
Q = blood flow
ΔP = pressure gradient (P1-P2), greater ΔP greater blood flow
R = vascular resistance, friction
flow inc when pressure difference inc
flow dec when resistance inc
LEC 9: Analyze 3 factors that affect vascular resistance (R)
Poiseuille’s Law:
R = 8ηl/πr4
η = viscosity, l = vessel length, r = vessel radius
blood viscosity
determined mainly by hematocrit (RBC volume)
higher viscosity → greater resistance
vessel length
longer vessel → greater resistance
vessel radius (MOST IMPORTANT)
resistance ∝ 1/r4
small dec in radius → large inc in resistance
LEC 9: Indicate the intrinsic (local) and extrinsic (humoral, neural) factors that affect peripheral resistance and blood flow to tissues
intrinsic (local) - autoregulation
factors within tissue or vessel that regulate local blood flow
myogenic response: vessel constrict/dilate due to changes in wall tension
metabolic control: low perfusion → waste products accumulate → vasodilation → inc blood flow
extrinsic
neural
control vascular tone and bp
a-adrenergic → vasoconstriction
b-adrenergic → vasodilation
humoral (blood borne)
vasoconstrictors: angiotensin ii, catecholamines, thromboxane, leukotrienes, endothelin
vasodilators: prostaglandins, kinins, nitric oxide
—trigger
peripheral resistance controlled by:
intrinsic: myogenic + metabolic autoreg
extrinsic:
neural: alpha constrict, beta dilate
humoral: hormones/chemicals constrict/dilate vessels
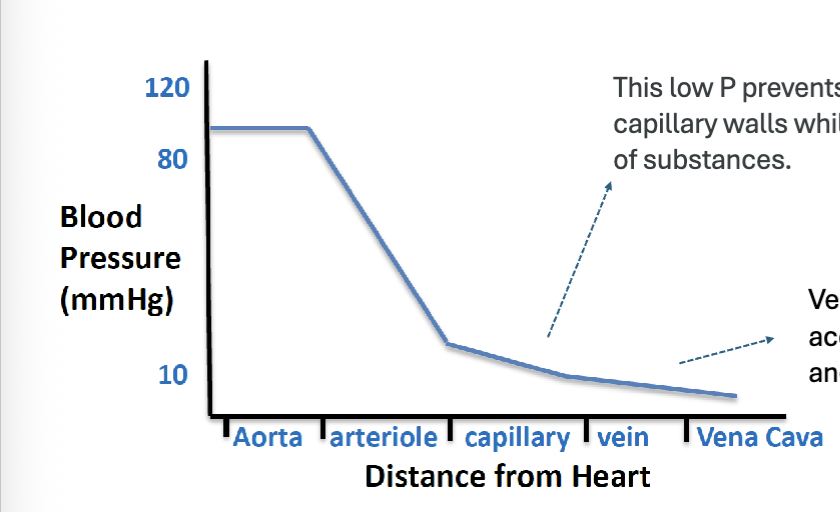
LEC 10: Using a graph of pressures within the systemic circuit, interpret the changes that occur in the arteries, capillaries, and veins
aora/arteries: have the highest pressure (~120mmHg), pressure is pulsatile due to heart contractions
arterioles: largest drop in pressure, major resistance vessels
capillaries: low pressure (~10-30mmHg), prevents damage to thin capillary walls, allow diffusion of gases and nutrients
veins: very low pressure, blood moves back to heart slowly
vena cava: lowest pressure (~0mmHg)
LEC 10: Given values for systolic and diastolic BP, calculate pulse pressure (PP) and mean arterial pressure (MAP)
pulse pressure (PP) = systolic BP (SP) - diastolic BP (DP)
SP: peak pressure during ventricular contraction
DP: lowest pressure during ventricular relaxation
mean arterial pressure (MAP) = DP + (1/3)(SP-DP)
MAP always closer to DP
represents average pressure in arteries during one cardiac cycle
MAP important bc it indicates pressure that perfuses organs
LEC 10: State the relationship between MAP, CO, and Total Peripheral Resistance (TPR)
MAP = CO * TPR
whenever CO dec, TPR inc to maintain MAP
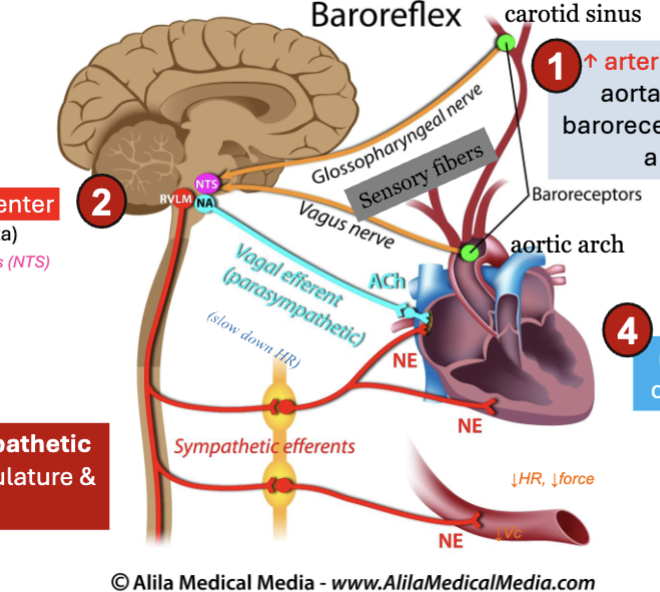
LEC 10: State the arterial sensory receptors and their functions
BARORECEPTOR (baroreflex)
location: carotid sinus, aortic arch
function: stretch receptors that detect BP, send signals to brainstem to regulate BP
CHEMORECEPTOR (chemoreflex)
location: carotid bodies, aortic bodies
function: detect changes in O2, CO2, and pH, send signals to brainstem respiratory centers, adjust respiration and vascular tone
LEC 10: Explain the steps of the baroreceptor reflex and describe how this reflex maintains BP homeostasis when BP changes
rapid, short-term regulation of BP via negative feedback
steps when BP increases:
INC of BP stretches arteries
baroreceptors in carotid sinus + aortic arch detect stretch
fire more AP
signals sent to cardiovascular center
medulla oblongata (nucleus tractus solitarius - NTS)
sympathetic activity DEC
DEC vasoconstriction
DEC heart activity
parasympathetic (vagal) activity INC
DEC heart rate
DEC contractility
BP dec back toward normal
LEC 10: State the functions of the blood
transport
delivers O2, nutrients, hormones
removes CO2 and metabolic wastes (urea)
regulation
maintains pH balance
maintains fluid balance
thermoregulation (heat distribution)
protection
immune defense (WBCs and antibodies)
hemostasis (stop bleeding)
LEC 10: Describe the overall composition of plasma, including the major types of plasma proteins and cells
blood composition: 55% plasma and 45% formed elements, adult 5L
plasma composition: 90% water, 7% proteins, 1-2% other solutes like electrolytes, nutrients, hormones, wastes
major plasma proteins: most synthesized in liver
albumin (60%) → maintains osmotic pressure
globulins (35%) → transport and immune functions
alpha: transport lipids, metals, hormones
beta: lipid transport (ex. LDL)
gamma: immunoglobulins (antibodies), produced by immune cells
fibrinogen (4%) → blood clotting/coagulation
other <1%: hormone transport proteins: SHBG, CBG, TBG
formed elements (3 types)
erythrocytes (RBCs)
45% of blood
transport oxygen
leukocytes (WBCs)
immune defense
types: neutrophils, lymphocytes, monocytes, eosinophils, basophils
platelets
blood clotting
all arise from hematopoietic stem cells in red bone marrow
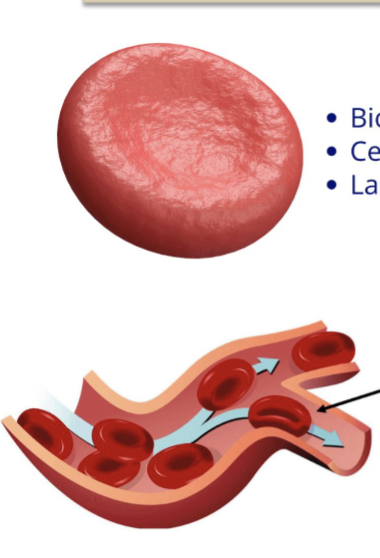
LEC 10: Indicate the morphological features of erythrocytes and their main function
morphological features:
biconcave disc shape
flexible membrane
no nucleus
no organelles
shape purpose: allow RBCs to squeeze thru narrow capillaries
main function:
transport O2 from lungs → tissues… CARRY
transport CO2 from tissues → lungs… REMOVE
LEC 10: Discuss the structure of hemoglobin
globular metalloprotein
quaternary structure (4 subunits)
2 alpha chains
2 beta chains
heme group
each subunit contains heme group
heme contains Fe2+ (ferrous ion) inside porphyrin ring
oxygen binding
each Fe2+ binds 1 O2 molecule
1 hemoglobin can carry 4 O2 molecules
fetal hemoglobin
beta chains replaced by gamma chain
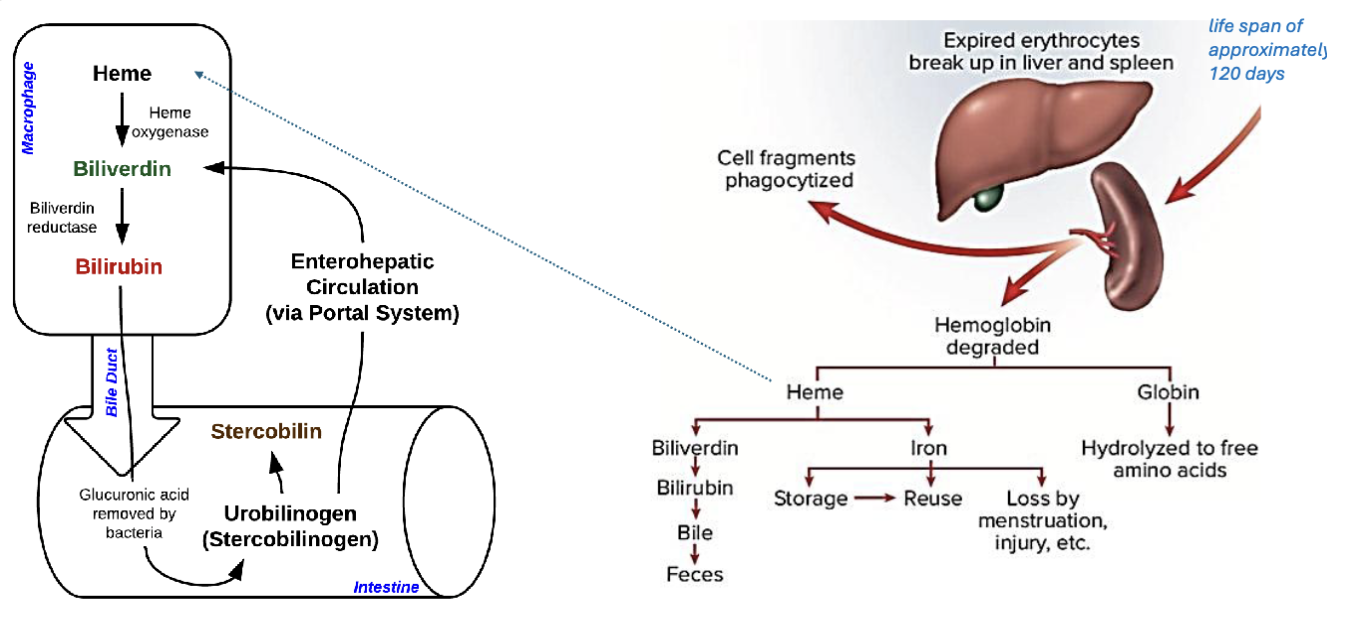
LEC 10: Discuss the breakdown products of hemoglobin
Hemoglobin → globin + heme
globin → amino acids
iron → reused
porphyrin → bilirubin → bile → stercobilin (feces)
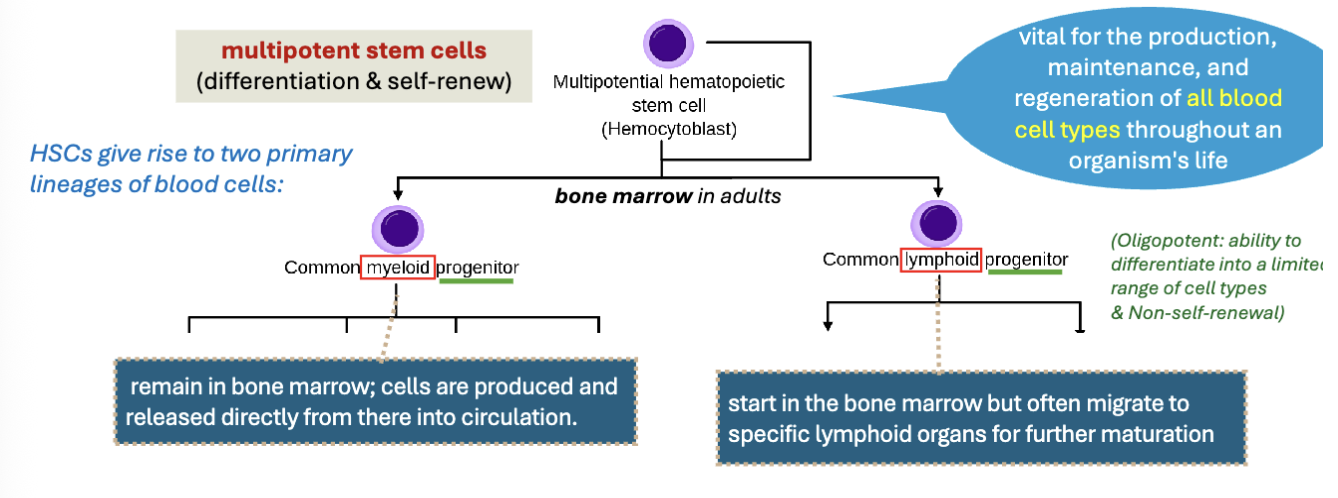
LEC 10: State the significance of the hematopoietic stem cell (HSC or hemocytoblast)
hematopoietic stem cells (HSCs)
multipotent stem cells in bone marrow
produce all blood cells types
2 main lineages
myeloid → RBCs, platelets, most WBCs
lymphoid → lymphocytes
LEC 10: Explain the basic process of erythropoiesis and define hematocrit
erythropoiesis: production of RBCs in red bone marrow
stimulated by: erythropoietin (EPO)
requires: iron, vitamin B12, folic acid, globin protein
stages of RBC development
proerythroblast → erythroblast stages → nucleus ejected → reticulocyte → mature erythrocyte (RBC)
hemoglobin synthesis INC during maturation
hematocrit (HCT/Ht): percentage of blood volume made up of RBCs
LEC 10: Describe the process of leukopoiesis and its key regulatory factors (CSFs and ILs)
Leukopoiesis = WBC formation in bone marrow
lineages:
myeloid → granulocytes + monocytes
lymphoid → T cells, B cells, NK cells
regulated by: colony-stimulating factors CSFs (G-CSF, GM-CSF, M-CSF), interleukins (IL-7, 15)
CSF myeloid lineage
IL/lymphocyte by cytokines
LEC 10: Indicate the types of leukocytes and their main functions. Classify each type as granulocyte or agranulocyte
granulocytes (granular cytoplasm)
neutrophils → phagocytosis
eosinophils → parasites
basophils → histamine
agranulocytes (no visible granules)
monocytes → macrophages
lymphocytes → T cells and B cells
NK cells → kill infected/cancer cells
innate immune system - first line of defense, recognize PAMPs using PRRs
adaptive immune system - highly specific, TCRs and BCRs → immunological memory
LEC 10: Describe platelets (thrombocytes), including their origin (how they form)
platelets (thrombocytes): small anucleate/no nucleus cell fragments, derived from megakaryocytes in bone marrow
formation
hematopoietic stem cell → myeloid progenitor → megakaryoblast → megakaryocyte → platelets
regulated by THROMBOPOIETIN (TPO) from liver + kidneys
main role: essential for hemostasis (clotting)
LEC 10: Describe the functions of platelets and identify and explain three main types of secretory organelles they contain
platelet function
hemostasis
thrombosis
platelet adhesion, activation, and clot formation
3 types of platelet granules
alpha-granules (most abundant) → clotting proteins (eg. vWF)
delta-granules (dense bodies) → activation (eg. ADP, ATP, Ca2+, serotonin)
lysosomes → proteolytic enzymes
LEC 11: Describe the role of platelets in hemostasis and the steps involved in the formation of the platelet plug
hemostasis: process that stops bleeding after blood vessel injury
steps of hemostasis
vascular spasm → vasoconstriction reduces blood flow and loss
primary hemostasis (platelet plug formation) (adhesion → activation → aggregation)
adhesion → platelets bind to exposed collagen, vWF help
activation → inc intracellular Ca2+, ADP and TXA2
aggregation → GP Ilb/Ila receptors bind fibrinogen, cross link
secondary hemostasis (coagulation cascade)
prothrombin → thrombin
fibrinogen → fibrin
fibrin mesh stabilizes platelet plug
requires Ca and K
LEC 11: Differentiate among the intrinsic, extrinsic, and common pathways of the coagulation cascade
coagulation cascade purpose: stabilize platelet plug w/ fibrin, clotting factors mostly produced in liver, serine proteases most factors
intrinsic pathway (contact pathway)
trigger: blood contacts exposed collagen/vessel damage
factors involved: 12 → 11 → 9 → 8 → 10, leads to activation of factor x
INTRINSIC = 12 11 9 8 10, FACTOR X
extrinsic pathway (tissue injury pathway)
trigger: tissue factor (factor III) released from damaged tissue
factors involved: 7 → 10
EXTRINSIC = 7 10
common path way (final clot formation)
factor x → Xa → prothrombin (ii) → thrombin (ila) → fibrinogen → fibrin → factor xiii cross link fibrin → stable clot
Ca (factor IV) → required for clotting rxn
K → needed to synthesize functional clotting factors
factor V → cofactor in prothrombinase complex
platelet granule molecules (help clot)
delta: ADP activate platelets, Ca2+ required for coagulation
alpha: vWF platelet adhesion to collagen, fibrinogen platelet aggregation, factor V clotting
LEC 11: Explain clot retraction
clot retraction: platelets contract and pull fibrin threads tgt, tighten clot
results: clot become stronger and smaller, serum squeezed out, edges of damaged vessel pulled tgt, blood flow partially restored
purpose: stabilize clot and help repair blood vessel
LEC 11: Discuss the process of fibrinolysis, including roles of plasminogen, tissue plasminogen activator, and plasmin
fibrinolysis: process that breaks down clot after healing begins
process of fibrinolysis:
endothelial cells release tPA (tissue plasminogen activator) → tPA converts plasminogen → plasmin → plasmin break down fibrin in clot → clot dissolves and normal blood flow returns
regulation: PAI-1 inhibit tPA, alpha2-antiplasmin inhibit plasmin preventing excessive clot breakdown
LEC 11: Explain the role of surface antigens on RBCs in determining blood groups
blood group determined by antigens on the surface of RBCs
2 main systems: ABO and Rh
if you lack antigen → you naturally have antibodies against it bc immune system is tolerant to self-antigens
A and B alleles are dominant, O allele is recessive
All RBCs have base structure H antigen. ABO gene make enzyme transferase that modifies H antigen
blood type → antigen on RBC → antibodies in plasma
A → A antigen → anti B
B → B antigen → anti A
AB → A and B antigens → none
O → none → anti A and anti B
Rh blood group: determined by Rh (D) antigen
LEC 11: Describe how the presence or absence of Rh antigen results in blood being classified as positive or negative
Rh blood type is determined by presence/absence of Rh (D) antigen on RBCs
type → meaning
Rh+ → RBCs have RhD protein antigen
Rh- → RBCs lack RhD protein antigen
LEC 11: Predict which blood types are compatible
you cannot receive RBCs with antigens your antibodies attack
universal donor: O-
universal recipient: AB+
ABO compatibility
blood type → can receive from
O → O
A → A, O
B → B, O
AB → A, B, AB, O
Rh rule: Rh+ can receive +/-, Rh- can only receive -
LEC 11: State the consequences of transfusing the incorrect ABO blood type
what happens: recipient antibodies bind donor RBC antigens, agglutination (RBC clump), hemolysis (RBC destruction)
consequences: clot block blood vessels, released hemoglobin damages kidneys, lead to kidney failure and severe transfusion rxn
LEC 11: Describe the development and clinical significance of anti-Rh antibodies
occurs when Rh- mom carries Rh+ fetus
first pregnancy: fetal Rh+ RBCs enter mom blood (usually during delivery), mother immune system recognize Rh antigen as foreign
maternal sensitization: mother product anti-Rh (anti-D) antibodies
subsequent Rh+ pregnancy: maternal anti-Rh IgG antibodies cross placenta
effect on fetus: antibodies destroy fetal RBCs → hemolytic disease of newborn (HDN)