Fluid and Electrolights
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
98 Terms
Fluid =
Water that contains dissolved and suspended such as glucose, mineral salts, and proteins
Fluid amount=
Volume
Fluid concentration=
Osmolality
degree of acidity =
pH
Intracellular-fluid inside the cells
2/3 of body water
plasma, trancellular fluids such as CSF, pleural,peritoneal, and synovial fluid
Extracellular fluid outside the cell
interstitial fluid b/w the cells
intravascular fluids inside vessels
Transcellular
Positive cations
Na+
K+
Ca 2+
Mg2+
Negative Anions
Cl-
HCO3-
Concentration
fluid containing of dissolved particles is more concentrated the same amount of fluid contains few particles
Osmolality
measure of the number of particles per Kilogram of water
some particles pass easily through cell membranes; others such as Na+ cannon cross easily
Tonicity
cannot cross cell
Isoronic-
Same tonicity
hypotonic:
Fluid more Dilute than blood
Hypertonic
fluid more concentrated than more blood
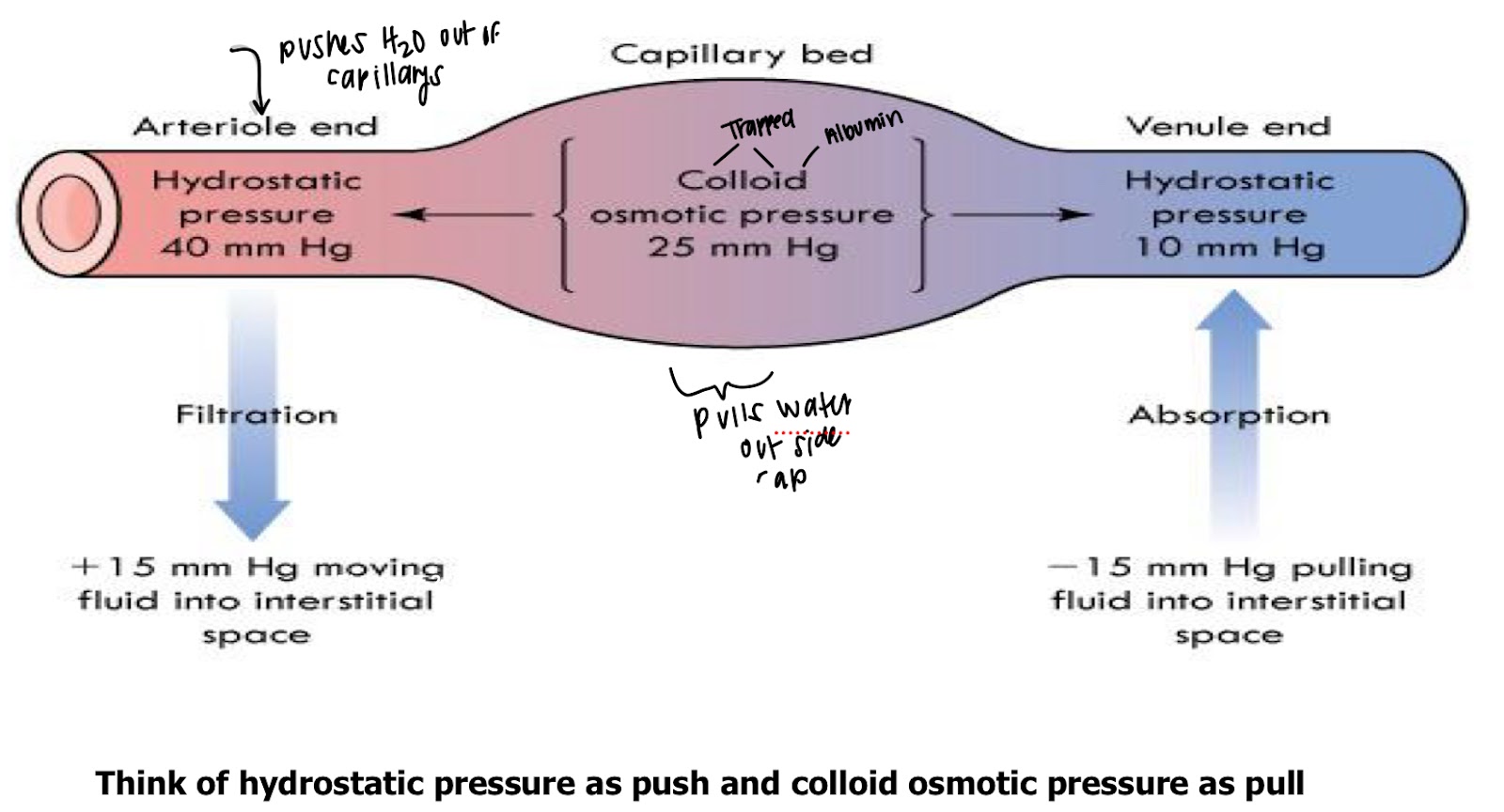
Filtration
Fluid moves into and out of capillaries
Active transport
Uses ATP to move electrolytes across cell membrane against concentration gradient (low to high concentration)
Diffusion
Passive movement of electrolytes or other particles down a concentration gradient (high to low concentration)
Osmosis
water moves through membrane separates fluid with different particle concentrations
Osmotic pressure
inward-pulling force by particles in fluid
Fluid intake
healthy adult 2300L
8-10 glasses per day 1920-2400 mL
80% food, 20% from food
fluid output
occurs in organs
skin
lungs
GI
kidneys
sensible loss
(visible) urine, feces, gastric drainage
insensible loss
(not visible) diffusion and evaporation through skin, lungs (water lossthrough skin/lungs)
Hypovolemia (ECV deficit)
output exceeds intake of sodium-containg fluid
sudden weight loss
postural hypotension
tachy
thready pulse +1
dry mucous membrane
poor skin turgor
dark yellow urine
Hypervolemia (ECV excess)
intake of sodium-containg isotonic fluid has exceeded fluid output
sudden weight gain
edema
DNV
crackles on auscultation
HyperNAremia
“water deficit”; hypertonic across cell membranes
serum Na+>145mEq/L (145mmol/L)
DEHYDRATION
Decrease LOC (confusion, lethargy, coma)
Thirst, dry mucous membrane
Seizures
HypoNatremia
“water excess”, hypotonic
intracelluar dehydration
Serum Na+ level <136mEq/L (136 mmol/L)
decrease LOC (confusion, lethargy, coma)
Seizures if develops rapidly or is very severe
A nurse is assessing a PT admitted w clinical dehydration. Which of the following findings would the nurse expected?
Dry Mucous membrane
Concentrated urine
Hypotension
confusion
HyperKalemia
potassium K 3,5-5.0 mEq/L
cause: Oliguria decrease K output , chronic Renal failure ESRD, DKA, use of potassium sparing diueretics
muscle weakness
Life Threatening Dysrhythmias
Cardiac Arrest
Foods: Fruits,potatoes,instant coffee,molasses Brazil nuts
HypoKalemia
cause: increase potassium output include diarrhea repeated vomiting, and use of potassium-wasting diuertics, glucosteroids therapy, Treatment for DKA
Muscle weakness
Resp muscle weakness
ECG-ST segment dep
Life Threating Dysrhythmias
Foods: Fruits,potatoes,instant coffee,molasses Brazil nuts
HyperCAlcemia
9.0-10.5 mg/dl
cause: increase calcium intake & absorption, shift of calcium and bone into the ECF, and decrease calcium output, some malignancies, prolonged
Food: diary products, canned fish w bones, broccoli ,oranges , requires vit D for best, absorption, undigested fat prevents absorption
HypoCAkcemia
cause: too much Ionized calcium to shift to the bound forms (pancreatitis) Chronic diarrhea, steatorrhea, laxative misuse
Food: diary products, canned fish w bones, broccoli ,oranges , requires vit D for best, absorption, undigested fat prevents absorption
HypoCAkcemia s/s
neuromuscular exitability
tetany
chvostek’s and Trousseau’s sign
muscle Twitching
Hyperactive reflexes
hyperCAlcemia
s/s
Anorexia, N/V
pathological fractures
decrease neuromuscular
excitability
decrease reflexes
lethargy, confusion
cardiac arrest if severe
HyperMAGnesemia
1.3-2.1 mEq/L
cause: ESRD, excessive use of magnesium contacting laxatives
Food: dark leafy vegetables, whole grains, undigestive fat prevents absorption
hypermagnesemia s/s
decrease neuromuscular excitability
lethargy
decrease DTRs
brady
severe-carduac Arrest, decrease RR
HypoMAGnesemia
casues: decrease mag intake and absorption, sift of plasma mag to its inactive bound form, and increase mag output, Alcoholism , malnutrition, chronic Diarrhea
HypoMAGnesemia
s/s
neuromuscular excitability
chovostek’s sign
hyperactive DTRs
tetany
cardiac dysrhythmias
acid production
cardbonic acid-excreated by lungs
metabolic acid-excrered by kidneys
Respiratory Acidosis
Alveolar Hypoventilation- the lung are unable to excrtet enough CO2
paCO2 rises, creating an excess of cardbonic acid in blood , which decreases pH
respiratory alkalosis
Alveolar hyperventilation lungs excrete too much cardbonic acid
paCO2 falls,creating a deficit of carbonic acid in the blood, which increases pH
Metabloic acidosis
occurs from an increase of metabolic acid or a decrease of base (HCO-3)
Metabolic Alkalosis
occurw from a direct increase of base (HCO-3) or a decrease of metabloic acid increase blood HCO3- by release
<7.35 = pH
acidosis
>7.35 = pH
alkalosis
PaCO2 >45mm Hg =
respiratory Acidosis
PaCO2 <35 mmHg=
respiratory alkalosis
HCO3 <21 mEq/L =
metabolic acidosis
Hco3 >28 mEq/L
metabolic alkalosis
Age: very young and old at risk
Very young: ECV deficit, osmolality imbalances, clinical dehydration
Very old: ECV excess or deficit, osmolality imbalances
Environment: excessively hot?, physical work, fluid replacements with salt?
intake: fluids, salt, foods rich in potassium, calcium, and
magnesium
Lifestyle: alcohol intake history
Medications: include over-the-counter (OTC) and herbal, in addition to
prescription medication
Skin and Mucous membranes (Tugor), Vital Signs
Daily weights
Best indicator of fluid status
Each kilogram (2.2 lb) of weight gained or lost overnight is equal to 1 L of
fluid retained or lost.
Weigh the patient at the same time each day with the same scale after a
patient voids Use same conditions
examples of patients w fluid, electrolytes and acid-base altertions
fluid imbalance
Dehydration
electrolyte imbalance
acid base imbalance
lack of knowledge of fluid regime
planning
goals and outcomes
setting priority's
teamwork and colab
implementation
teach pt and caregivers to recognize risk factors for dev imbalances and implement appropriate preventive measure
teach pt w chronic conditions about risk factors and sign of imalance, and to do if they occur
Fluid intake and output (I&O)
24-hour I&O: compare intake versus output
Intake includes all liquids eaten, drunk, or received through feeding tubes, IV
output = Urine, diarrhea, vomitus, gastric suction, wound drainage
Assessment
lab values
cbc
electrolytes
serum/urine osmolality
UA
ABG’s
Isotonic
0.9% saline (NRN)
Lactated ringers (LR)
5% Dextrose in water
Hypotonic
0.45% saline (1/2 NS)
0.225% saline (1/4 NS)
0.33% saline (1/3 NS)
Hypertonic
3% saline
5% saline
10% Dextrose in water (D10 W)
5% Dextrose in 0.9%
5% dex in 0.45% saline
5% dex in lactated ringers
Inserting of the intravenous line
Guage
length of treatment
type of fluid
a peripheral VAD is called an over-the-needle cath; consists of a small plastic tube or cath threaded over a sharp stylet (needle)
butterfly needle
IV adm
1. Infusion of large volumes of IV fluid containers
that contain medications mixed, labeled, and
dispensed by pharmacy
2. Injection of a bolus or small volume of medication
through an existing IV infusion line or intermittent
venous access (heparin or saline lock)
3. “Piggyback” infusion of a solution containing the
prescribed medication and a small volume of IV
fluid through an existing IV line
IV Bolus
Introduces a concentrated dose of medication
directly into the systemic circulation.
Advantageous when the amount of fluid that a patient can take is restricted.
The most dangerous method for medication administration because there is no time to correct errors.
Confirm placement of the IV line in a healthy site.
Determine the rate of administration by the amount of medication that can be given each minute.
volume controlled infusions
small amounts (50-100mL) compatible fluids
adm sets, piggy back stem, & syringe pumps
IVPB-IV piggy back
small (25 to 250 mL) IV bag or bottle short line that connects to the upper Y-port of a primary line or to an intermittent venous access
regulating the infusion rate (IV pump)
Avoid uncontrolled flow into a patient, Use Electronic infusion devices (EIDs), IV pumps
Calculate the flow rate (mL/hr) at prescribed time frame.
Maintaining the system
Keeping the system sterile and intact;
Changing IV fluid containers, tubing, and contaminated site dressings;
Helping a patient with self-care activities so as not to disrupt the system;
Monitoring for complications of IV therapy.
Blood transfusion
Autologous transfusion (autotransfusion) is the collection and reinfusion of a patient’s own blood.
blood transfusion s/s
Anemia
Blood loss
Increasing circulating blood volume after surgery,trauma, or hemorrhag
Deficiency in blood component
Clotting factors, platelets, albumin
Hemoglobulin < 7 or 8 with active bleed/symptomatic
Group A
Has only the A antigens on the red cells and (B antibody in the plasma)
Group B
Has only the B antigen on red cells (A antibody in plasma)
Group AB
Has both A & B antigens on red cells (neither A nor B antibody in plasma)
Group O
Has neither a Norby antigens on red cells, but (both A and B Antibodies are in the plasma)
Transfusion blood products
Two RNs verify
Stay with patient for the first 15 minutes
VS Q 15 times 2, then 30 min, then post-infection
Mild allergic allergy to blood
Flushing, itching, urticaria (hives)
Sepsis bacterial contamination of blood
Rapid onset of chills, high fever, severe hypotension, and circulatory
shock
May occur: Vomiting, diarrhea, sudden oliguria (acute kidney
injury), disseminated intravascular coagulation (DIC)
Febrile non-hemolytic sensitivity to white blood cells, plasma protein
Sudden shaking chills (rigors), fever (rise in temperature 0.5c 1F
Headache, flushing, anxiety, muscle pain
Hemolytic reaction right blood cell breakdown due to incompatible blood
Chills, fever, low back pain, flushing tacky tacky Peia hypotension hemoglobinuria sudden oliguria (acute kidney injury) circulatory, shock, cardiac arrest, and death
Circulatory overload too much or two rapid infusion
Dyspnea, cough, crackles or rails lobes of lungs
DNV went upright
Blood transfusion reactions
Stop transfusion if suspected reaction
Replaced with saline infusion
Notify HCP
IF HEMOLYTIC-send Tubing, blood, sample of blood and urine from PT to lab
Prepare to call a code/ CPR/ MEDs
A nurse is assessing a patient with hyponatremia. Which of the following clinical manifestations should the nurse expect?
Confusion and seizures
A nurse is reviewing a patient’s lab results and notes a potassium level of 5.8 mEq/L. Which of the following interventions should the nurse anticipate?
Prepare the patient for sodium polystyrene sulfonate ( kayexalate) adm
A patient is admitted with severe dehydration. Which of the following findings should the nurse expect?
Hypotension
A nurse is caring for a patient with metabolic acidosis. Which of the following conditions is a potential cause of this imbalance?
Diabetic ketoacidosis
A nurse is monitoring a patient receiving IV magnesium sulfate for hypomagnesemia. Which of the following findings indicates magnesium toxicity?
Positive Trousseau’s sign
The nurse is assessing a patient with hypocalemia. Which of the following findings should the nurse expect
Distended neck veins
A patient with a history of heart failure is admitted with fluid volume overload. Which of the following findings should the nurse expect?
Respiratory depression
A nurse is reviewing a patient's arterial blood gas (ABG) results: pH 7.30, PaCO₂ 50 mmHg, HCO₃ 24 mEq/L. The nurse recognizes these findings indicate which acid-base imbalance?
Respiratory acidosis
A nurse is providing care for a patient with hypernatremia due to dehydration. Which of the following interventions should the nurse include in the plan of care?
Encourage oral fluids and adm hypotonic IV fluids
A patient with heart failure has a sodium level of 128 mEq/L. Which of the following factors may have contributed to this imbalance
Excessive Diuretic use
1. An IV fluid is infusing more slowly than ordered. The infusion pump is set correctly. Which factors could cause this slowing? (Select all that apply.)
1. Infiltration at VAD site
2. Patient lying on tubing
Tubing kinked in bedrails
The nurse assesses pain and redness at a VAD site. Which action is taken first?
Discontinue the IV infusion
When delegating I&O measurement to assistive personnel, the nurse instructs them to record what information for ice chips?
One-half of the volume
What assessments does a nurse make before hanging an IV fluid that contains potassium? (Select all that apply.)
Urine output
Serum potassium laboratory value in EHR
The health care provider’s order is 500 mL 0.9% NaCl intravenously over 4 hours. Which rate does the nurse program into the infusion pump?
125 mL/hr
Which of the following steps are necessary when inserting a short-peripheral IV? (Select all that apply.)
1. Apply tourniquet to arm 10 to 15 cm (4–6 inches) above theintended insertion site.
2. Cleanse skin using an approved antiseptic agent such as alcohol-based 2% chlorhexidine and allow to dry thoroughly.
4. Use the smallest-gauge, shortest catheter available and insert with the bevel up at a 10- to 15-degree angle.
5. Observe for blood in the flashback chamber of the catheter
and advance the catheter off the needle into the vein.
Place the following steps for discontinuing IV access in the correct order:
Carefully check the healthcare providers order
Used to identifiers to ensure correct patient
Explain procedure to patient
Perform hand hygiene and apply gloves
Stop the infusion and clamp the tubing
Remove IV site dressing in tape
Clean the site with withdraw the catheter and apply pressure
A patient has hypokalemia with stable cardiac function. What are the priority nursing interventions? (Select all that apply.)
Fall prevention intervention
Monitor for constipation
Which assessment does the nurse use as a clinical marker of vascular volume in a patient at high risk of ECV deficit?
Fullness of neck veins when supine