Cardiovascular System: Blood
List the main functions of the Circulatory system:
Distribution - Regulation - Protection
Body Temperature
Oxygen
Electrolytes (H+ Ions)
Takes away CO2
Regulation action potentials and hormones
Water protection (barrier)
Describe the basic characteristics of the blood:
More dense than water
pH= 7.35 - 7.45
Volume
5-6 liters in males & 4-5 liters in females
Temperature - 100.4 degrees
(Add pressure to help blood flow to a certain place)
Constricting
List the three formed elements:
Cell and cell fragments
Erythrocytes = RBC’s (99% of formed elements)
Carry O2 and CO2
More abundant and have no nuclei.
Leukocytes = WBC’s
Fight diseases
Have nuclei and can differ in size/types
Platelets (Cell Fragments)
Define hematocrit (or packed cell volume) and describe its importance:
Measures the proportion of red blood cells in the blood. Red blood cells carry oxygen throughout the body. Having too few or too many of them can be a sign of certain diseases. The hematocrit test is a simple blood test. It is sometimes referred to as a packed-cell volume test.
Blood tends to clot because:
Moving Slower
Rough Surfaced
Thicker Blood
Tends to happen in athletes that take RBC boosters, boosting the RBC count % to 65%
Describe the composition of blood plasma and differentiate between plasma and serum:
Plasma- whole blood minus cells
Serum- plasma without protein clotting factors (straw colored)
Plasma is obtained when blood is collected in an anticoagulant tube, preventing it from clotting. Serum is similar to plasma in terms of its composition but differs in how it is obtained. The serum is obtained after blood has been allowed to clot naturally.
List and describe the importance of the three main proteins found in blood plasma:
Albumins
Buffer blood pH
Osmotic balance
Globulins
protect against disease (immunoglobulins or antibodies)
Fibrinogens
Clotting factors
What is the most abundant protein?
Albumin is 2/3’s of the proteins in the plasma.
Describe the origin, structure, and function of erythrocytes:
Small, biconcave disk
A-nucleate, no ribosomes, no mitochondria
Have to make new protein to stay alive
Makes oxygen and ATP anaerobically
Describe the structure and function of hemoglobin:
Transports oxygen
Accounts for more than 95% of protein in RBC
Transports carbon dioxide when oxygen gets dropped off so it can take over (RBC)
Structure
Protein with 2 alpha chains and 2 beta chains
Heme - non-protein, lipid
Ring with Iron center (binds oxygen)
4 heme per hemoglobin (one per chain)
Heme:
No protein part of hemoglobin that contains several elements that are key to the transportation processes.
Describe the life cycle of erythrocytes from erythropoiesis to RBC destruction:
Erythropoiesis. The life cycle of erythrocytes involves three stages; production, maturity and destruction. Production of erythrocytes (erythropoiesis) is one of the sub-processes of hematopoiesis, happening in the red bone marrow.
Erythropoiesis:
This is dependent on oxygen transport to help balance the amount going throughout the blood.
Pack cell volume increases and RBC count also increases
Erythropotient:
Release of oxygen levels in blood in the kidneys
Names and describe the types, causes and effects of RBC excesses and deficiencies:
Polycythemia and Anemia
Poly- Too many RBC in the blood and can lead to several problems including blood clots.
Anemia- Not enough RBC and can lead to cyanosis and not enough blood and oxygen being transported leading to hemoglobin and iron deficiencies.
List several types and causes of polycythemia and anemia:
Nutritional deficiency
lack of Iron in diet; Iron is a hemoglobin component
Lack of B12 or folic acid needed for cell division
Aplastic Anemia
Bone marrow depression
Hemorrhagic anemia
heavy bleeding and RBC’s are normal but lacking
Hemolytic Anemia
Bed transfusion- elicits immune attack on RBC’s
Genetic conditions
Thalassemia - low amounts of a and b chains
sickle cell anemia- chance in b chain
Hemoglobin molecules stick together
List several types and causes of polycythemia and anemia:
Absolute
primary polycythemia
cancer of the erythropoietic line
secondary polycythemia
all other causes
respiratory problems
high altitudes
excessive aerobic exercise
Relative
dehydration or spleen issues
Describe sickle-cell anemia and explain why the condition remains prevalent in certain geographical locations:
What causes sickle cell disease? Sickle cell is an inherited disease caused by a defect in a gene. A person will be born with sickle cell disease only if two genes are inherited—one from the mother and one from the father. A person who inherits just one gene is healthy and said to be a "carrier" of the disease.
Define and compare leukocytosis and leukopenia:
Leukocytosis is an elevation in the absolute WBC count (>10,000 cells/μL). Leukopenia is a reduction in the WBC count (<3500 cells/μL).
Describe the relative abundance of each type of leukocyte:
White blood cells make up approximately 1% of the total blood volume in a healthy adult, making them substantially less numerous than the red blood cells at 40% to 45%.
What is the name for the clinical measure of the relative abundance of each type of leukocyte?
Differential WBC Count
– Relative abundance of different kinds of WBCs
– Measured by counting numbers of each different
type of WBC in a total of 100 cells
WBC's are composed of granulocytes (neutrophils, eosinophils, and basophils) and non-granulocytes (lymphocytes and monocytes).
Explain the function of leukocytes (WBC’s) in general and the role of each type of leukocyte:
N L M E B
Neutrophils (Granulocyte)
Eosinophytes (Granulocyte)
Basophils (Granulocyte)
Lymphocytes (Agranulocyte)
Monocytes (Agranulocyte/Macrophages)
Neutrophils
60-70%
10-14 μm in
diameter
Multi-lobed nucleus
Phagocytic against
bacteria
– Granules = Lysosomes
Lymphocytes
25-33%
5-17 μm in diameter
Spherical nucleus
Control other immune cells
(T cells)
Secrete antibodies (B cells)
Provide immune memory
Monocytes
3-8%
14-24 μm in diameter
Some become
macrophages within tissues
Functions: Phagocytize viruses, debris and bacteria
Eosinophils
2-4%
10-14 μm in
diameter
Bi-lobed nucleus
Functions:
– Phagocytize
allergens, antibody- antigen complexes, cell debris
Secrete chemicals that weaken parasitic worms
Basophils
<1%
8-10 μm in diameter
Lobed nucleus
Functions:
– Accumulate in
damaged tissues
where they release histamine and heparin.
Secrete to attract other granulocytes
Differentiate between granulocytes and agranulocytes:
The granulocytes are present within the cytoplasm in the form of granules while agranulocytes exist without the granules. The granulocytes have 4 lobes and agranulocytes are single lobes.
List some of the causes and effects of leukocyte excesses:
infections.
smoking.
certain types of leukemia.
emotional or physical stress.
having your spleen removed.
a reaction to medications, including steroids, lithium, or certain types of inhalers.
chronic inflammation caused by injuries, arthritis, or other inflammatory conditions.
Erythro or Hemo:
Red Blood Cells
Leuko:
White Blood Cells
Thrombo:
Platelets
List the functions of platelets and state their origin in the body:
(Thin blood and the spleen)
Stick together/ stick to other things if in rough surfaces or thicker blood (Blood clots)
Small (2-4 μm in diameter),
a-nucleate cell fragments
Conditions if platelet numbers are outside their
homeostatic levels:
– Thrombocytosis – numbers too high
Caused by infection, inflammation, cancer
– Thrombocytopenia – numbers too low
Caused by platelet destruction or inadequate production
Enhance clotting and retract clots
Symptoms: excessive bleeding
Define hemostasis and list the three general stages of the processes:
The stoppage of bleeding
Three phases:
1. Vascular spasm
2. Platelet plug formation
3. Coagulation (Blood Clotting)
Describe two reaction pathways that produce blood clots:
Thrombocytosis - numbers are too high
Caused by infection, inflammation, cancer
Describe two reaction pathways that produce blood clots:
Thrombocytopenia - numbers are too low
Caused by platelet destruction or inadequate production
Symptoms: excessive bleeding
How do intrinsic and extrinsic pathways differ?
Intrinsic - platelets/blood interaction
Extrinsic - Initiated by damaged tissue
Define coagulation and list several factors that must be present for efficient clotting:
Coagulation - amount of clotting
Positive feedback loop
Series of reactions resulting in formation of insoluble fibrin fibers
Reaction cascade allows for a large amount of fibrin to be formed with few starting reactants
Two reaction paths can lead to fibrin formation (Intrinsic and Extrinsic)
Vascular Spasm:
Contraction of smooth muscle (SM) within a
blood vessel wall
SM contraction
→ Release of chemical factors & hormones by endothelial cells
→ More vascular spasm and proliferation of all cell types in the area
Platelet Plug Formation:
Platelet adhesion
Platelets stick to exposed collagen fibers in broken vessel
Platelet aggregation
Attached platelets change shape forming processes to reach out to other platelets
Activated platelets release:
Protein clotting factors
Platelet- derived growth factor (for vessel repair)
Explain what happens to blood clotting when they are no longer needed:
Afterward, the clots usually dissolve. But sometimes a clot doesn't get broken down as it's supposed to. Clots may also form when they're not needed. Sometimes, clots break off a vessel wall and travel through the blood to other parts of the body.
Fibrinolysis
Fibrinolysis is a process that prevents blood clots from growing and becoming problematic. Primary fibrinolysis is a normal body process, while secondary fibrinolysis is the breakdown of clots due to a medicine, a medical disorder, or some other cause.
Explain what keep blood from clotting in the absence of an injury:
Clot Retraction:
Platelets adhere to fibrin and pull torn vessels edges together
Reduces size of damaged area
Can stick to each other or can stick to something surrounding
List several anticoagulants, both naturally produced and clinically applied:
Heparin- synthetic
Warfarin (Coumadin)
Interferes with clotting factors that need vitamin K
Aspirin
Interferes with platelet aggregation
Chelating Agents
Bind up calcium
List several anticoagulants, both naturally produced and clinically applied:
Plasma anticoagulants
Heparin
Released by basophils; stops thrombin production
Thrombomodulin
Released by endothelial cells; changes thrombin activity
Prostacylin
Inhibits platelet aggregation
Describe some bleeding and clotting disorders:
Hemophilia
recessive X-linked genetic disease where clotting factors (Usually factor VIII) are lacking in abundance
Describe some bleeding and clotting disorders:
Thrombus
Clot formed in intact vessel wall
(Often where cholesterol plaques occur)
Can break free and block vessel
Embolus
Abnormal mass (usually a clot) in blood
May start out as a thrombus OR may form spontaneously
Can cause an embolism (Vessel blockage) and subsequent infarct (tissue damage)
E.x. Stroke - infarct in CNS
myocardial infarct (in heart)
Describe the general location, size, and shape of the heart:
Function: Provides pressure for the movement of blood.
Size: About the size of a fist.
Location: Within the pericardial cavity in the mediastinum and the left of midline
Describe the pericardial sac that endorses the heart:
The pericardium consists of two layers: the fibrous and the serous. The fibrous pericardium is a conical-shaped sac. Its apex is fused with the roots of the great vessels at the base of the heart. Its broad base overlies the central fibrous area of the diaphragm with which it is fused.
List and describe the three layers of the heart wall:
Heart wall has 3 layers
Epicardium
Visceral pericardium of areolar and epithelial
Myocardium
Cardiac muscle, blood vessels and nerves
Endocardium
epithelial tissue
Trace the flow of blood through the four chambers of the heart, valves, and adjacent blood vessels (Atria):
Chambers of the heart
2 of these receive blood from the veins
Auricles- areas of the atria that can expand to accommodate blood from the venae cavae (majors veins to heart)
Coronary sulcus = separates atria from ventricles
Trace the flow of blood through the four chambers of the heart, valves, and adjacent blood vessels (Ventricles):
2 of these pump blood into arteries
Separated by:
anterior inter ventricular sulcus
posterior inter ventricular sulcus
Base - area to which blood vessels are attached
Apex - tip of the heart formed by left ventricle
Define and distinguish among the following circulatory circuits: Pulmonary
To and from the capillary beds associated with alveoli in the lungs
Gas exchange blood/tissue and air occurs
Brings deoxygenated blood to the lungs and returns oxygenated blood to the heart.
Define and distinguish among the following circulatory circuits: Systemic
To and from capillary beds of the rest of the body
Gas exchange b/t blood and tissue
Brings oxygenated blood to the tissues and returns deoxygenated blood to the heart
Define and distinguish among the following circulatory circuits: Bronchial
The lung also has a systemic vascular supply, the bronchial circulation, which provides oxygenated blood from the systemic circulation to the walls of the conducting airways, pulmonary arteries and veins.
Define and distinguish among the following circulatory circuits: Cerebral
Cerebral circulation is the movement of blood through a network of cerebral arteries and veins supplying the brain. The rate of cerebral blood flow in an adult human is typically 750 milliliters per minute, or about 15% of cardiac output. Arteries deliver oxygenated blood, glucose and other nutrients to the brain.
Define and distinguish among the following circulatory circuits: Coronary
The coronary arteries also supply the myocardium with oxygen to allow for the contraction of the heart and thus causing circulation of the blood throughout the body. Two main coronary arteries originate from the base of the aorta as it exits the left ventricle: the left and right coronary arteries. (First branch off the aorta)
Only one of these circuits experiences an increase in oxygen levels…
The Pulmonary Circuit
Describe the purpose of the four valves of the heart: Atria and AV valves
Vessels: Conduct for blood movement
Atrioventricular AV valves
(Tricuspid - right) (Bicuspid - left)
Allow blood to flow from atria to ventricles (open when ventricles relax)
Prevent flow from ventricles to atria (close when ventricles contract
NOTE: Ventricles contract to make AV valves close
Ventricles contract to make AV valves open
Ventricles relax to make SL valves close
Describe the purpose of the four valves of the heart: Ventricles and SL valves
Semilunar (SL) valves
(Pulmonary SL valve) (Aortic SL valve)
Allows blood to flow from ventricles to arteries (Open when ventricles contract)
Prevent back flow from arteries to ventricles (Close when ventricles relax)
Differentiate among the Myocardium pectinate muscle, and papillary muscle:
Myocardium: It is the heart muscle that contracts and causes the heart to pump deoxygenated blood to the lungs and the oxygenated blood to tissues.
Pectinate: The function of pectinate muscles is to increase the power of contraction without increasing heart mass substantially.
Papillary: They are attached by fine strands of tendon to the valves between the atria and ventricles and prevent the valves from opening when the ventricles contract.
List and describe three heart valve disorders:
Rheumatic Heart Disease: Rheumatic heart disease is a condition in which the heart valves have been permanently damaged by rheumatic fever. Rheumatic fever is an inflammatory disease that can affect many connective tissues, especially in the heart. Untreated or under-treated strep infections put a person at increased risk.
Stenosis: Aortic valve stenosis is a thickening and narrowing of the valve between the heart's main pumping chamber and the body's main artery, called the aorta. The narrowing creates a smaller opening for blood to pass through. This reduces or blocks blood flow from the heart to the rest of the body. (Hardening)
Murmur: These sounds occur as the heart valves open and close to allow blood to flow through the heart. A heart murmur is an extra noise heard during a heartbeat. The noise is caused when blood does not flow smoothly through the heart.
Occlusion:
Blockage resulting in oxygen and nutrition deprivation
Ischemia:
State of oxygen deficit
Infarction:
Area of cell death (necrosis) caused by anoxia
Caused bu blockage of blood delivery/drainage
List the unique properties of cardiac muscle:
Entire organ contracts all or none
Long refractory period
Self-excitatory - not dependent of the nervous system
there’s a rhythm in the heart that pace the action potentials
Differentiate between autorythmic and contractile cardiac muscle cells (CMC’s):
Autorythmic CMC:
Produce pacemaker potentials
Conduct impulses through heart muscle
Contractile CMC:
Produce contraction leading to alternating
Systole (contraction)
Diastole (relaxation)
Differentiate between systole and diastole:
Systole occurs when the heart contracts to pump blood out, and diastole occurs when the heart relaxes after contraction.
Explain how the quantities and relative movement of sodium, calcium and potassium affect the action potential within autorythmic and contractile CMC’s:
These cells are self‐excitable, able to generate an action potential without external stimulation by nerve cells. The auto rhythmic cells serve as a pacemaker to initiate the cardiac cycle (pumping cycle of the heart) and provide a conduction system to coordinate the contraction of muscle cells throughout the heart.
Sodium- Slow inflow
Calcium- Fast inflow
Potassium- Fast outflow
Describe the internal electrical system of the heart:
Your heart's electrical system controls the timing of your heartbeat by regulating your: Heart rate, which is the number of times your heart beats per minute. Heart rhythm, which is the synchronized pumping action of your four heart chambers.
Contracts:
Atria
Ventricle (Perkunje)
AP spreads rapidly through conduction system to contractile cells
Trace the movement of the electrical signal throughout starting with the SA node:
The SA node starts the sequence by causing the atrial muscles to contract. That's why doctors sometimes call it the anatomical pacemaker. Next, the signal travels to the AV node, through the bundle of HIS, down the bundle branches, and through the Purkinje fibers, causing the ventricles to contract.
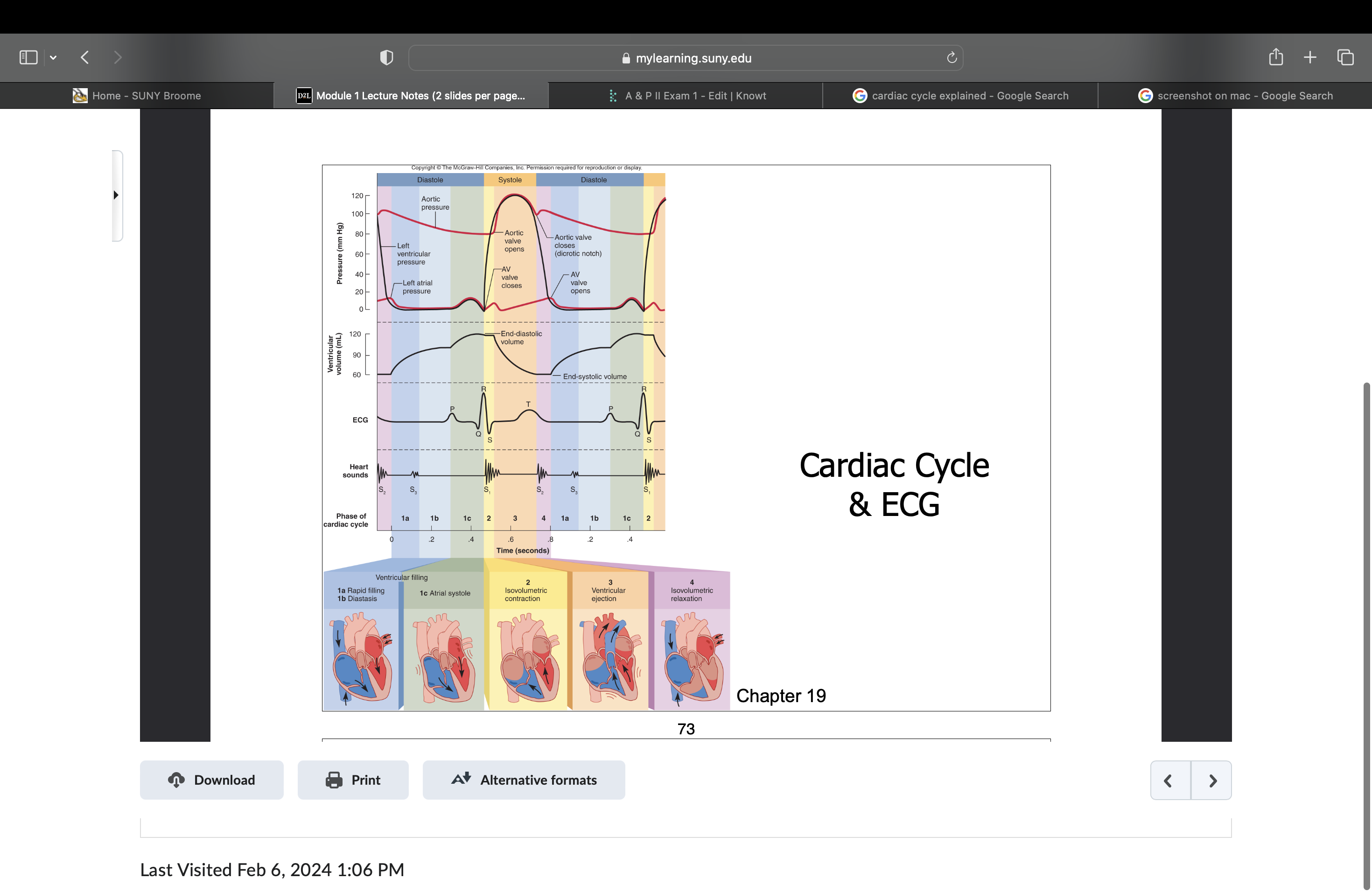
Interpret a normal electrocardiogram (ECG):
P wave
atrial depolarization
QRS complex
Ventricular depolarization
T wave
Repolarization of ventricles
Depolarize = Contraction = Systole
R wave is bigger than the P wave because there are more contractile cells, ventricles in the R wave section are stronger.
Describe the terms bradycardia, tachycardia, flutter and fibrillation:
Sinus bradycardia - SA node impulses initiated at low rate (<60/min)
Sinus Tachycardia- SA node impulses initiated at high rate (>100/min)
Atrial flutter- 200-300 APs/min
Atrial fibrillation- 450-600 APs/min
Describe in detail one complete cycle of heart contraction and relaxation:
Ions: Na and Ca = depolarization (contraction)
Ions: K = repolarization (relaxation)
T wave, things start to relax
Ventricles are most full in the systole stage
When ventricles are in systole they increase rapidly, causing semilunar valves to open.
Explain isovolumetric contraction:
The phase of systole when both valves are closed (and, as a result, the productive flow is zero)
Define cardiac output and explain its importance:
CO= volume of blood ejected per minute
Depends on:
Heart Rate (HR) - beats per minute
Depends on ANS
Stroke volume (SV) - volume ejected per beat
CO = HR (Beats/Min) x SV (Volume/Min)
(Same amount of blood and pressure within the right and left ventricle)
Define stroke volume and heart rate and explain how one might calculate cardiac output:
Cardiac output is the product of heart rate (HR) and stroke volume (SV) and is measured in liters per minute. HR is most commonly defined as the number of times the heart beats in one minute. SV is the volume of blood ejected during ventricular contraction or for each stroke of the heart.
Describe preload, after load and ventricular contractility and explain how these factors can alter stroke volume:
Pre load - End-Diastolic Volume (EDV)
Higher pre load = higher SV
After load
Pressure of blood in arteries (Aorta)
Higher after load = smaller SV
Ventricular Contractility
Efficient contraction of ventricular myocardium
Before ventricles pump, they have to be full
Describe some of the nervous, hormonal and chemical factors that alter the heart rate and over contractility of the heart: Contractility
Positive IA increase contractility
sympathetic innervation = Ca+ influx and increase
Cardiac glycosides
Epinephrine and caffeine
Negative IA decrease contractility
Hyperkalemia
Calcium channel blockers
Describe some of the nervous, hormonal and chemical factors that alter the heart rate and over contractility of the heart: Heart Rate
Increase:
Sympathetic division of the ANS
Increase AP at SA node
Increased responses of AV node = less delay
Hormones
Epinephrine
Thyroxine
Altered ions
Hypocalcemia
Spastic contraction
Increased temperature
Describe some of the nervous, hormonal and chemical factors that alter the heart rate and over contractility of the heart: Heart Rate
Decrease:
Parasympathetic division of ANS
Decrease at SA node
Decreased AP conduction at AV node
Altered ions
High and low potassium interfere with AP’s
Decreased temperature
Explain how a change in blood pressure would result in a change in cardiac output and peripheral resistance (PR) via a baroreceptor negative feedback mechanism:
Respond to baroreceptors for arterial and atrial blood pressure for neutral control of BP
Negative Feedback:
If BP is too low:
Increase in HR/SV - Increase in CO - Increase in BP
AND generalized vasoconstriction - Increase in PR/BP (Sympathetic “fight or flight” mode)
If BP is too high
Decrease in HR/SV/CO/BP
AND generalized vasodilation - decrease in PR/BP (Parasympathetic ANS “rest and digest” mode)
Explain how a change in oxygen concentration, carbon dioxide concentration, or pH would result in a change in cardiac output or peripheral resistance via a chemoreceptor negative feedback mechanism:
Respond to chemoreceptors in aortic arch and large arteries in the neck for neural control of BP
Negative feedback:
If oxygen is LOW, pH is LOW, CO2 is HIGH
Increase in HR/PR (generalized vasoconstriction by norepinephrine)
Increase in BP
If oxygen is HIGH, pH is HIGH, CO2 is LOW
Decrease in HR/PR (generalized vasodilation by inflammatory chemicals)
Decrease in BP
Describe some effects of exercise on cardiac output:
Cardiac output during exercise increases greatly owing to the relatively high heart rates that are achieved during exercise. Heart rate increases proportionately with workload until heart rates close to maximal are attained.
Describe the structure of a blood vessel:
Function:
Delivery of nutrients and oxygen
Removal of wastes
Types of vessels:
Arteries
Carry blood away, under high blood pressure from the heart
Elastic or muscular
Arterioles = smaller arteries with organs
Capillaries
Sites of materials exchange b/t blood and tissues
Veins
Return blood (under low pressure) to heart
Venules = smaller and leaky
Sinuses = flatted venous reservoirs
Describe the different types of arteries, capillaries and veins:
Arteries carry blood away from your heart. Veins carry blood back toward your heart. Capillaries, the smallest blood vessels, connect arteries and veins
Trace the route usually taken by the blood from the heart to the tissues and back again:
Systemic circulation carries oxygenated blood from the left ventricle, through the arteries, to the capillaries in the tissues of the body. From the tissue capillaries, the deoxygenated blood returns through a system of veins to the right atrium of the heart.
Explain the relationship between blood pressure, peripheral resistance, and velocity of blood flow:
The constriction of arterioles increases resistance, which causes a decrease in blood flow to downstream capillaries and a larger decrease in blood pressure. Dilation of arterioles causes a decrease in resistance, increasing blood flow to downstream capillaries and a smaller decrease in blood pressure.
Describe the relative distribution of blood among arteries, capillaries and veins:
Arteries transport blood away from the heart and branch into smaller vessels, forming arterioles. Arterioles distribute blood to capillary beds, the sites of exchange with the body tissues. Capillaries lead back to small vessels known as venules that flow into the larger veins and eventually back to the heart.
Define the term perfusion:
Blood supply to a certain region, fight or flight. Can choose which part of the body gets blood at a point in time. (Blood can not be supplied everywhere at the same time)
Explain the forces that keep blood flowing back to the heart in the veins:
Heart valves
The valves prevent blood from flowing backward. The heart has four valves. The tricuspid valve separates the right atrium and right ventricle. The mitral valve separates the left atrium and left ventricle.
How do veins prevent the pooling of blood in the lower extremities:
The valves also control the pressure in smaller veins on the legs' surface. If the valves within the veins fail to work properly, there is a blockage to normal flow, or the calf muscles cannot pump properly, blood can flow backwards in the veins and pool in the legs
Define and describe the various types of hypotension and hypertension:
High blood pressure (hypertension) occurs when the force of blood against the artery walls is too strong, while not enough force is the problem with low blood pressure (hypotension)
Differentiate among continuous, fenestrated and sinusoid types of capillaries:
Continuous:
Complete endothelium with tight junctions
Blood-brain barrier
Fenestrated:
Porous endothelium; very permeable
Small intestine, kidney
Sinusoid:
Incomplete endothelium; slows blood flow
Liver, spleen, lymphoid tissue
Describe the forces that enable capillaries to exchange materials between blood and tissues:
As blood passes from arteries to veins through the capillary bed, fluids are exchanged by diffusion, the movement of molecules from areas of high pressure to low pressure. This relies on two forces: hydrostatic pressure, or blood pressure, and osmotic pressure, the constant pressure needed to keep blood from diffusing.
Distinguish between capillary hydrostatic and osmotic pressure:
Capillary hydrostatic pressure
Physical pressure on capillary walls
“Pushing” fluids out
Blood Pressure
Plasma Osmotic Pressure
Physical draw by solutes on the more concentrated side of capillary walls
“Pulling” fluids in
Filtration
Describe the causes and effects of edema:
Edema is swelling caused by too much fluid trapped in the body's tissues. Edema can affect any part of the body.
Describe atherosclerosis and arteriosclerosis:
Arteriosclerosis is the condition of the arterial walls where there is a development of thickness and hardening and atherosclerosis is a type of this condition where there is significant plaque buildup.
Define aneurysm:
Localized dilation or out pouching of a blood vessel.
Describe how varicose veins form:
When the valves become weakened or damaged, blood can collect in the veins. This causes the veins to become enlarged. Sitting or standing for long periods can cause blood to pool in the leg veins, increasing the pressure within the veins. The veins can stretch from the increased pressure.