Cytotoxic Chemotherapy (2)
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
describe the MOA of anthracyclines (antitumour antibiotics)
DNA intercalation- drug physically inserts between base pairs and causes distortion of the DNA helix and inhibition of RNA transcription and DNA synthesis
Poisoning of topoisomerase II- leads to stabilisation of the topoisomerase II-DNA cleavage complex and consequently the accumulation of dsDNA breaks
Topo-II is the enzyme responsible for untangling the DNA during replication
Redox cycling of the quinone group via NADPH-dependent enzymes such as CYP450 reductase. this causes generation of ROS
describe the MOA of doxorubicin (DOX), how it is administered and when it is used
MOA of DOX- it intercalates preferentially in GC-rich regions of DNA
Administered intravenously
Used for breast cancer, lymphomas, sarcomas, leukaemia and solid tumours
though cell cycle non-specific which cycle phase are cells more sensitive to DOX and why
cytotoxicity of DOX is enhanced at the S/G2 phase
S phase- cells have increased sensitivity in this phase due to active DNA replication and topoisomerase II-mediated strand cleavage
G2 phase- it is dependent on topo II for decatenation of sister chromatids before mitosis
describe the side effects of DOX and what it means to be a vesicant chemotherapeutic
Side effects- emetogenic, alopecia, harmless urine discolouration for 1-2 days post-dose (this can be alarming to patients if they are not warned)
vesicant chemotherapeutic
if the drug leaks out of the vein during infusion it causes severe tissue damage that may create a need for skin grafting
Once the drug leaks it out it enters healthy cells, binds to their DNA and kills the cells which causes them to undergo lysis
Lysis causes the release of DOX into the environment and it is then taken up more normal cells
DOX is cleared slowly by the local microenvironment so it continues to have prolonged toxicity and the injury evolves over time leading to severe tissue
name the major organ toxicities of DOX and state which is the primary dose limiting toxicity
Cardiotoxicity- this is the primary dose-limiting toxicity
Myelosuppression
Mucositis (inflammation and ulceration of GI mucosa)
Hepatotoxicity (though less prominent)
name and describe the 3 types of cardiotoxicity DOX causes
acute (rare)
ECG changes, transient arrhythmias, rarely myocarditis
chronic (dose limiting)
Progressive dilated cardiomyopathy resulting from cumulative cardiomyocyte injury
OS, MD, TOP2-beta inhibition causes reduced left ventricular ejection fraction
progress to heart failure due to myofibrillar deterioration and intracellular calcium dysregulation
huge risk seen at total doses ≥450 mg/m²
late/delayed
manifest years/decades after treatment, particularly in childhood cancer survivors
name the mechanisms of DOX cardiotoxicity
oxidative stress
disrupts mitochondrial function
topoisomerase II
calcium dysregulation and cardiomyocyte injury
Mechanisms of cardiotoxicity- describe the process of DOX-mediated oxidative stress
DOX is enzymatically reduced into an unstable semiquinone radical
This radical reacts with oxygen and that triggers a redox cycle that amplifies ROS production
ROS induces lipid peroxidation, protein oxidation and DNA damage
Cardiomyocytes are particularly susceptible due to their low antioxidant capacity (e.g. low levels of catalase)
Mechanisms of cardiotoxicity- describe how DOX disrupts mitochondrial function
DOX impairs mitochondrial function via ROS-dependent and independent mechanisms
ROS-dependent: mitochondrial lipid peroxidation, impaired ATP production, oxidative damage to respiratory chain complexes
ROS-independent (inhibition of TOP2-beta): altered transcription of genes regulating mitochondrial biogenesis and oxidative phosphorylation which leads to impaired mitochondrial respiratory chain function
Mitochondrial dysfunction promotes the opening of mPTP which leads to a loss of mitochondrial membrane potential and activation of cell death pathways
Interaction of DOX with cardiolipin in the inner mitochondrial membrane promotes mitochondrial retention of DOX and facilitates ROS generation, contributing to a self-amplifying cycle of redox cycling, energy failure and cell injury in the cardiomyocytes
Mechanisms of cardiotoxicity- describe the effect of DOX on topoisomerase II
ATP-dependent enzyme that regulates the DNA topology- supercoiling, decatenation and chromosome segregation
It creates transient dsDNA breaks to relieve torsional stress and this is essential for DNA replication and transcription
2 isoforms: alpha (dividing cells, antitumour effects), beta (non-dividing, cardiotoxicity)
DOX poisons Topo-II in tumour cells (mainly alpha) and cardiomyocytes (beta) this leads to persistent dsDNA breaks, increased p53 signalling and apoptosis
DOX also causes cytotoxicity through Topo-II independent mechanisms
forms covalent DNA adducts after formaldehyde-mediated activation
Mechanisms of cardiotoxicity- describe how DOX causes calcium dysregulation and cardiomyocyte injury
DOX disrupts SR Ca2+ storage and homeostasis
DOX binds and blocks SERCA2a and RyR2 which reduces Ca2+ reuptake into SR and increases abnormal Ca"+ leak respectively
RyR Ca2+ leak is partly driven by ROS-mediated oxidative modification of RyR2
As a results, there is reduced Ca2+ storage in SR and increased cytosolic Ca2+
Mitochondria take up the excess Ca2+ leading to mPTP opening, CytC release and apoptosis
Cytosolic Ca+ overload also activates calpain-mediated proteolysis and other Ca2+ dependent pro-apoptotic pathways
describe the MOA of mitotic inhibitors (M-phase specific) and name 2 examples
These drugs disrupt the mitotic spindle dynamics, thereby preventing proper chromosome segregation
leads to activation of the spindle assembly checkpoint which consequently leads to metaphase arrest and apoptosis
2 subgroups:
Vinca alkaloids e.g. Vincristine
Taxanes e.g. docetaxel
describe the MOA of vinca alkaloids
MOA- bind to vinca domain on the beta subunit of tubulin, which is the building block of MT and inhibits its polymerisation and therefore the formation of functional mitotic spindles
describe the MOA of taxanes
MOA- enter cells via passive diffusion (primary route) or membrane transporters (depending on cell type) and bind to beta tubulin. It stabilises the microtubules, prevents depolymerisation, thereby disrupting spindle function
describe the toxicity profile for taxanes and how some can be managed
narrow therapeutic window
dose limiting toxicity is the myelosuppression especially neutropenia
peripheral neuropathy
stocking glove pattern- numbness and tingling in hands and feet; moves distally to proximally
due to disrupted axonal MT transport
fluid retention
hallmark of docetaxel not vincristine
requires dexamethasone premedication
hypersensitivity
managed with corticosteroids and antihistamines
nail changes and alopecia
hepatoxicity due to metabolism by CYP3A4/5
describe the MOA of docetaxel fluid retention
caused through a process called capillary leak syndrome where fluid escapes from capillaries into surrounding tissues
mechanism is not fully understood but involves several interconnected pathways
DOC damages endothelial cells lining small blood vessels
this increases their vascular permeability leading to plasma fluid and proteins leaking into the interstitial space
results in peripheral edema
DOC also stabilises MTs and prevents normal MT dynamics
endothelial cells depend on cytoskeletal remodelling to maintain tight junction and regulate permeability
if there is disruptions to the MT function it can cause dysfunctional endothelial barrier integrity and disrupt actin-MT coordination
results in a leaky capillary
dexamethasone premedication
it stabilises the endothelial barriers by tightening intercellular junctions to decrease leakage from capillaries
MOA of cytotoxicity of antimetabolites and name 2 examples
S-phase specific agents that result in DNA synthesis failure
examples- methotrexate and 5-fluorouracil
describe the MOA of methotrexate and the toxicity profile
MOA- inhibit dihydrofolate reductase (DHFR) which prevents generation of tetrahydrofolate. This depletes folate pools required for synthesis of thymidylate (dTMP) and purines and therefore impairs DNA replication
TOXICITY PROFILE
Myelosuppression is common and dose-limiting
GI toxicity- mucositis (dose limiting), stomatitis
Hepatotoxicity especially with chronic use
Nephrotoxicity because it crystallises in renal tubules
Clinicians alkalinise the urine using sodium bicarbonate to avoid this
Cardiac effects are rare
discuss the mechanism of MTX-mediated hepatotoxicity
chronic use of MTX is associated with fat accumulation and fibrosis with a potential to progress to cirrhosis
aside from MTX main mechanism of exerting cytotoxicity (explain?)
MTX also interferes with methylenetetrahydrofolate reductase (MTHFR) and hence the generation of methionine from homocysteine
this leaves excess homocysteine which causes ER stress which can lead to accumulation of fat (e.g. triglycerides) in the hepatocytes
homocysteine can also activate pro-inflammatory cytokines and activate hepatic stellate cells leading to liver fibrosis
describe the metabolism of 5-fluorouracil and how this relates to its MOA
This can be converted to multiple active metabolites:
FUTP- this incorporates into the RNA and disrupts RNA processing and function
FdUMP- this inhibits thymidylate synthase and blocks conversion of dUMP to dTMP which leads to dTMP depletion, thymidine deficiency and 'thymineless death'
describe the toxicity profile of 5-fluorouracil
Myelosuppression is common
GI toxicity- mucositis (dose limiting)
Neurotoxicity
Hand-foot syndrome- patient experiences redness, soreness and peeling in palm and soles of their food
Important to check for DPD deficiency as 5% of population have partial or complete deficiency of this enzyme → 5-FU accumulation
Can cause acute coronary vasospasm
describe the MOA of leucovorin (folinic acid) in the presence of MTX or 5-FU
MTX
rescue cells from MTX effect by bypassing DHFR block and providing reduced folate to healthy cells.
This restores nucleotide synthesis in normal cells
needs to be gap between MTX and leucovorin administration
because MTX needs to damage tumour cells then leucovorin is given to rescue the normal cells
Cancer cells have reduced capacity to take up leucovorin and retain MTX longer than normal cells
5-FU
inhibits thymidylate synthase to stop DNA synthesis
does this increasing 5,10-methylene-THF which is the specific form required to stabilise binding of FdUMP to thymidylate synthase
leads to strong TS inhibition and increases drug efficiency
describe the peripheral pathway of chemotherapy induced nausea and vomiting
peripheral (within 24hrs)
This is primarily driven by 5HT
It damages enterochromaffin cells in the small intestine, release large amounts of 5HT
5HT binds to 5HT3R on the vagal afferent nerves; these receptors are the primary drivers of acute emesis
Signals are then transmitted to the vomiting centre
Clinical implication- 5HT3R antagonists such as ondansetron are effect in preventing acute CINV
describe the central pathway of chemotherapy induced nausea and vomiting
central
Dopamine acts primarily on D2R area postrema in the CTZ located in the medulla outside the BBB
This means that the CTZ is directly exposed to drugs and toxins
This sends signals to the NTS and activates the vomiting central
describe the delayed phase (>24hrs) pathway of chemotherapy induced nausea and vomiting
Driven by SP which is the primary driver of delayed emesis
SP acts on NK1R in the brainstem
Clinical implications- NK1R antagonists e.g. aprepitant are used to target this pathway
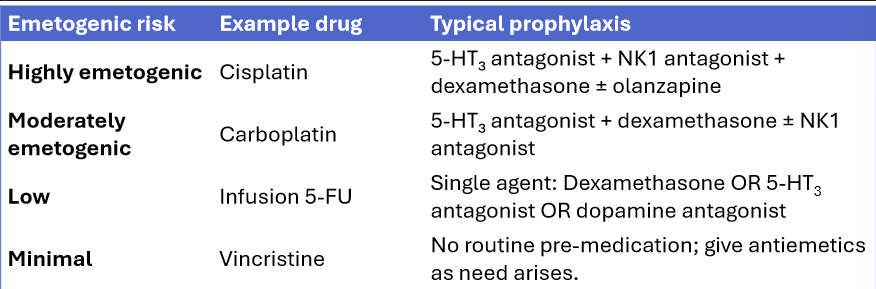
define the emetogenic risk
The emetogenic risk is the likelihood that a medication will cause nausea and vomiting (emesis) without preventative treatment
using specific examples of drugs with different levels of emetogenic risk, state the drug used for antiemetic prophylaxis
Antiemetic prophylaxis depends on the emetogenic risk of the chemotherapy regimen
corticosteroids e.g. dex enhance antiemetic efficiency
describe mucositis as a chemotherapy induced side effect
Mucositis is inflammation and ulceration of the oral and GI mucosa caused by damage to rapidly dividing mucosal epithelial cells, including intestinal crypt cells
MOA- ROS generation and DNA damage leads to epithelial apoptosis which activates NFkB signalling, induces proinflammatory cytokine release (TNF-alpha, IL1-beta, IL6) which causes mucosal breakdown and ulceration
clinically seen as stomatitis- pain, dysphagia, reduced oral intake
describe the chemotherapy agents associated with mucositis and how it be managed
associated with antimetabolites, some alkylating agents and anthracyclines
management
oral hygiene, analgesics such as cryotherapy where ice chips are given during 5-FU infusion, and palifermin which is a keratinocyte growth factor given to high risk patients
The ice chips cause vasoconstriction and so slow down how fast the drug reaches the GI are
discuss the clinical implications of known cell cycle specificity of tumour cells
Tumours contain cells in different cell cycle phases at any given time
Resistance- repeated exposure kills sensitive cancer cells but allows resistant ones to survive and these may repair DNA damage or change how they divide making the drug less effective over time
Combination regimens are now designed to: target tumour cells across multiple cycle phases by combining phase specific and non-specific agents, exploit different cytotoxicity mechanisms, reduce likelihood of resistance and use non-overlapping toxicity profiles (e.g. avoid 2 nephrotoxic agents)