Ch. 30 Perio Surgery Pt. 1
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
Primary Goals of Periodontal Surgery:
1. To eliminate the pathologic changes in the pocket
2. To create a stable and easily maintainable healthy state of the periodontium throughout the life of the patient
***Surgery is necessary when the periodontitis cannot be controlled with nonsurgical periodontal therapy alone.
Historical Perspective for Periodontal Surgery:
Until the middle of the 20th century perio surgery procedures were resective
Recommended for removal of what was thought to be dead or infected periodontal tissues
Refers to those procedures that simply cut away and remove damaged tissues
Today, resective procedures are not commonly used in periodontal care (Good for gingivectomy)
Modern Periodontal Surgical Techniques
Basic sciences and regenerative medicine has advanced
Emphasis has shifted from resective surgery to regenerative surgical techniques
Regenerative- attempt to rebuild or regenerate lost periodontal tissues
Most modern surgeries begin with a periodontal flap
Now we add regenerative products under the incision to regrow the tissue
Indications for Periodontal Surgery:
1. To provide access for improved instrumentation of root surfaces
2. To reduce pocket depths
3. To provide access to defects in the alveolar bone (AKA-osseous defect)
4. To resect or remove tissue
5. To regenerate the periodontium lost due to disease
6. To graft bone or bone-stimulating materials into osseous defects
7. To improve the appearance of the periodontium
8. To enhance prosthetic dental care
9. To allow for the placement of a dental implant
1. Access for Periodontal Instrumentation
Pockets increase, resulting in challenging to reach the base of the pocket
Surgery allows for increased access and visualization of the root surfaces
Nonsurgical (NSPT) is challenging with deep pockets.
Ex. Flap surgery
2. Reduction of Pocket Depths
Biofilms thrive in deep pockets resulting in challenging control of periodontitis
Surgical procedures reduce pocket depths so that a combination of self-care and professional care increases the chance of controlling periodontitis
3. Access to Osseous Defects
An osseous defect is a deformity in the tooth supporting the alveolar bone- usually a result of periodontitis
Alveolar bone loss modifies the normal contour and structure of the bone
Bone defects can be managed by periodontal surgery
4. Resect or Remove Tissue
Needed when there is overgrowth or enlargement of gingival tissue
Overgrown tissue may interfere with normal eating
Surgery can remove and reshape the gingiva
“Gummy Smile”
5. Regenerate the Periodontium Lost due to Disease
Defined: The reconstitution of new tissue=
to grow back cementum, PDL, & alveolar bone
Possible to achieve in some instances with sophisticated periodontal surgical techniques
$$$ - Remember Emdogain from chapter 28?
6. Graft Bone or Bone-Stimulating Materials
Grafting of bone or bone-stimulating materials into an osseous defect
Does not necessarily mean there will be regeneration of the lost cementum or the lost PDL
Again $$$ but worth it!!
7. To Improve Appearance of the Periodontium
Some patients may have gingival levels or contours that result in an unattractive smile
Periodontal surgery may improve the quality of a patient’s smile.
8. Enhance Prosthetic Dental Care
Modern periodontal surgery includes many procedures directed toward enhancing restorative dentistry
Altering alveolar ridge contours
Lengthening tooth crowns
Augmenting the amount of gingiva
Augmenting the bone prior to the implant placement
9. Allows for Placement of Dental Implants
Periodontal surgery can be used to prepare sites for dental implants
Dental implants must be surrounded by sound alveolar bone
Periodontal Surgery Contraindications:
Most contraindications for periodontal surgery are relative contraindications
Relative contraindications are conditions that may make surgery inadvisable for some patients when the conditions or situations are severe or extreme. Ex elevated BP
An absolute contraindication is a situation that makes a particular treatment absolutely inadvisable. Ex. Patient with full blown AIDS
Relative Contraindications for Surgery:
Patients who:
1. Have certain systemic diseases
2. Are totally noncompliant with self-care
3. Have a high risk for dental caries
4. Have unrealistic expectations for the outcomes of periodontal surgery
Systemic Diseases and Conditions:
Recent history of heart attack
Uncontrolled hypertension
Uncontrolled diabetes
Certain bleeding disorders
Kidney dialysis
History of radiation to the jaws
HIV infection
Self-Care Noncompliance:
Outcomes of many types of surgery depend on the level of the patient’s efforts with plaque control
Poor self-care can cause a poor periodontal surgical outcome
High Risk for Dental Caries:
Periodontal surgery can expose portions of the tooth root
High risk caries patients may have rampant root caries
Unrealistic Expectations of Surgical Outcomes:
Surgical correction of damage to diseased tissues does not always result in a perfectly restored periodontium
For example, pocket reduction can result in portions of the tooth root being exposed in the oral cavity
Patients have to develop realistic expectations for surgical outcomes
Outcomes of Modern Periodontal Surgery:
Readaptation of soft tissue to the tooth root by formation of a long junctional epithelium
Resolution of inflammation associated with periodontal pockets
Regeneration – a restored periodontium; an expectation for periodontal regenerative surgery but not expected as the result of nonsurgical periodontal therapy alone.
Terminology Used to Describe Surgical Wound Healing:
1. Healing by repair
2. Healing by reattachment
3. Healing by new attachment
4. Healing by regeneration
Healing by REPAIR
healing of a wound by formation of tissues that do NOT precisely restore the original architecture or original function of the body part
Example---formation of a scar during healing of a cut to a finger
Healing the Periodontium by REPAIR:
Healing after periodontal instrumentation results in a long junctional epithelium
A long junctional epithelium does NOT precisely duplicate the original periodontal tissues
No formation of new bone
No formation of new cementum
No formation of periodontal ligament
Healing by REATTACHMENT:
healing by the reunion of the periodontal connective tissue and tooth root where the two tissues have been separated by incision or injury, but NOT by disease
Example---temporarily moving healthy tissue away from the tooth root or bone during crown lengthening.
Healing by NEW ATTACHMENT:
New attachment---healing that occurs when epithelium and connective tissues are newly attached to a tooth root where periodontitis had previously destroyed this attachment
New attachment occurs in an area damaged by disease
Again, Reattachment occurs in the absence of disease, such as in a surgical procedure.
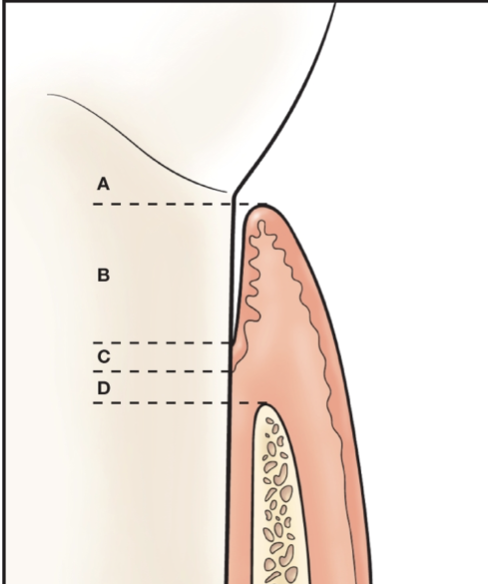
To qualify as new attachment, the tissues must be attached to the tooth surface in the area where on this picture?
B-area of attachment loss
Healing by REGENERATION:
regrowth of the precise tissues that were present before the disease or damage to the tissues occurred
REGENERATION of the Periodontium:
The healing would have to result in the reformation of the lost cementum, lost periodontal ligament, and lost alveolar bone
Regeneration of the periodontium is possible with modern surgical procedures
Unfortunately, the periodontium cannot be regenerated predictably in all sites with current surgical techniques
Terminology to Describe the Degree of Wound Closure:
1. Healing by primary intention
2. Healing by secondary intention
3. Healing by tertiary intention
1. Primary Intention:
Occurs when the wound margins are closely adapted to each other
Ideally, all wounds created by periodontal surgery would heal by primary intention, but often this is not possible
Difficult in periodontics since one edge of the surgical wound is the tooth root that cannot contribute any living cells to the wound healing
2. Secondary Intention:
Margins or edges of the wound are not close in contact with each other
Granulation tissue must form to close the space between the wound margins and then the epithelial cells grow over the surface of the wound
Many wounds in periodontal surgery involve healing by secondary intention
3. Tertiary Intention:
Tertiary intention---healing of a wound that is temporarily left open with the specific intent of surgically closing that wound at a later date
Not normally a type of healing that applies to periodontal surgery
“Needs to heal from within & could create abscess if closed too soon.
Ex. A dog bite
Periodontal Flap:
Defined: is a periodontal surgical procedure in which incisions are made in the gingiva or mucosa to allow for separation of the epithelium and connective tissues from the underlying tooth roots and underlying alveolar bone
Periodontal Flap Procedure:
Incision made to allow for separation of the soft tissue from the roots and alveolar bone
The soft tissue is lifted temporarily from the teeth and alveolar bone
Improved visualization of both the tooth roots and alveolar bone contours
Elevation or Reflection of Tissue:
Elevation---separating the epithelium and connective tissues from the underlying tooth root and alveolar bone
Once these tissues are elevated, they can be replaced at the original position or moved to different locations
Indications for a Periodontal Flap:
To provide access to tooth root surfaces for completion of meticulous periodontal instrumentation that was begun as part of the nonsurgical periodontal therapy
To provide access to reshape or treat alveolar bone defects resulting from periodontitis
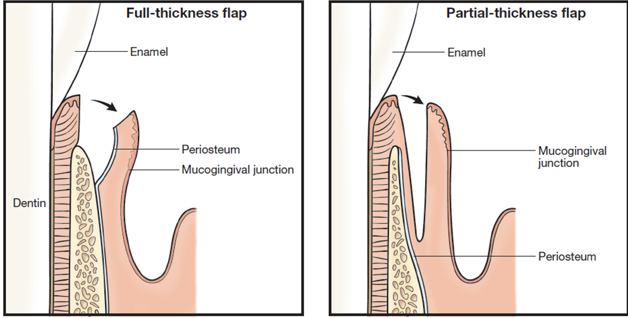
Classification of Periodontal Flaps:
Based on bone exposure
1. Full-thickness flap
2. Partial-thickness flap
Based on location of the flap margin
1. Nondisplaced flap
2. Displaced flap

1. Full-Thickness Flap
Also called a mucoperiosteal flap
Lifting of the entire thickness of soft tissue
Provides complete access to the underlying alveolar bone
BLUNT instruments are used to elevate the flap in a manner quite similar to lifting the peel off an orange

2. Partial Thickness Flap:
Elevation only of the epithelium and a thin layer of the underlying connective tissue
Sharp instruments are used for a partial-thickness flap
Nondisplaced Flap:
A flap that is sutured with the margin of the flap placed at its original relationship to the CEJ of the tooth
Analogy: the window shade goes up, window shade comes back down
Displaced Flap:
A flap that is sutured with the margin of the flap placed at a position other than its original position in relation to the CEJ
A displaced flap can be positioned apically, coronally, or laterally in relationship to its original position
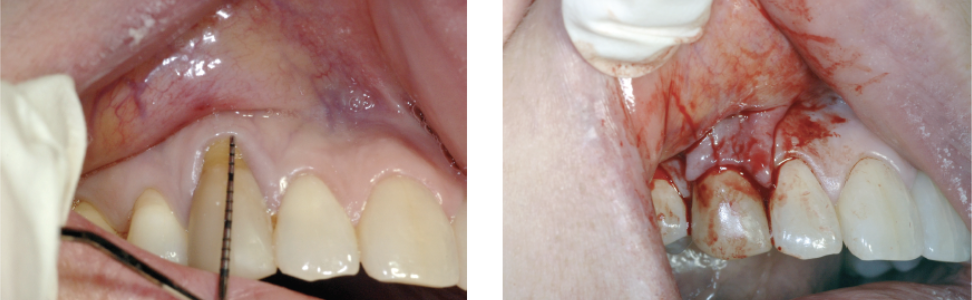
Types of Incisions Used During Periodontal Flap Surgeries:
Horizontal---run parallel to the gingival margin in a mesiodistal direction
•1. Inverse bevel incision- left photo-initial incision
•2. Crevicular incision –right photo-2nd incision
3. Vertical Incision- runs perpendicular to the gingival margin in an apico-occlusal direction
Releases sides
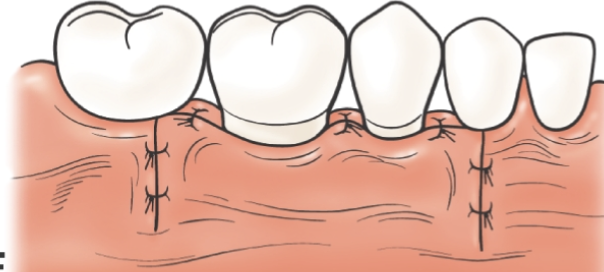
Displaced Flap with a Photo:
A flap that is sutured with the margin of the flap placed at a position other than its original position in relation to the CEJ
A displaced flap can be positioned apically, coronally, or laterally in relationship to its original position
Types of Periodontal Surgery: Flap for Access
Also called modified Widman flap surgery
Provides access to tooth roots for improved root preparation
Tissue is lifted long enough for the procedure
After completion of the procedure, tissue is replaced at the original position
Sutured in place (Shade up Shade down)
Special Considerations for the Dental Hygienist– Flap for Access
Difficult to remove all calculus deposits in pocket depths deeper than 6 mm in nonsurgical periodontal instrumentation
Flap for access surgery allows more efficient and meticulous instrumentation of root surfaces
Types of Periodontal Surgery: Open Flap Debridement
Similar to flap access except:
More extensive flap elevation
May displace flap margin to new location
Steps in Open Flap Debridement
Horizontal incisions being made to bone within the sulcus or pocket base
Elevation of full-thickness flap to expose tooth roots and alveolar bone
Periodontal instrumentation of tooth roots
Types of Periodontal Surgery: Osseous Resective Surgery
Corrects deformities of the alveolar bone resulting from advanced periodontitis
Main goal---to eliminate periodontal pockets
Ostectomy---removal of the alveolar bone attached to the tooth
Osteoplasty---reshaping the alveolar bone without removing the supporting bone
Contraindicated in patients with severe periodontitis- may further compromise the support around the tooth
Boney Defects are…
harder to fix
Boney Defects Classification:
1 wall defect- 3 walls missing w/ 1 wall remaining
2 wall defect- 2 walls missing
3 wall defect- 1 wall missing w/ 3 walls remaining
This is the best one to have due it is the least damaged and easiest to fix!!
Types of Periodontal Surgery:Apically Positioned Flap w/ Osseous Resective Surgery
Combines displaced flap in the apical direction with the resective osseous surgery
Gingival margin apical to CEJ
Increased root exposure
Reduced pocket depths
Expect reasonable patient self-care and professional periodontal maintenance
to purposefully remove gingiva to create a reduced pocket depth
Steps in Apically Positioned Flap w/ Osseous Resective Surgery:
Internal Bevel incision and vertical releasing incision
Removal of collar of soft tissue following flap elevation
ostectomy
Inspection of final bone contours after ostectomy and osteoplasty
Suturing
Note that the flap margin is displaced in an apical position compared to its original position
Placement of periodontal dressing to stabilize the flap at its new position
Special Considerations for the Dental Hygienist:
During surgery, it is common for the gingival margin to be positioned against the teeth in a more apical position than is originally occupied
This exposes a portion of the root to the oral cavity
Exposure of a portion of the root may be an esthetic concern for the patient
Exposure of a portion of the root can lead to root caries
Temporary dentinal sensitivity is a frequent postsurgical complaint
Before surgery, the patient should be informed about anticipated changes in appearance and the potential for dentinal sensitivity