HP 252 Exam
0.0(0)
Card Sorting
1/48
Earn XP
Description and Tags
Study Analytics
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
49 Terms
1
New cards
autism definition
Refers to a range of conditions characterized by challenges with social skills, repetitive behaviors, speech and non-verbal communication as well as unique strengths and differences
2
New cards
Autism DSM-5
o Impairments in Social Communication and Social interaction like social emotional reciprocity, nonverbal communicative behaviors used for social interaction
o Restricted, repetitive patterns of behaviors, interests or activities
o Restricted, repetitive patterns of behaviors, interests or activities
3
New cards
Incidence, prevalence and risk factors of autism
Present in early childhood, limit or impair everyday functioning, inherited genetics and older parental age, 1-2% prevalence
4
New cards
Other early signs of autism in young children
Unusually strong interest in their toys but do not engage with people during play, no response to name, and enjoy being tickled but don't look at their mom to show enjoyment
5
New cards
Understanding of the term ‘neurodiversity’
“Difficulties in interactions occur because of different ways
of experiencing the world and processing information
(Davis & Crompton ‘21).”
● Diversity of the human mind
● Variation in neurocognitive functioning (Walker ‘14)
of experiencing the world and processing information
(Davis & Crompton ‘21).”
● Diversity of the human mind
● Variation in neurocognitive functioning (Walker ‘14)
6
New cards
Describe the difference between person-first and identity-first language
Person first language emphasizes the person before the disability, for example “person who is blind." Identity first language puts the disability first in the description, e.g., “disabled” or “autistic."
7
New cards
Differences between the medical model and social model approaches
Medical Model
-The person is disabled by the abnormalities and deficits of their own body and/or brain
- Disabled people are broken, abnormal, or damaged versions of human being and should be fixed, cured, and/or prevented
Social Model
- Person is disabled by their environment and its physical, attitudinal, communication, and social barriers
- Disabled people are normal valid varieties of human being
-The person is disabled by the abnormalities and deficits of their own body and/or brain
- Disabled people are broken, abnormal, or damaged versions of human being and should be fixed, cured, and/or prevented
Social Model
- Person is disabled by their environment and its physical, attitudinal, communication, and social barriers
- Disabled people are normal valid varieties of human being
8
New cards
Communication profiles of women with ASD
● Not a homogeneous group
● Manifests differently in males versus females
● Often later diagnosis
● Less restricted and repetitive interests
● Higher social motivation and capacity for friendship
● Tend to internalize emotions (leads to negative
outcomes)
● Manifests differently in males versus females
● Often later diagnosis
● Less restricted and repetitive interests
● Higher social motivation and capacity for friendship
● Tend to internalize emotions (leads to negative
outcomes)
9
New cards
The new framework for working from a neurodiversity perspective
1. The neurotypical communicative style is not the goal
2. Understanding the ND individual’s own communication style is important
3. NT and ASD communication styles are just different. One is not better than the other
2. Understanding the ND individual’s own communication style is important
3. NT and ASD communication styles are just different. One is not better than the other
10
New cards
Motor development in middle childhood
Gross Motor: Smoother, more coordinated.
Fine Motor: Improved, fine-tuned
Hands used as Tools: Hammering, pasting, tying shoes, and fastening clothes
Fine Motor: Improved, fine-tuned
Hands used as Tools: Hammering, pasting, tying shoes, and fastening clothes
11
New cards
Early signs of autism
- No babbling by 12 months of age
• No use of gestures by 12 months of age
• Doesn’t say single words by 16 months
• Doesn’t say two-word phrases by 24 months
• Loses language or social skills
• No use of gestures by 12 months of age
• Doesn’t say single words by 16 months
• Doesn’t say two-word phrases by 24 months
• Loses language or social skills
12
New cards
Social and emotional development
Increased ability to understand complex emotions, understanding of multiple emotions in single situation, ability to suppress or conceal negative emotional reactions, use of self-initiated strategies for redirecting feelings
13
New cards
Dodge’s Social Processing Model
Encode social cues, interpret social cues, search for response, select an optimal response, enact appropriate response
14
New cards
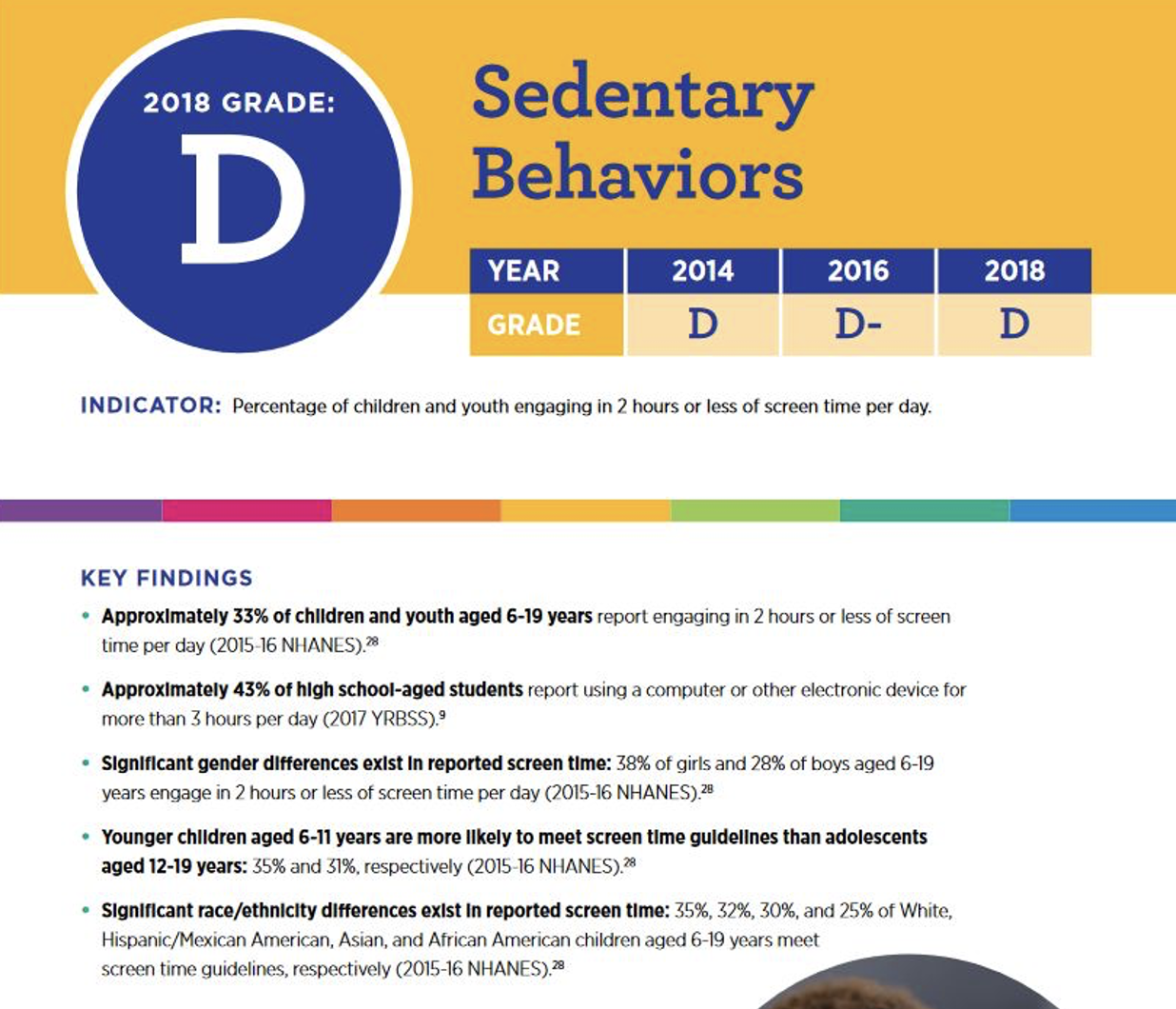
Obesity in children (Prevalence, health implications, influence of diet and exercise factors)
18.5 % of children 6-19 are obese
Risk of heart disease and high cholesterol, some forms of cancer, social consequences, type 2 diabetes
Socio-economic and cultural factors (ie cup-noodles are more cost effective than an apple and are more filling) -> access to education regarding healthy eating
62% of children ages 9-13 do not participate in any organized physical activity in non-school hours, 23% do not engage in any free-time physical activity
Risk of heart disease and high cholesterol, some forms of cancer, social consequences, type 2 diabetes
Socio-economic and cultural factors (ie cup-noodles are more cost effective than an apple and are more filling) -> access to education regarding healthy eating
62% of children ages 9-13 do not participate in any organized physical activity in non-school hours, 23% do not engage in any free-time physical activity
15
New cards
New roles and experiences child have when transitioning to elementary school
New relationships, new reference groups, and new standards for judging themselves. Emerging concern: New evidence that early schooling proceeds mainly on the basis of negative feedback. Vygotsyky: ZPD with scaffolding.
16
New cards
Common impairments/conditions of children with disabilities
10% of all children in the U.S. receive special education, and of these kids 50% learning disability, 21% speech or language impairments,12% intellectual disability and 9% serious emotional disturbance.
Learning disabilities: Are of normal intelligence or above but have difficulties in at least one academic area and usually several. ADHD is considered a learning disability in the school context.
Learning disabilities: Are of normal intelligence or above but have difficulties in at least one academic area and usually several. ADHD is considered a learning disability in the school context.
17
New cards
Educational issues: The IEP & LRE
IDEA spells out broad mandates for services to all children with disabilities.
IEP (individualized education plan): A written statement that spells out a program specifically tailored for the student with a disability. Should be related to a child's learning capacity.
LRE (least restrictive environment): IDEA mandates that a child with a disability must be educated in a setting as similar as possible to that of child without disability -> inclusion, mainstreaming, integration
IEP (individualized education plan): A written statement that spells out a program specifically tailored for the student with a disability. Should be related to a child's learning capacity.
LRE (least restrictive environment): IDEA mandates that a child with a disability must be educated in a setting as similar as possible to that of child without disability -> inclusion, mainstreaming, integration
18
New cards
The cognitive and social demands/experiences in the elementary school years
Children need to know what scripts to follow to get other children to be their friends, peer relations.
19
New cards
Definition and understanding of executive functions
In early childhood, executive function especially involves advances in cognitive inhibition, cognitive flexibility, and goal-setting.
Self-control/inhibition, working memory, flexibility in thinking strategies
Self-control/inhibition, working memory, flexibility in thinking strategies
20
New cards
Impact of executive function differences for children
- EF skills predict academic success
- Children w weak EF skills are at high risk for dropping out of school
- Children with weak EF skills are at high risk for social/behavioral problems
- Children w weak EF skills are at high risk for dropping out of school
- Children with weak EF skills are at high risk for social/behavioral problems
21
New cards
Inhibition
Inhibition: The ability to stop an automatic impulse
Fundamental to: Regulating attention, social adaptation, effective learning
Fundamental to: Regulating attention, social adaptation, effective learning
22
New cards
Self-regulation
Ability to implement executive functions when you need them
23
New cards
Attention regulation
- Choose the focus of attention
- Keep paying attention until the task is done
- Only pay attention to what is important
- Stop paying attention and focus on something else
- Keep paying attention until the task is done
- Only pay attention to what is important
- Stop paying attention and focus on something else
24
New cards
Working memory
Holding information in mind while performing a mental task
25
New cards
Planning
- Planning skills become increasingly
important throughout elementary school
- Planning relies heavily on the interaction
between working memory and inhibition
important throughout elementary school
- Planning relies heavily on the interaction
between working memory and inhibition
26
New cards
Cognitive flexibility
The ability to adapt our behaviour and thinking in response to the environment. IE: games like uno, connect four
27
New cards
Definition and main signs of ADHD (attention deficit hyperactivity disorder)
May or may not be comorbid with a specific learning disability
A disability in which children consistently show one or more of the following characteristics: (1) inattention, (2) hyperactivity, and (3) impulsivity.
A disability in which children consistently show one or more of the following characteristics: (1) inattention, (2) hyperactivity, and (3) impulsivity.
28
New cards
Signs of inattention and impulsivity/hyperactivity
Inattention:
- Often fails to give close attention to details/ makes careless mistakes
- Is often easily distracted
- Is often forgetful in daily activities
- Often does not seem to listen when spoken to directly
Impulsivity/hyperactivity:
- Often fidgets with or taps hands or feet, or squirms
- Often talks excessively
- Often has trouble waiting their turn
- Often fails to give close attention to details/ makes careless mistakes
- Is often easily distracted
- Is often forgetful in daily activities
- Often does not seem to listen when spoken to directly
Impulsivity/hyperactivity:
- Often fidgets with or taps hands or feet, or squirms
- Often talks excessively
- Often has trouble waiting their turn
29
New cards
Supports and interventions for children with SLD and ADHD
The right educational approaches, the right strategies for learners, and context management
Educational approaches (SLD), medical management (ADHD), metacognitive strategies, context management
Educational approaches (SLD), medical management (ADHD), metacognitive strategies, context management
30
New cards
Puberty (Physical changes, brain development, timing)
Brain-neuroendocrine process
• Important marker of beginning of adolescence
• Ends before adolescence does
Levels of neurotransmitters increase
• Dopamine
Prefrontal cortex only finishes maturing at 18-25 years
• Reasoning, decision making, self-control
Adolescent experiences could also stimulate brain changes
• Not just all biological maturation
• Important marker of beginning of adolescence
• Ends before adolescence does
Levels of neurotransmitters increase
• Dopamine
Prefrontal cortex only finishes maturing at 18-25 years
• Reasoning, decision making, self-control
Adolescent experiences could also stimulate brain changes
• Not just all biological maturation
31
New cards
Physical and environmental factors influencing adolescent sleep behaviors
Delayed release of melatonin in older adolescents. Influence of screen time, caffeine, adjusted school start time
32
New cards
Leading causes of death in adolescents
1) Unintentional injuries
• Almost half of deaths
• Motor vehicle accidents
2) Suicide
3) Homicide
• Almost half of deaths
• Motor vehicle accidents
2) Suicide
3) Homicide
33
New cards
Current patterns in substance use/abuse in adolescents
• General decline in drug and alcohol use in past 50
years, including smoking (some replaced by ecigarettes)
- 30% of seniors said they’d been in vehicle with
driver under the influence of drugs or alcohol
in past two weeks
years, including smoking (some replaced by ecigarettes)
- 30% of seniors said they’d been in vehicle with
driver under the influence of drugs or alcohol
in past two weeks
34
New cards
Adolescent egocentrism (Definition and components)
The heightened self- consciousness of adolescents.
35
New cards
Application to current/relevant contexts
Adolescents’ belief that others are as interested in them as they themselves are, as well as attention-getting behavior motivated by a desire to be noticed, visible, and “on stage.”
Frequent use of social media, such as Facebook may increase adolescents’ egocentrism
Frequent use of social media, such as Facebook may increase adolescents’ egocentrism
36
New cards
Describe aspects of social development relating to family and friend relationships
• Parenting (Access/restriction to social media, parent access to child’s information/accounts, gender and cultural differences regarding autonomy)
• Parent-adolescent conflict: May serve positive developmental function
• Sibling relationships: Predicts relationship later in life
• Quality of friendship matters
• Peer groups and identity
• Changes in social media usage (Nesi et al., 2018)
• More frequent and immediate experience
• Amplifies experiences and demands (feedback
seeking, expectations for friendship maintenance
and access)
• Alters qualitative aspects of relationship
• Can change who the relationship is with
(geographical distance)
• New behaviors – ratings, public feedback
• Parent-adolescent conflict: May serve positive developmental function
• Sibling relationships: Predicts relationship later in life
• Quality of friendship matters
• Peer groups and identity
• Changes in social media usage (Nesi et al., 2018)
• More frequent and immediate experience
• Amplifies experiences and demands (feedback
seeking, expectations for friendship maintenance
and access)
• Alters qualitative aspects of relationship
• Can change who the relationship is with
(geographical distance)
• New behaviors – ratings, public feedback
37
New cards
Positive Youth Development Programs and what they aim to do
Focus on positive outcomes
• Pro-active
• All youth
• Youth as active participants
• Community response (systemic change)
• Community members
• Pro-active
• All youth
• Youth as active participants
• Community response (systemic change)
• Community members
38
New cards
Difference between sexual orientation and gender identity
Sexual orientation refers to who we are attracted to while gender identity refers to who we are
39
New cards
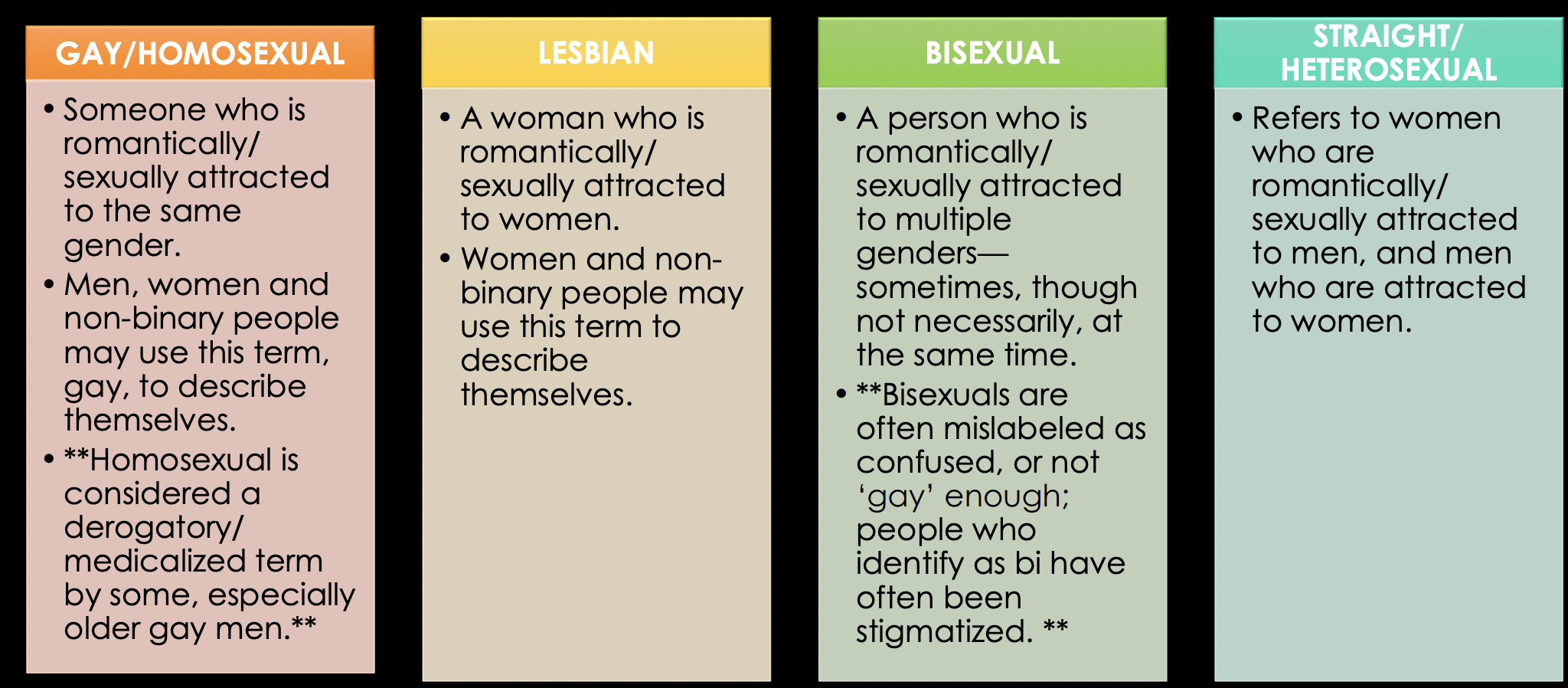
Understanding of sexual orientation terms: gay/homosexual, lesbian, bisexual, straight/heterosexual, queer, pansexual, asexual, questioning
see image
40
New cards
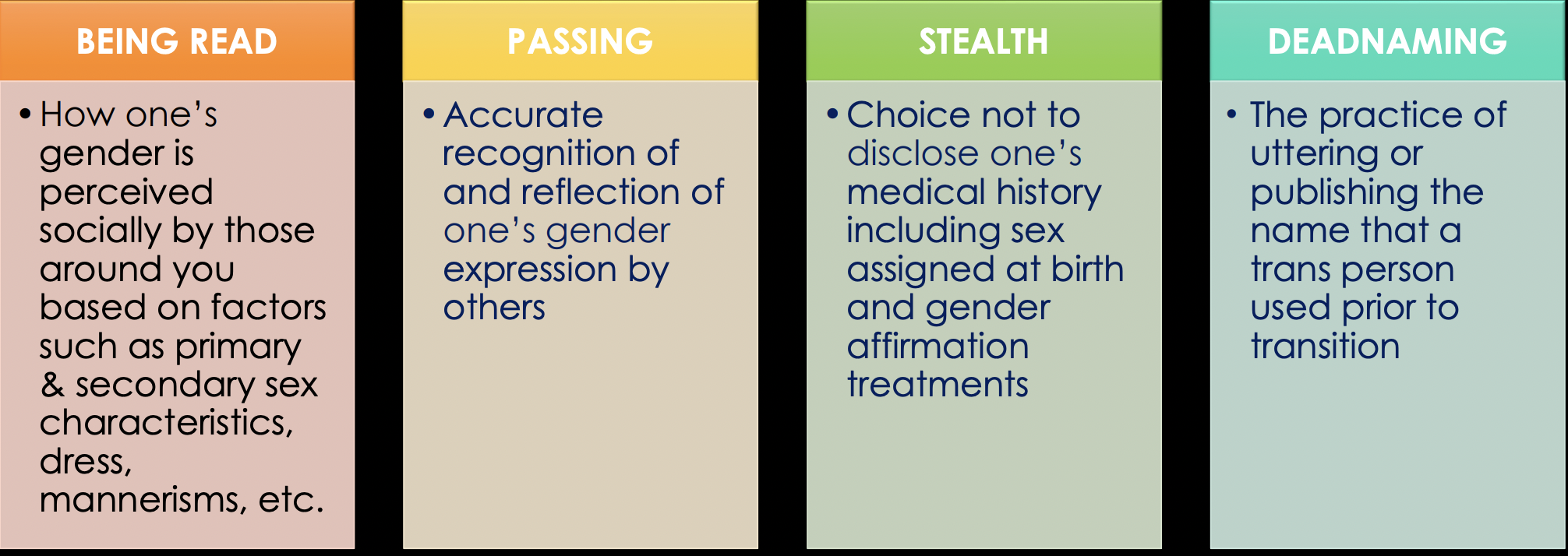
Understanding of gender diversity and trans* terms: transgender, gender nonconforming, cisgender, being read, passing, stealth, deadnaming
see image
41
New cards
Impact of misgendering on individuals’ health and their healthcare experiences
Misgendering can lead to decreased self-esteem, heightened anxiety and depression.
42
New cards
Examples of Anti-Trans Legislation and how these impact transgender youth
Medical:
• Limit or ban gender affirming care for TGD youth
• Penalize or even criminalize gender affirming care
Sports:
• Bans trans girls/women from sports
• “Fairness in women’s sports”
- Usually don’t address trans masculine individuals
• Limit or ban gender affirming care for TGD youth
• Penalize or even criminalize gender affirming care
Sports:
• Bans trans girls/women from sports
• “Fairness in women’s sports”
- Usually don’t address trans masculine individuals
43
New cards
Health and social impacts of non-affirmation for transgender youth
Suicidality, attempt and self-harm, as well as EDs and substance abuse disorders.
- Substance use disorders & tobacco use
• Unprotected sex and rates of HIV transmission
• Homelessness, placement in foster care system
• Involvement in juvenile justice system
- Substance use disorders & tobacco use
• Unprotected sex and rates of HIV transmission
• Homelessness, placement in foster care system
• Involvement in juvenile justice system
44
New cards
Stages and age ranges of adolescence
Early adolescence (10-13), Middle adolescence (14-17), Late adolescence (17-21), Emergent adult (18-25)
45
New cards
Normal changes, perceptions, experiences in adolescence
What's normal? Preoccupation with self, mood swings, body image insecurity, parental conflict, conformity with peer values, impulse control problems, experimentation with drugs and delinquency
46
New cards
Understanding of the types of teen dating violence
Physical violence, sexual violence, psychological aggression, stalking
47
New cards
Consequences of unhealthy, abusive, or violent relationships
Lead to depression and anxiety, use of drugs and alcohol, thoughts of suicide, exhibit antisocial behaviours. Youth who are victims of dating violence in high school are more likely to be victimized in college too
48
New cards
Risk and protective factors for teen dating violence perpetration
Individual (risk): Low self-esteem, Low education or income, Young age, Aggressive or delinquent behavior as a youth, Heavy alcohol and drug use
Individual (protective): Awareness of community services for TDV, Use of conflict management skills, Attending religious services, Grade point average, Employment
Individual (protective): Awareness of community services for TDV, Use of conflict management skills, Attending religious services, Grade point average, Employment
49
New cards
Components of the public health approach
Define the problem, Surveillance, Identify risk and protective factors, develop and test prevention strategies, assure widespread adoption