BIOL 232: Respiratory Infection
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
transmission of respiratory infections
droplet, airborne, contact
droplet respiratory infections
- over 5 microns
- influenca, S. pneumonia
- surgical mask and eye protection
airborne respiratory infections
- less then 5 microns
- TB, measles
- N95, negative pressure room
ways to classify respiratory symptoms
location (URTI, LRTI) and time
what does the epiglottis do
serves as the divider between the two regions
URTI
- affects nose, pharynx, sinuses, +/- conjunctiva or ear mucosa
- most URTI are viral so they DO NOT require antibiotics
- self limiting
MRTI
- epiglottis is the only structure
- division between upper and lower
LRTI affects?
trachea, bronchioles, bronchi, alveoli
URTI includes
- rhinitis, pharyngitis, tonsilitis, sinusitis, laryngitis
- Common cold viruses such as = adenovirus, coronavirus, RSV
common s/s URTI
- runny nose
- sore throat
- sneezing
- mild cough
LRTI involve
- deeper lung structures
- trachea, bronchi, bronchioles, alveoli
most important LRTI
- pneumonia = infection and inflammation of the lung parenchyma (alveoli)
- air sacs fill with pus and liquid
- productive cough + focal indicate bacterial pneumonia
Pneumonia clinical prevalance
typical = bacterial
atypical = viral, fungi
Pneumonia anatomical classifications (areas affected)
bronchopneumonia = more viral
lobar = more commonly seen in bacterial
interstitial = more commonly seen in viral like influenza
Pneumonia location
- CAP (community acquired pneumonia) = non hospitalized or more than 48 hours after hospitalization
- HAP (hospital acquired pneumonia) = presents less than 48 hours after hospitalization
- VAP (ventilator associated pneumonia) = presents less than 48 hurs after endotracheal intubation
- Aspiration pneumonia = from aspiration of colonized URTI or GI secretions
Pneumonia pathogens
- bacterial
- viral
- fungal/opportunistic
- chemical
Pneumonia s/s
- early cases = productive cough/ acute changes, high fever, changes in xrays
- geri might only show LOC as the immune system is not able to trigger fever and there nervous system is not adequate to trigger cough reflex
dx of CAP in adults without immunocompromising conditions
1st = newly recognized pulmonary infiltrates on chest imaging
2nd = one resp symtoms (new or worsening cough or sputum production, dyspnea, chest pain)
3rd = at least one symtom/findings (abnormal lung sounds, fever, leukocytosis or unexplained bandemia, hypoxia)
common organisms in Pneumonia (bacterial, viral, nosocomial)
Streptococcus pneumoniae (typical)
GAS (atypical bacteria)
- Mycoplasma pneumoniae
- Chlamydophila pneumoniae
- Legionella pneumophila
Viral
- Influenza
- Adenovirus
Nosocomial
- Pseudomonas aeruginosa
- S. aureus (including MRSA)
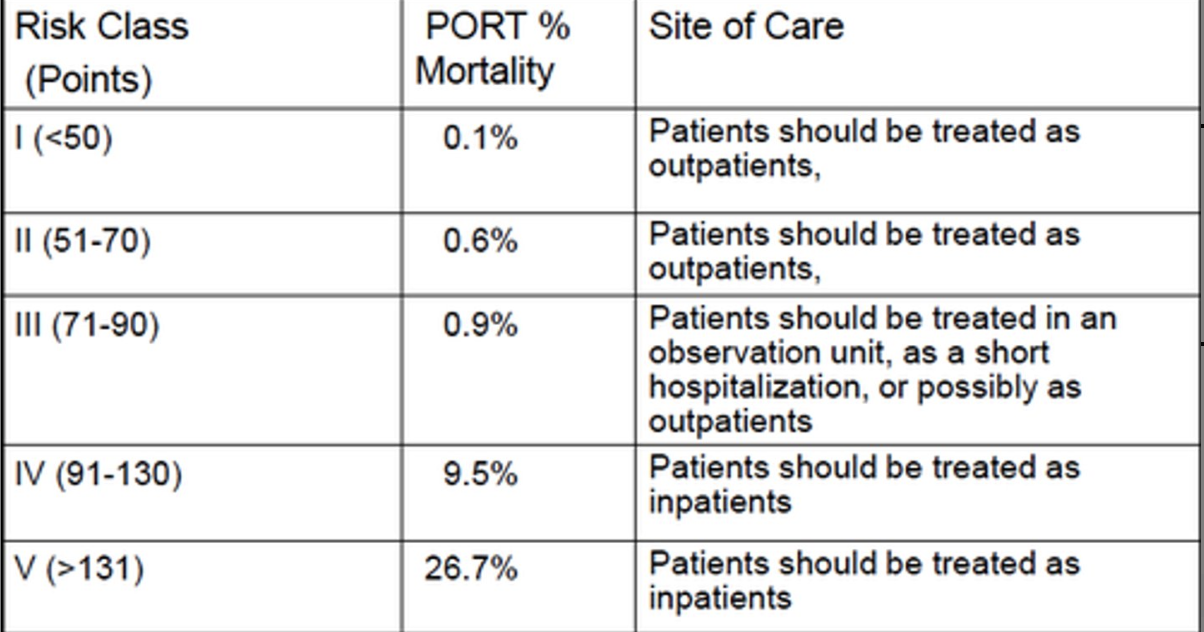
Which class of pneumonia pts need to be hospitalized
Class IV and V (medium to high risk)
3 main mechanisms by which bacteria reach the lungs
- aspiration
- inhalation
- hematogenous spread
common s/s of LRTI
- productive cough
- dyspnea
- pleuritic chest pain
- focal lung findings
- lung infiltration on CXR
cause of infectious sinusitis
- acute infectious rhinitis/sinusitis is usually caused by viral organisms
- common cold viruses and influenza
3 cardinal signs of infectious rhinitis
- for 10 days or longer
- clear to mucopurulent nasal discharge
- nasal obstruction/congestion
- headache (facial pressure)
fever is 50% sensitive and specific = dont need to cosnider that much (do consider how high the fever is, with a cold it should be low grade, but if bacterial infection it should be high grade)
how to know if infectious rhinitis is caused by bacteria
- s/s with no improvement after 10 days
- double sickening (pt initially improves but then develops worsening symptoms several days later = indicates a secondary bacterial infection)
- high fever
- foul smelling nasal discharge
common cold with infectious rhinitis
- gradual onset and mild s/s (depends on the viral tropism for URTI)
- runny nose
- fever not common/low grade
- sneezing
- dysphagia
- mild cough
- stuffy nose, sore throat
- headache is rare/mild
flu with infectious rhinitis
- sudden onset of systemic symtoms
- fever, chills, fatigue, weakness
- aches
- headache is common
- influenzas virus is the only cause of the flu
- rapid progression and abrupt (short incubation period)
infectious pharyngitis microorganisms are
viral or bacterial
viral infectious pharyngitis
- most common etiologic agent is viruses in adults and kids (50-80%)
bacterial infectious pharyngitis
- more common in children
- most common causative organism is group A streptococci aka streptococcus pyogenes = strep throat
viral vs bacterial respiratory infections
viral: diffuse spread, non-productive cough, mild fever, gradual symptoms
bacterial: localized spread, productive cough, high fever, severe symptoms
pharyngitis evaluation/ dx tools
- WBC is not very useful
- RADT is specific for group A beta-hemolytic streptococci
- throat swab = more sensitive
RADT
- fast and cheap
- detect viral bacterial proteins (antigens expressed on the surface of the bacteria)
- if positive can be trusted
- if negative cannot be trusted (false negatives), do throat culture
throat culture
- sensitive
- used if RADT is negative to confirm negative result
streptococci sequelae
- Untreated strep throat can lead to serious complications
- Scarlet fever, acute rheumatic fever
scarlet fever
Rash, strawberry tongue
rheumatic fever
- 4-9 year of age (2-3 weeks after)
- High fever
- Higher risk for developing endocarditis later
- Affected organs: heart valves, joints, skin, nervous system
- Untreated strep leads to rheumatic heart disease
- Antibodies against streptococcus cross-react with host cells in an autoimmune reaction, resulting in serious sequalae (attack our own tissues)
tx for bacterial pharyngitis
- 6-10 day course of oral amoxicillin
tx for viral pharyngitis
- antiviral therapy within 48 hours
- oseltamivir or zanamivir
- vaccination
whooping cough causative organism
Gram negative bacillus Bordetella pertussis
whooping cough characteristics
- Airborne droplets transmission
- Incubation period of 7-21 days
- Progressive phases
LRTI main infections
CROUP and pneumonia
CROUP infects
Infects the larynx - the trachea and even bronchi = laryngotracheobronchitis (LBT)
CROUP main target populations
children 6 months - 5 years
s/s of CROUP
- Barking or seal cough (laryngitis), caused by inflammation of larynx or trachea
organisms responsible for CROUP
Parainfluenza viruses types 1 and 2
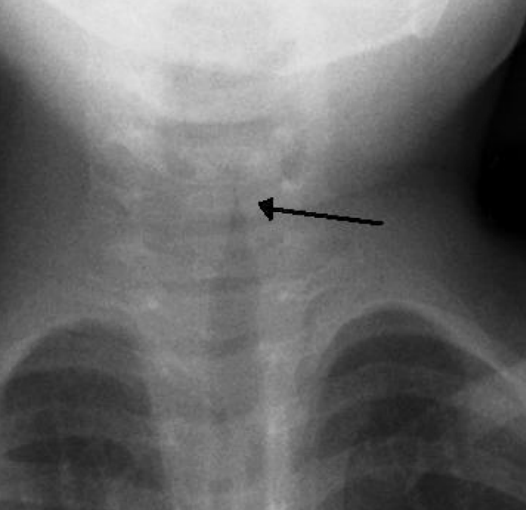
dx of CROUP
- neck/chest xray for steeple sign (narrowing of the airway)
- tx is symptomatic and it should be carefully selected to avoid airway obstruction
- when this is present, we can start seeing the STEEPLE sign in x-rays (narrowing of the airway)
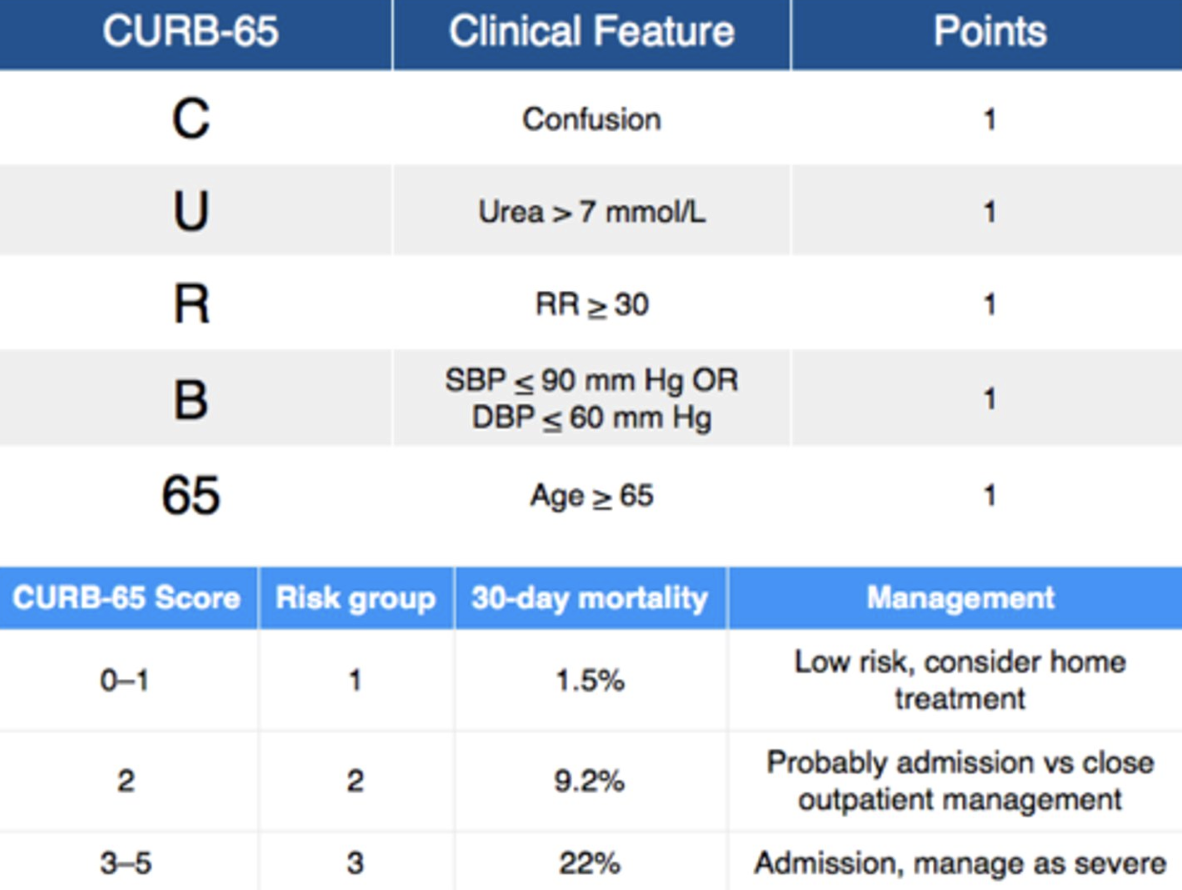
Curb 65 Score - Pneumonia Clinical Prediction Tool
More sensitive for treatment decisions and mortality risk prediction