Module 6 - Part 1 Vitamins, minerals + sport performance
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
73 Terms
**What are Vitamins?
Organic compounds/catalysts involved in metabolic reactions
*********WHERE are Vitamins obtained?
MUST be obtained from DIET except for 2
*******What are the 2 vitamins that we cannot obtain from the diet?
VIT D = synthesized from sunlight
VIT K = Synthesized by GUT BACTERIA
******Several Vitamins are in what form? give an example
Precursor or Provitamin form in foods + have to be converted to the active form
eg. beta-carotene
Are there any difference in Athlete vs. Non-athlete vitamin intake?
NO
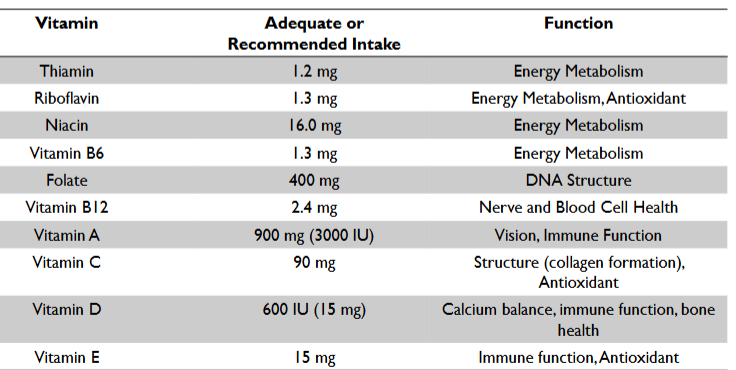
***Vitamins: FUNCTION + REQUIREMENTS (athlete)
*******MINERAL: Macro (major) vs. Micromineral (trace)
WHAT is the difference that categorizes a mineral as macro vs. micro?
INTAKE req.
Macro = >100 mg or >0.01% body wt
Micro = <100 mg or <0.01% body wt
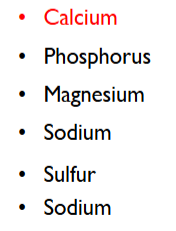
*****What are the Macrominerals + which is VERY important for athletes?
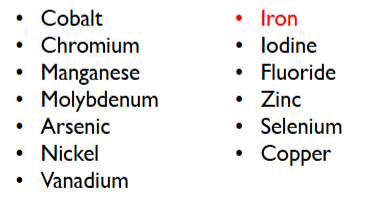
*****What are the Microminerals + which is VERY important for athletes?
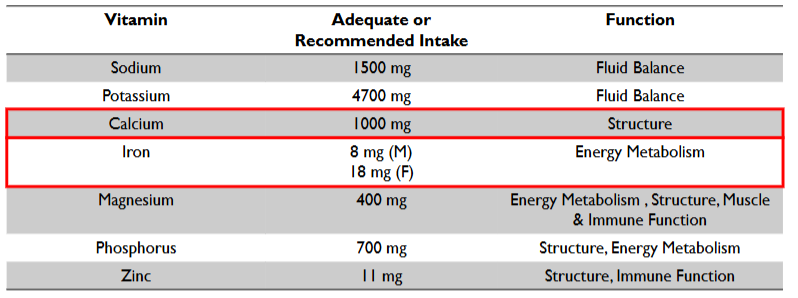
******Minerals: Function + AI requirements (Athletes)
CALCIUM
Macro = CALCIUM = 1000 mg (AI)
function → Structure
******Minerals: Function + requirements (Athletes)
IRON: Req for F vs. M + functions
Micro = IRON
8 mg M
18 mg F
Function → Energy metabolism
******Minerals: Function + requirements (Athletes)
Others; not highlighted as very important in lecture slides
*****Are Current recommendations for micronutrient intakes for the general population adequate for athletes?
YES
******Do athletes need micronutrient supplements?
NO
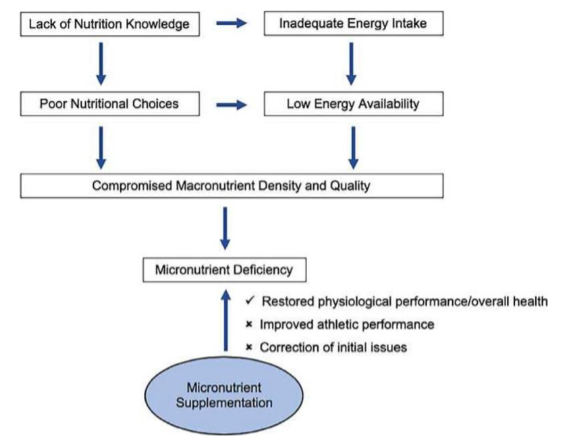
It is the joint position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine, that micronutrient supplements are unnecessary for athletes who consume a diet providing high energy availability (EA) from a variety of nutrient-dense foods.
supplements is only needed for athletes who consume suboptimal amounts of micronutrients
If we ensure that an athlete has adequate EA, it is likely that they will also have adequate micronutrient status
Low EA has been lined to micronutrient deficiencies in athletes when it does occur
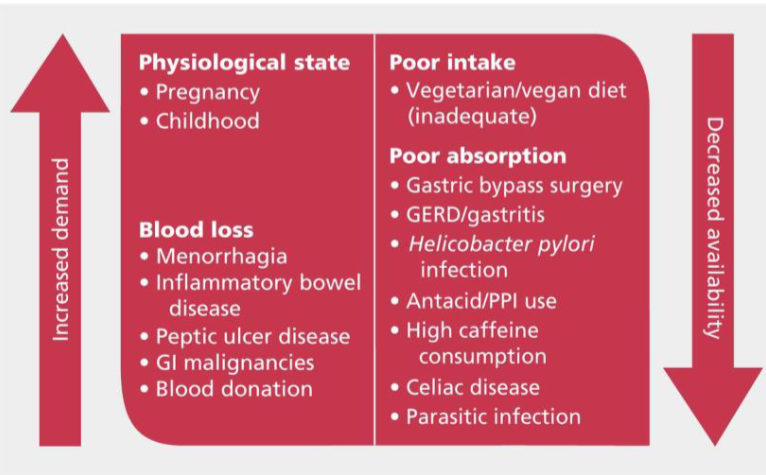
How do cases where supplement of micronutrients is needed occur
what causes micronutrient deficiencies?
*****What is an exception to the generalized observation that: Athletes who have Adequate E intake PLUS a diet that provides a variety of foods are unlikely to suffer from micronutrient deficiencies?
Iron deficiency in female athletes
What are reasons why Achieving adequate E intake = critical for athletes?
Sport performance + general health + well being
Athletes with LEA = create a secondary risk for micronutrient deficiency because they are not consuming the amounts and diversity of foods needed to meet the otherwise manageable req. for vit + minerals
********Does EXCEEDING the AI for any Micronutrient result in performance?
NO
there is NO EVIDENCE to show that exceeding AI for any micronutrient results in gains unless they were deficient to begin with
******What is the relationship between blood + sport performance?
ATP (metabolic production of energy) need O2
RBC: deliver O2 to working muscle + carry CO2 back to lungs
O2 carrying capacity of blood is proportional to the [Hb] in RBC
Athletes need to have adequate RBC AND Hb within each RBC
******What is the relationship between Micronutrients and blood + sport performance?
Micronutrients are co-factors for the enzymes responsible for Hb synthesis or RBC formation
*******What are the 4 micronutrients that are co-factors in Hb + RBC synthesis?
Iron
Copper
Folate
Vit B12
******Which of the 4 RBC/Hb co-factors are likely to be low in young people?
Iron
******Which of the 4 RBC/Hb co-factors are likely to be low in old people? WHY?
Vit B12
Decreased function of Intrinsic factor needed for absorption
********What is the role of IRON in terms of Blood + sport performance?
what is it required for
Required for Hb + Myoglobin production
*****What is Heme
Heme = Iron containing molecule at the center of each Hb unit binds O2 + CO2 reversibly
*****What is Myoglobin
= an Iron + O2 binding protein found in Muscle tissue
acts as a STORAGE VESSEL for O2 as it hold O2 inside cardiac + skeletal muscle
******Is Myoglobin found in the bloodstream?
NO
Only found in blood when released following muscle injury = Abnormal finding
******What are the 2 forms that dietary iron in food comes in?
Heme
Non-heme
*******Compare heme vs. non-heme iron
Difference
What foods are they each found in?
HEME = better absorbed
found in meat, fish + poultry
NON-heme = less well absorbed
found in plant proteins, fruits, eggs, milk + grains
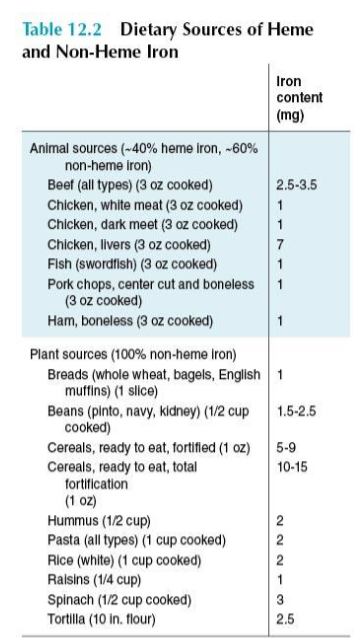
******What are some good sources of Dietary Heme + Non-heme iron
HEME = Red meats + livers
Non-heme = Fortified cereals + spinach + beans
******What are some factors that INCREASE Iron absorption
Nutrition factors or physiological
Heme iron in diet = increase absorption of non-heme
Increased demands in body: Pregnancy, low iron stores, high altitudes, high blood loss, high exercise training
Vit C in mean = increases non-heme absorption
High gastric acid production (low stomach pH)
******What are some factors that DECREASE Iron absorption
Nutrition factors or physiological
Good iron status = decrease demands
Factors in meals eg. phytates + polyphenols (coffee + tea), oxalic acids, fiber + soy
Mineral-mineral interactions eg. CALCIUM compete for transfer
high antacid use = Increase pH (less acidic stomach) + mineral interactions
*******RDA for Iron:
Adult men
Pre-menopausal women
Post-menopausal women
Adult men = 8 mg
Pre-menopausal women = 18 mg
Post-menopausal women = 8 mg
People treated for iron deficiency may require intakes far above the RDA to replete their stores
******How do IRON RDA for Athletes compare to non-athletes?
The exact iron requirements for athletes and athlete sub-groups are currently unknown. They are believed to be higher than in the general population.
***********What is Hepcidin?
Hormone that regulates iron metabolism in the gut + macrophages
major regulator in the body
***********Where is Hepcidin synthesized?
In the LIVER
***********HOW does Hepcidin affect iron metabolism?
By degrading transporter FERROPORTIN (Fpn) located on the brush border membrane of duodenal enterocytes
degradation of Fpn transporters can results in DECREASED dietary IRON ABSORPTION from small intestine
*******What is the impact of physical activity on Hepcidin?
Intense physical activity upregulates Hepcidin
it is thought that this activity-driven upregulation of hepcidin decreases iron absorption, increases iron, needs + presents an additional risk for anemia
*********What are the 5 key measures taken when measuring IRON status?
Ferritin
Transferrin saturation
Total Iron binding capacity (TIBC)
Hemoglobin
Hematocrit
*********Of the 5 key measures taken when measuring IRON status, Which is the first to decrease (first sign of low iron)?
FERRITIN
******Ferritin measures vs. Iron status
What does it reflect
How do values change when iron status is low
Serum ferritin levels reflect tissue iron stores
decreases when iron status is low
FIRST THING TO DECREASE
******What does 1microgram/L of Ferritin = in terms of amount of Stored iron?
1microg/L ferritin = 8 mg stored iron
*****What is the function of Transferrin
Is a protein that carries iron to cells (transport)
******Transferrin measures vs. Iron status
What does it reflect
How do values change when iron status is low
Transferrin saturation is a measure of how much iron is bound + being actively carried by transferrin
Decreases when iron availability in blood is low and is a measure of iron status
******What is the normal % of Transferrin sat with Iron
What is the range?
30% = norm
Norm range = 16-50%
******TIBC (total iron binding capacity) measures vs. Iron status
What does it reflect/measure
How do values change when iron status is low
Measures total capacity for transferrin to bind + carry iron
Values INCREASE if iron status is low
******Hemoglobin measures vs. Iron status
What does Low values mean?
If Hb is low = iron shortages have been occurring for some time
******Hematocrit measures vs. Iron status
What does it reflect/measure
What do values mean
Measure of actual volume of RBC in the whole blood to total blood value
LOW Hematocrit = Fewer RBC = indicative of anemia
******Define Anemia
A GENERIC TERM for any condition in which Hb levels are low
******What are some causes of anemia?
Multiple causes (some diet some not)
*****What are some Clinical symptoms of Iron deficiency Anemia?
pallor
fatigue
loss of endurance capacity
reduction in strength
lowered immunity
Itchiness
“spoon” nails (Koilonychia)
decreased cognitive function
inability to regulate temp.
pica (odd cravings - i.e. Clay)
low hemoglobin, hematocrit and serum ferritin levels.
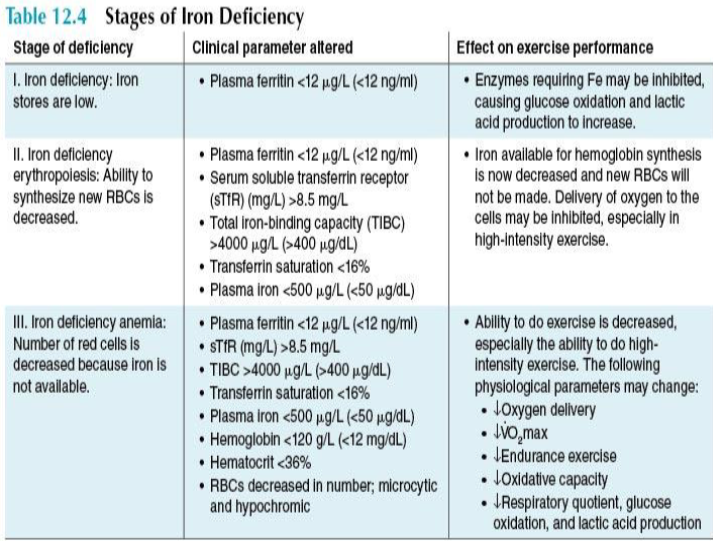
***********What are the 3 stages of IRON DEFICIENCY?
Which LAB VALUES are changed
what are the EFFECTS on performance
Iron deficiency: Iron stores are low = LOW FERRITIN (first sign) = glucose oxidation + increase lactic acid production
Iron deficiency Erythropoiesis: ability to synthesize new RBC = decrease => Low plasma FERRITIN, TIBC, TRANSFERRIN SAT, plasma IRON = Delivery of O2 inhibited
Iron deficiency Anemia: # of RBC decreased because iron not available => Low plasma FERRITIN, TIBC, TRANSFERRIN SAT, plasma IRON, HEMOBLOBIN, HEMTOCRIT, RBC low in number + small + pale in color = ability to exercise = decreased
******What is the PREVALENCE of iron deficiency anemia in athletes?
VERY COMMON concern for athletes
********Compare Iron deficiency anemia in athletes vs. general pop.
Compare percentages of General pop. vs. Athlete pop (M + F)
MUCH MORE PREVALENT IN ATHLETES
In the general population, the prevalence of iron-deficiency anemia among youth and adults is estimated at 2% to 5% in females and 1% to 2% in males.
▪ In athletes, iron deficiency affects:
▪ Iron Deficiency anemia is most common in female athletes (15–35%), but it is not an exclusively female health concern.
▪ 5–15% of the male athletes are also iron-deficient.
***Which type of sport has more prevalent Iron deficiency
give a %
Endurance 30-50% of athletes in endurance sports
**What % of Adolescent female athletes have iron deficiency anemia?
▪ Up to 52% of female adolescent athletes.
********What are 3 reasons why Athletes have ENHANCED IRON REQ.?
High physiological demands + requirements for iron associated with physical activity:
Hard training stim increase in RBC + blood vessels
Inadequate consumption of dietary iron
Low intake of cereal/grains + meats or very low E intake = make it hard to meet req.
High iron loss, mostly from blood loss
Injury, extreme events, FOOT STRIKE, heavy sweating
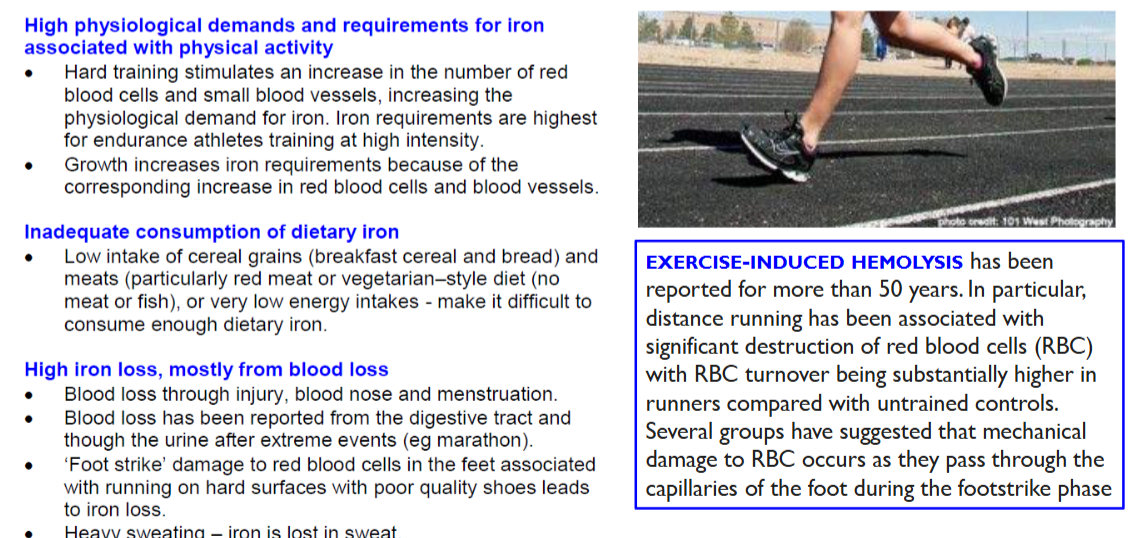
*******What is exercise induced Hemolysis?
HIGH IMPACT eg. heel strike = burst RBC in the capillaries of the foot during foot strike
common in distance runners
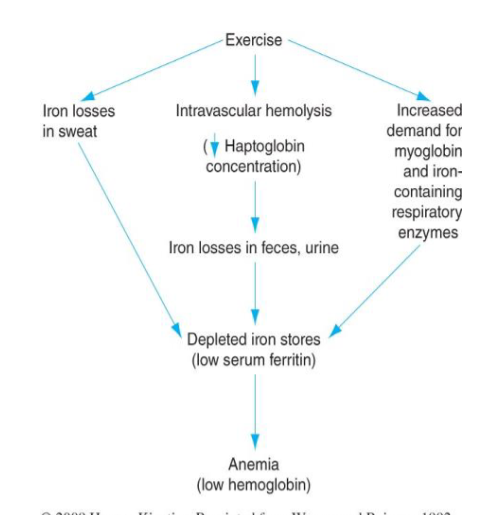
******What is the Possible mechanism for exercise induced iron deficiency?
What are 3 key factors that deplete iron stores?
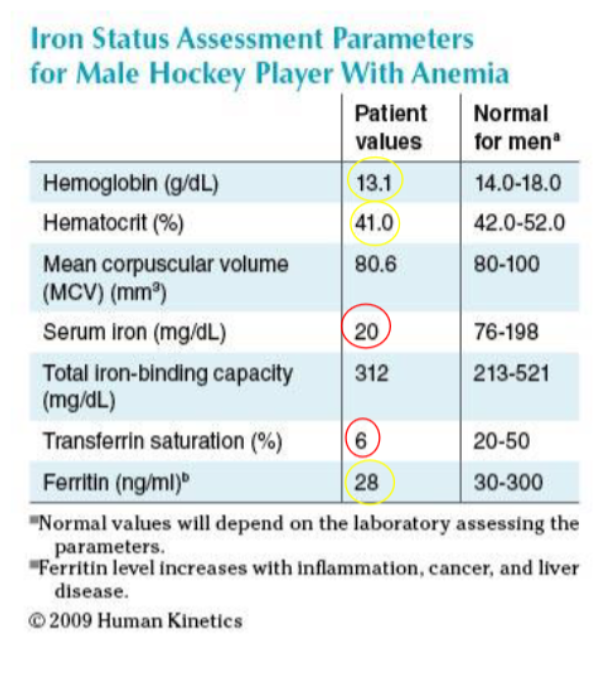
CASE study 1: 25 yr old minor hockey player with blood work suggestive of Fe-deficiency anemia. On Fe-therapy. No obvious sources of blood loss. Dark stools. Hx of abdominal cramping attributed to the Fe-therapy. Rectal exam indicates stools +ve for occult blood. This athlete was subsequently diagnosed with Crohn’s disease based on his medical hx and blood work.
based on his lab work + diagnosis what is the proposed intervention for Low iron? should you use supplements?
Treatment: Medical therapy for Crohn’s disease
Iron supplementation will play a relatively minimal role in this athlete’s overall recovery.
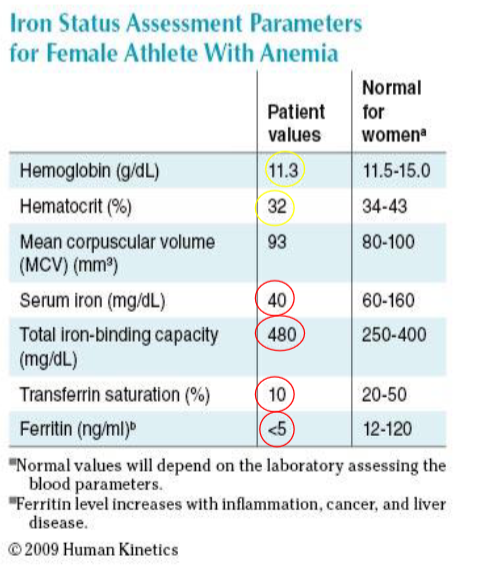
CASE STUDY 2: 21 yr old female athlete and personal trainer. Hx of fatigue and decreased ability to perform intense workouts. Body comp = 16.6% BF, BMI = 19.1 kg/m2. Iron intake = 10.9 mg/day. Avoids red meats. Menstrual cycles are normal. No associated blood or GI disorders. This athlete was diagnosed with iron deficiency secondary to poor dietary intakes.
based on her lab work + diagnosis what is the proposed intervention for Low iron?
Treatment: Dietary Therapy
▪ Increased dietary iron intake (food + supplemental Fe therapy)
▪ Reduction of training volume.
*****What are some things to keep in mind when giving treatments of anemia?
DETERMINE THE CAUSE!
Not all anemia is due to nutritional causes
Need to know if bleeding, disease or malnutrition is the primary cause.
Iron supplementation is not a cure-all for every type of anemia!
*****Iron Deficiency treatment: What amount of iron supplementation?
What are the guidelines for supplementation: when to take, what to take with, what not to take with
Iron Supplementation: 100-200 mg elemental iron per day
▪ Ferrous form of iron
▪ Taken on an empty stomach with full glass of water or fruit juice
▪ Taken in the morning or earlier in the day.
▪ Taken with a source of Vitamin C (e.g. fruit juice, oranges, tomatoes).
▪ Should not be taken with Calcium products (e.g. supplements, certain antacids, milk or milk products)
▪ Avoid high-oxalate foods (e.g., coffee, tea, spinach, kale, broccoli).
*****Iron Deficiency treatment: What steps to take after prescribing supplement?
What to check + when
how long to continue supplement
▪ Check iron stores 2-4 weeks post therapy for repletion.
If not replete, re-investigate cause.
▪ Check iron stores after 2-4 months to ensure ID doesn’t recur.
If ID recurs re-investigate and/or refer for further assessment.
▪ Continue with iron therapy for additional 4-6 months if Hb normal.
▪ Maintenance with a low dose of iron therapy may be required for patients with ongoing needs e.g., menses, dietary, growth spurts.
******What is Sports Anemia?
True form of anemia?
alternate names
CAUSES
NOT a true form of anemia
aka. “dilutional Pseudoanemia”
No response to Fe-therapy = NO markers of blood loss
CAUSES:
Blood volume expands in response to training + Hb production sometimes lags behind
****Sport anemia: Is expansion of blood volume expected with training
YES
Expansion of blood volume is an expected benefit of training.
▪ Blood volume expansion is a temporary effect of training.
▪ [Hb] may not be parallel to increase in BV
▪ Random blood draws, if taken at a time of BV expansion can mimic anemia BUT THIS IS
NOT THE CASE
▪ E.g. low Hb relative to blood volume
****Sport anemia: Is treatment needed?
NO (don’t give supplements)
◦ Given time the situation will normalize provided dietary iron intake is adequate.
Temporary and benign
▪ Will resolve after with adequate rest from training
▪ No adverse effect on athletic performance and possible beneficial effects
▪ No treatment needed
*****What does it mean by Sports Anemia is a Diagnosis of exclusion?
Systematically ruling out all other possible conditions that could explain a patient’s symptoms. (it cannot possibly be one of the other causes/types of anemia)
A diagnosis of exclusion occurs when no single test or observation can definitively confirm a condition, so healthcare providers identify it by eliminating other plausible causes of the symptoms
◦ Need to rule out dietary or medical causes of anemia thus Sports anemia is a diagnosis of exclusion
*****What are 3 sport factors that relate to sport anemia?
Type of sport: ENDURANCE = changes iron status assessment parameters more than other sports
Intensity/duration of training: GREATER = greater change for finding sport anemia
Adaptation to training: sport anemia is more likely to be found in early stages of a new training regime
****What is the Most prevalent Genetic disorder in north americans
Hemochromatosis
1/300 canadians
******What is Hemochromatosis
Most prevalent Genetic disorder in north Americans that results in:
Heightened Iron absorption + excessive storage of iron Where it should not be:
skin liver, heart, pancreases, pituitary gland + joints
What is Excess Iron absorption + storage in Hemochromatosis related to?
CHD (heart disease)
Cirrhosis of the liver + or liver cancer
******What does the Existence + prevalence of a Disorder like hemochromatosis mean in terms of treatment + prescription?
All athletes should have their iron status checked before taking nutrient supplements that contain iron, including MVI.
if give supplements to someone with this condition = can risk health