Nutrition, Metabolism, Energy: Part 2 (copy)
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Pancreas
Triangular gland located partially behind stomach
Has both exocrine and endocrine cells
Acinar cells
Pancreatic islets
Acinar cells
exocrine cells that produce enzyme-rich juice for digestion
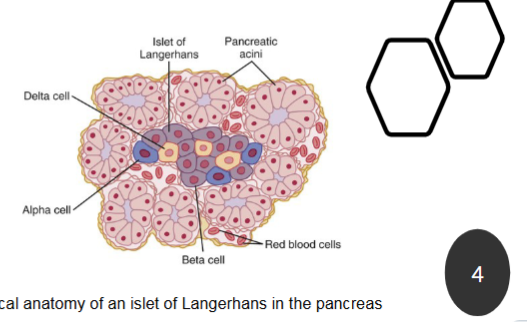
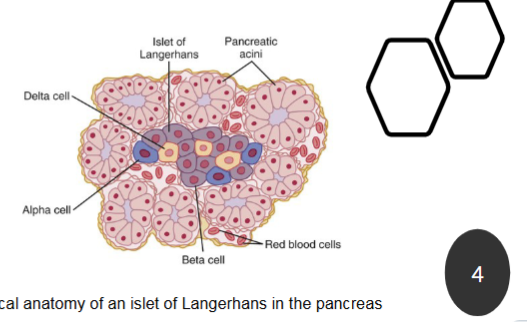
What cells does pancreatic islets contain?
Pancreatic islets (islets of Langerhans) contain endocrine cells for control of blood glucose
Alpha cells produce glucagon
Beta cells produce insulin
Delta (D) cells secrete somatostatin
F cells produce pancreatic polypeptide
Insulin and Glucagon from the pancreas regulate blood glucose levels

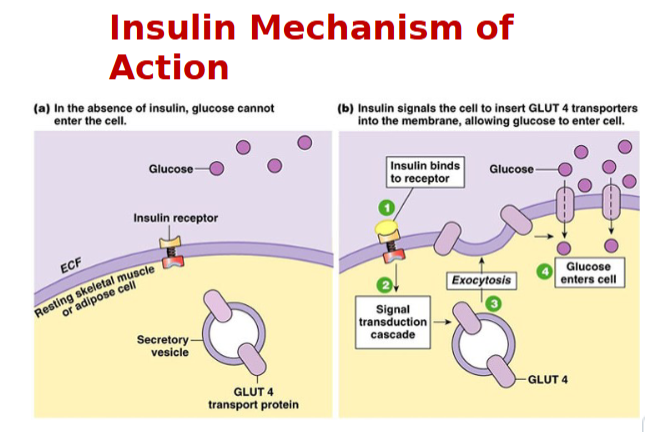
Insulin mechanism of Action
Via facilitated diffusion
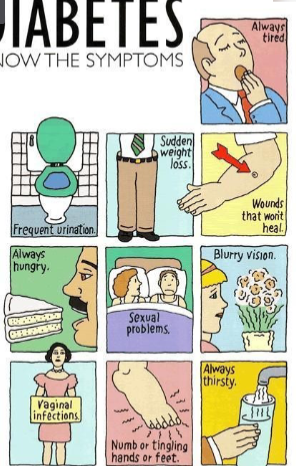
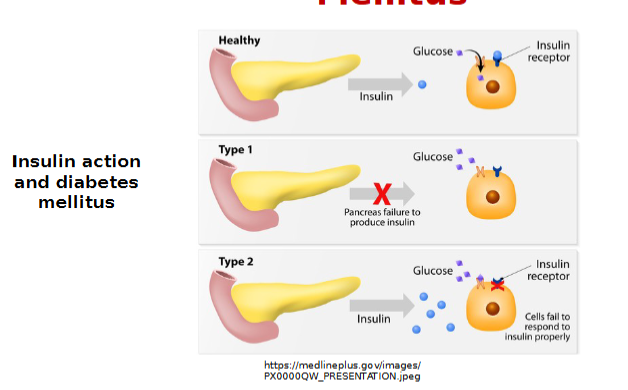
Diabetes Mellitus
is a group of metabolic diseases characterized by high levels of blood glucose resulting from defects in insulin production, insulin action, or both.
complex disorders of CHO, fat and protein metabolism
Blurry vision= humor in the eye becomes sugary
Type 1 Diabetes
Autoimmune destruction of beta cells
Absolute insulin deficiency-WHY? because there isn’t any other organ or gland that can produce insulin leads to hyperglycemia
require daily insulin injections multiple times a day
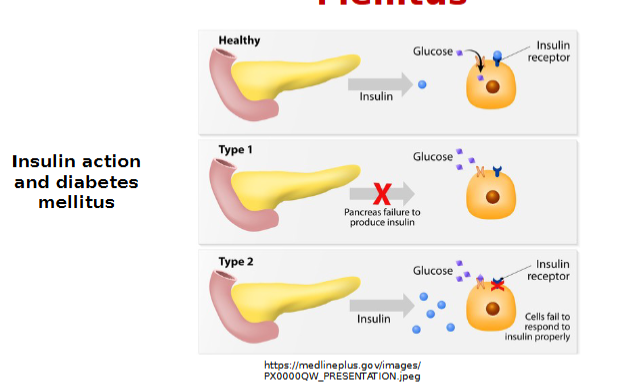
Type 2 Diabetes Mellitus
Insulin resistance = relative insulin deficiency
e.g. interference with insulin binding to target tissue
Net results in inefficient transport of blood glucose into the cells also leads to hyperglycemia
Require oral hypoglycemics
Consequence of insulin deficit (diabetes mellitus)
Polyphagia occurs because body think body is going into starvation mode
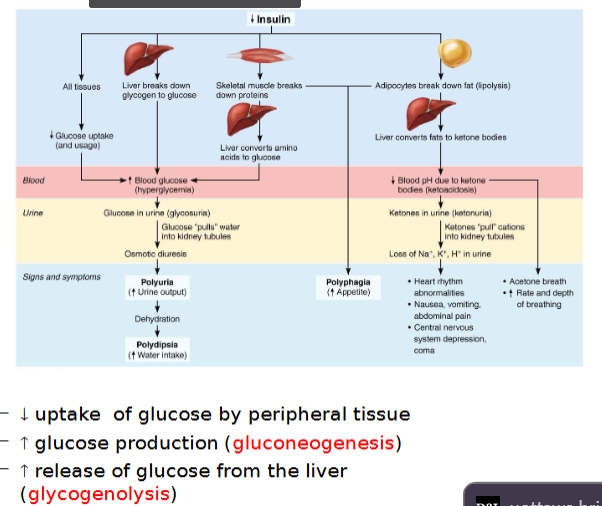
Metabolic consequences of Type 1 DM
When sugars cannot be used as fuel, as in DM, fats are used, causing lipidemia (high levels of fatty acids in blood)
Fatty acid metabolism (lipolysis) results in formation of ketones (ketone bodies)
Ketones are acidic, and their build-up in blood can cause ketoacidosis
Also causes ketonuria
acute consequences of type 1 DM
rarely in type 2 because of small insulin production
Untreated ketoacidosis causes hyperpnea, disrupted heart activity and O2 transport, and severe depression of nervous system that can possibly lead to coma and death
Hyperinsulinism (hyperinsulinemia)
Excessive insulin secretion(sometimes from injections)
Causes hypoglycemia: low blood glucose levels
Symptoms: anxiety, nervousness, disorientation, unconsciousness, even death
Treatment: sugar ingestion
Type 2 Diabetes Mellitus risk factors
age, obesity, hypertension, physical inactivity, and family history.
Consequences of obesity
adipose tissue secrete hormone that decrease insulin sensitivity
increased FFAs/ TGs and cholesterol:
interfere with intracellular insulin signalling
decrease tissue responses to insulin
alter incretin actions (from GIP or GLP)
promote inflammation
increase inflammatory cytokines that cause insulin resistance and are toxic to beta cells
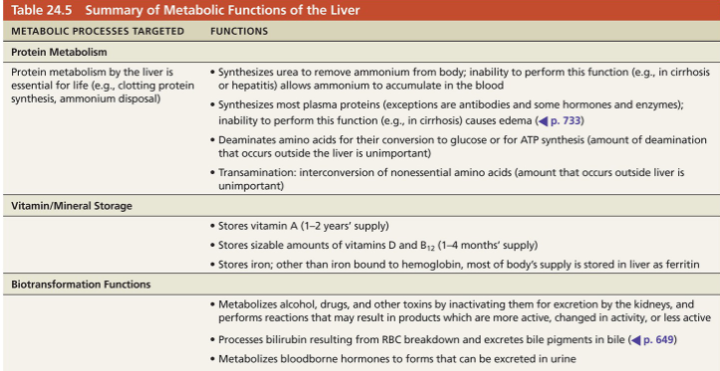
Metabolic role of liver (5)
Hepatocytes carry out ~500 metabolic functions
Process nearly every class of nutrient
Play major role in regulating plasma cholesterol levels
responsible for producing clotting factors
Store vitamins and minerals
Metabolize alcohol, drugs, hormones, and bilirubin
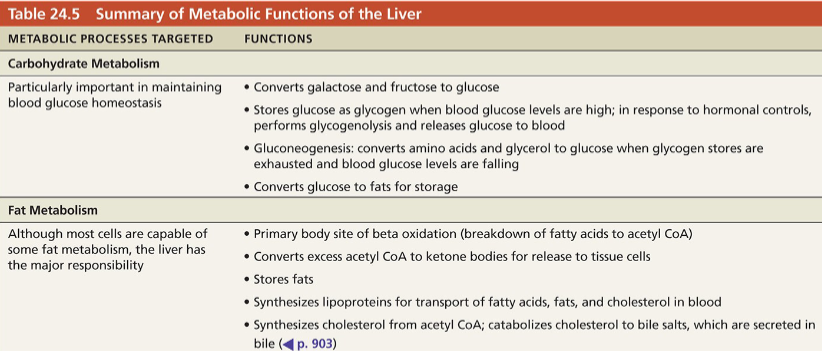
Summary of metabolic functions of liver
Biotransformation: ability to take a compound and convert it to something else
EX: bilirubin broken down from RBCs is conjugated by liver into something that can be excreted
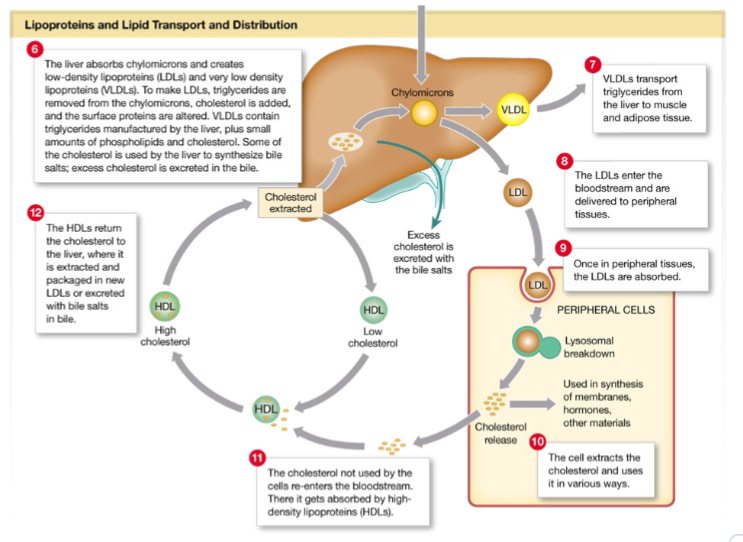
Cholesterol metabolism and regulation of blood cholesterol levels(6)
Not used as an energy source
Structural basis of bile salts, steroid hormones, and vitamin D
Major component of plasma membranes
15% is ingested, the rest made in body, primarily by liver
Lost from body when catabolized or secreted in bile salts that are lost in feces
is hydrophobic and must be transported via lipoproteins
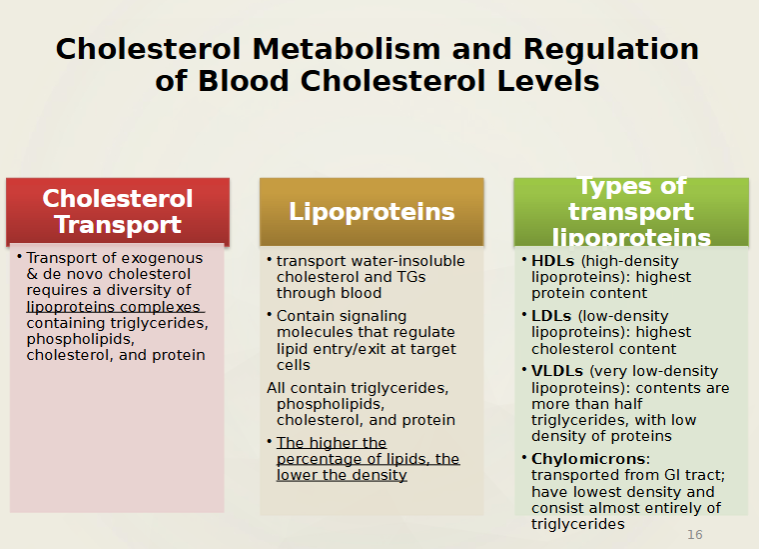
4 types and Composition of lipoprotein
Includes
VLDLs: when they dump triglycerides, they become LDLs
LDLs: Along with VLDLs start to deposit cholesterol into peripheral structures like artery walls causing health problems
HDLs: can be reused and is there to prevent accumulation of cholesterol in and around tissues
Chylomicrons: is the least dense of all
The more protein, the more density it has. The more triglycerides, the less dense
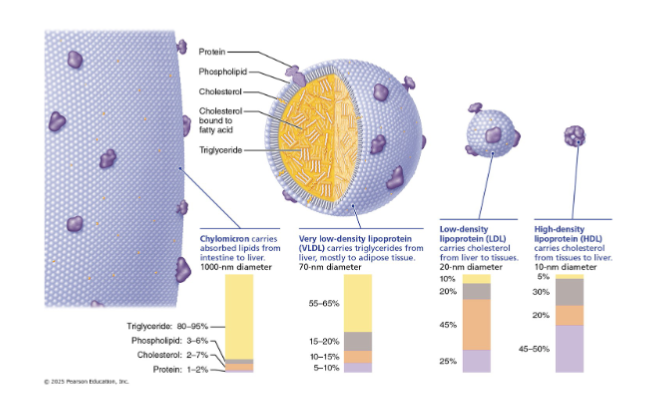
VLDLs
transport triglycerides from liver to peripheral tissues (mostly adipose
LDLs
transport cholesterol to peripheral tissues for membranes, storage, or hormone synthesis
HDLs
transport excess cholesterol from peripheral tissues to liver to be broken down and secreted into bile
Also provide cholesterol to steroid-producing organs
Blood levels of total cholesterol, LDL, and HDL
Generally, Blood tests measure total cholesterol < 200 mg/dL (< 5.2 mmol/L) of blood is desirable for adults
More important to look at ratio of lipoproteins transporting cholesterol in blood esp. for ppl with high cardiovascular risk
High levels of LDL are generally considered bad (associated with atherosclerosis)
High levels of HDL were considered good because it transported cholesterol destined for degradation
Why does restricting dietary cholesterol not markedly reduce cholesterol levels?
Because the liver produces cholesterol at a basal level regardless of dietary cholesterol intake so reducing dietary cholesterol intake doesn’t make a huge difference
what is the MOST important effect on regulating blood cholesterol levels?
The relative amounts of saturated and usaturated fatty acids
Saturated fatty acids: stimulate liver synthesis of cholesterol & inhibit its excretion from body
Unsaturated fatty acids: enhance excretion of cholesterol into bile salts. Should be in diets
Trans fats: increases LDL & reduce HDL
Unsaturated omega-3 fatty acids effect on regulating cholesterol levels
Very good for body
Unsaturated omega-3 fatty acids (found in cold-water fish) have lower proportions of saturated fats and cholesterol
Helps cardiovascular system: Make platelets less sticky and help prevent spontaneous clotting
reduces risk of thrombus and embolism
Appear to lower blood pressure
Other factors that regulate blood cholesterol levels
Cigarette smoking and stress lower HDL levels
Regular aerobic exercise and estrogens lower LDL and increase HDL levels.
Menopausal women are at risk since they have lower estrogen
Body Shape
How does body shape contribute to regulating blood cholesterol levels
Apples” (people with upper body and abdominal fat, seen more often in males) tend to have higher levels of cholesterol and LDLs
higher risk of type 2, metabolic syndrome, etc.
“Pears” (whose fat is localized in the hips and thighs, more common in females) tend to have lower levels
because fat is away from key organs
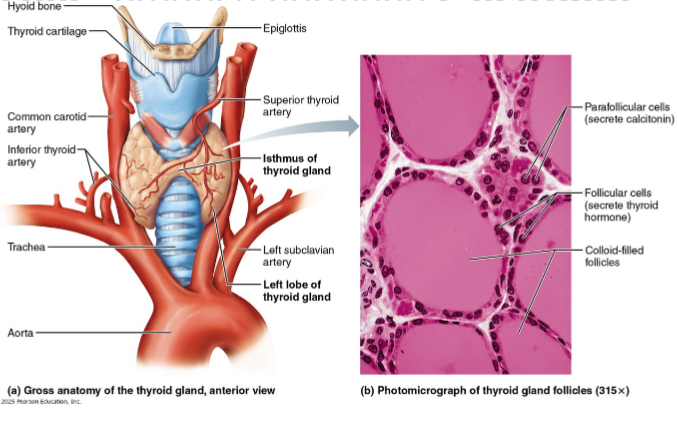
Location and structure of thyroid gland
Butterfly-shaped gland in anterior neck on the trachea, just inferior to larynx, that consists of:
Isthmus: median mass connecting two lateral lobes
closed follicles: hollow sphere of epithelial follicular cells that produce glycoprotein thyroglobulin
Colloid: fluid of follicle lumen containing thyroglobulin & iodine (precursor to thyroid hormone)
Parafollicular cells: produce hormone calcitonin
calcitonin lowers blood calcium levels
Role of thyroid hormone
the body’s major metabolic hormone
Is lipid soluble so transported as lipoprotein
functions like a STEROID hormone
affects virtually every cell in the body
Just like steroid hormones, it enters target cell and binds to intracellular receptors within nucleus
triggers transcription of various metabolic gene
takes longer
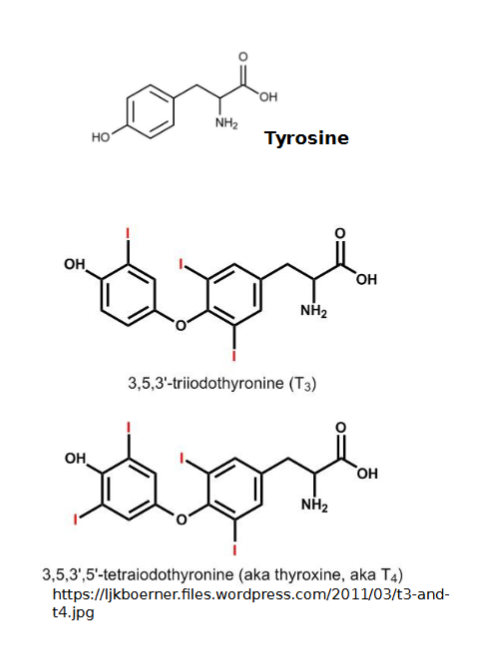
2 forms of thyroid hormone
Both are iodine-containing amine hormones and both work together
T4 (thyroxine): major form that consists of two tyrosine molecules with four bound iodine atoms. 94% of TH is T4
Most converted to T3 at tissue level
T3 (triiodothyronine): form that has two tyrosine molecules with three bound iodine atoms. The most potent/active form
T3 has higher affinity for receptors than T4
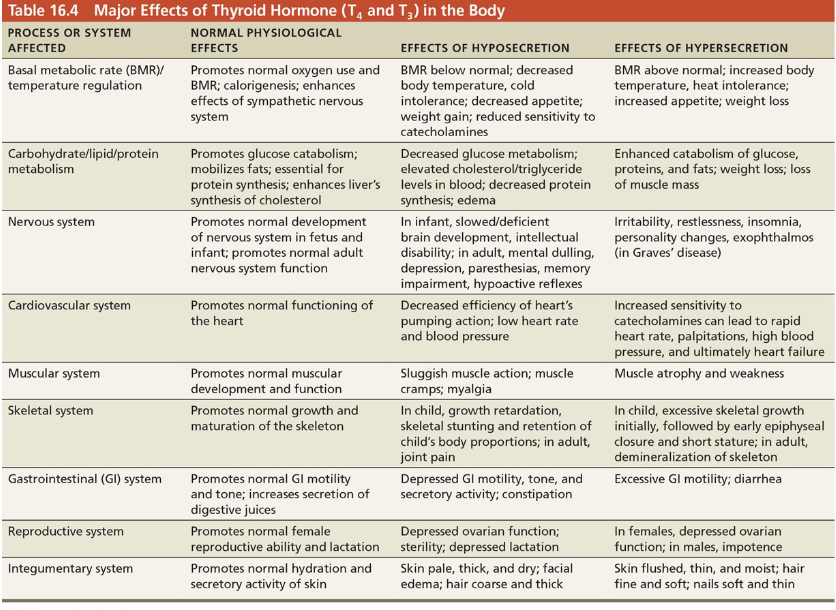
3 major Effects of thyroid hormone
Increases basal metabolic rate and heat production
Referred to as calorigenic effect
Regulates tissue growth and development
Critical for normal skeletal and nervous system development and reproductive capabilities
Maintains blood pressure
Increases adrenergic receptors in blood vessels
can increase cardiac rate and cardiac output
hypothyroidism does opposite of that
Major effects of thyroid hormone in the body
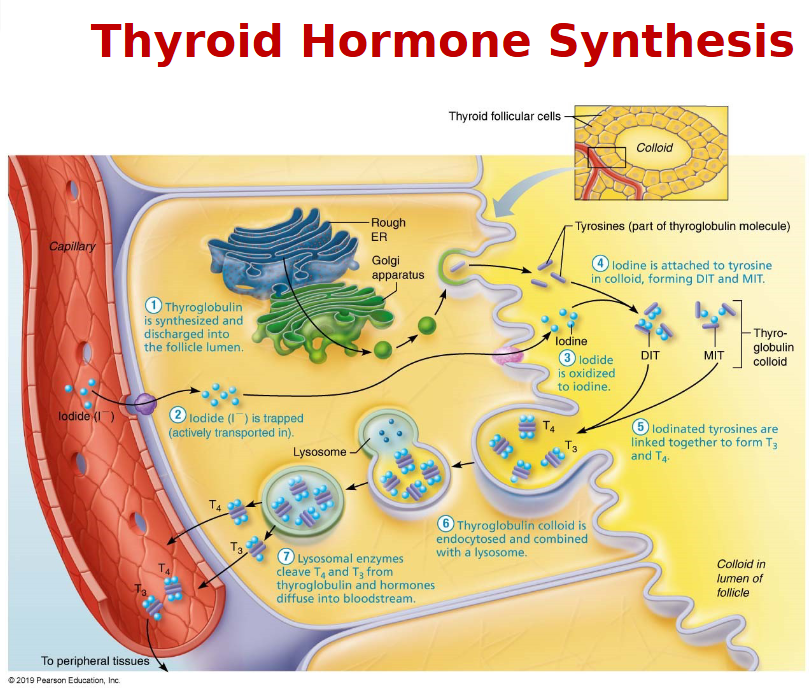
Synthesis of thyroid hormone
T3 and T4 are stored in the follicles lumen until triggered for release by TSH
amounts sufficient for 2-3 months
DIT has 2 iodines attached (FYI)
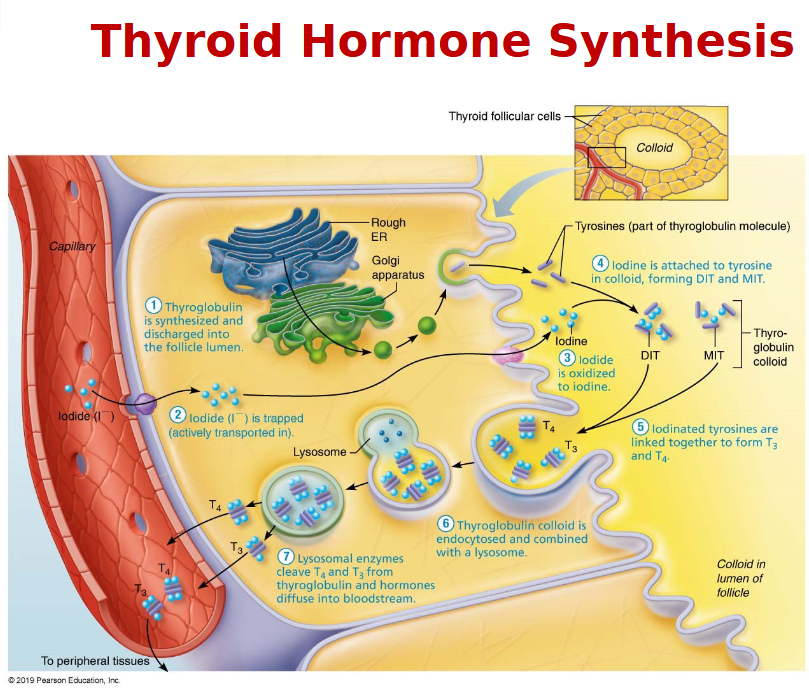
Role of iodine in TH synthesis
Iodine - ingested in the form of iodides is necessary for the formation of T3/T4
Iodide from the GI→ the blood and is trapped in the thyroid follicles that actively pump iodide from the blood into the interior of the cells
The rate of iodide trapping is influenced by Thyroid Stimulating Hormone(TSH)
Transport and regulation of thyroid hormone
T4 & T3 transported by thyroxine-binding globulins (TBGs)
Both bind to target receptors, but T3 is 10 times more active than T4
Peripheral tissues have enzyme that to convert T4 to T3 (-1 iodine)
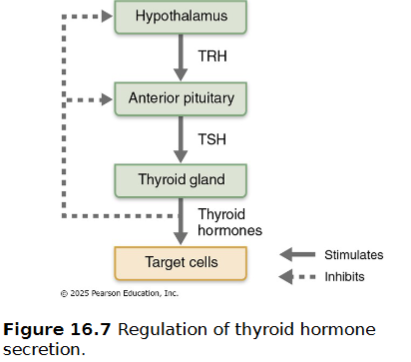
Negative feedback regulation of TH release
Falling TH levels stimulate release of thyroid-stimulating hormone (TSH)
Rising TH levels provide negative feedback inhibition on TSH
TSH can also be inhibited by GHIH, dopamine, and increased levels of cortisol and iodide
Hypersecretion of TH
most common type is Graves’ disease
Grave’s disease
Autoimmune disease: body makes abnormal antibodies(they mimic TSH) directed against thyroid follicular cells
Antibodies mimic TSH, stimulating TH release
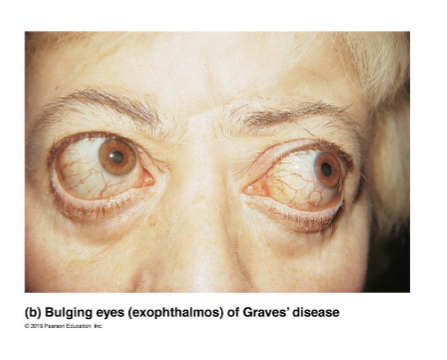
6 Symptoms of Grave’s disease
Symptoms include elevated metabolic rate, sweating, rapid and irregular heartbeats, nervousness, and weight loss despite adequate food
Exophthalmos may result in eyes protruding as fatty tissue behind eyes becomes edematous and fibrous
Treatments for Grave’s disease
Treatments include
surgical removal of thyroid gland
radioactive iodine to destroy active thyroid cells(less common)
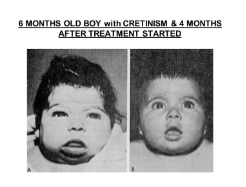
TH hyposecretion
in adults can lead to myxedema/goiter.
in infants can lead to cretinism
8 Symptoms of myxedema
low metabolic rate
thick and/or dry skin
puffy eyes
feeling chilled
constipation
edema
mental sluggishness
lethargy

Hyposecretion due to lack of iodine
If due to lack of iodine, a goiter may develop
not enough thyroid hormone so thyroid glands ramps up amount of thyroglobulin but there is not iodine to collect precursor, thus enlargement of thyroid gland
↑ synthesize of unusable thyroglobulin causes thyroid to enlarge

Cretinism
Congenital hypothyroidism leads to cretinism
Symptoms include intellectual disabilities, short and disproportionately sized body, thick tongue and neck
Energy balance
energy released from food (intake) must equal total energy output
Energy intake
energy derived from absorbable foods = energy liberated during food oxidation
Energy output
immediately lost as heat (~60%)
used to do work (driven by ATP)
stored as fat or glycogen
Uses of energy in the body
Nearly all energy from food is eventually converted to heat, which cannot be used to do work, but it
warms tissues and blood
helps maintain homeostatic body temperature
allows metabolic reactions to occur efficiently
Positive energy balance = weight, energy intake exceeds energy output. Vice versa for negative energy balance

Body mass Index (BMI)
is a formula used to determine obesity based on a person’s weight relative to height

How is BMI maintained
Body mass (BM) is maintained when energy intake = energy expenditure
Clinically, overweight is defined by a BMI of 25–30 (carries some health risk)
Obesity is a BMI > 30 (with markedly increased health risk)
health risks associated with BMI doesn’t account for age, sex, ethnicity, muscle mass, etc…
5 major Risks of obesity
highest risk factor of type 2 diabetes mellitus
hypertension
heart disease / atherosclerosis
cancer
osteoarthritis
Canadian statistics of obesity
Nearly 68 % of adults are overweight or obese combined
Around 33 % of Canadian adults (ages 18– 79) are classified as obese based on BMI
30 %+ of children and youth aged 5–17 fall into overweight or obesity combined
around 8.6 % of Canadian children and youth aged 6 to 17 years are classified as obese
About 3.9 million Canadians (≈9.7 % of the population aged 1+ years) live with diagnosed diabetes (both type 1 and type 2), according to 2023–2024 surveillance
Metabolic syndrome
cluster of five risk factors
High blood pressure comes from storing fat into adipose tissues, which are vascularized. This means more work for heart to pump blood to those sites

5 factors seen in metabolic syndrome
↑ Waist circumference
↑ Blood pressure
↑ Blood glucose
↑ Blood triglycerides
↓ Blood HDL cholesterol
Presence of these factors can:
Double chance of heart disease
Increase risk of diabetes five times
Increased risk of stroke
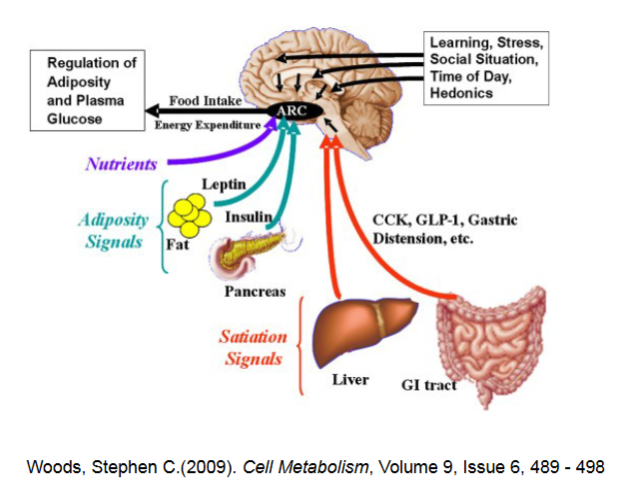
Regulation of food intake
Current theories focus mainly on neural signals from GI tract, hormones, and blood nutrient levels
To lesser extent, body temperature and psychological factors also play role
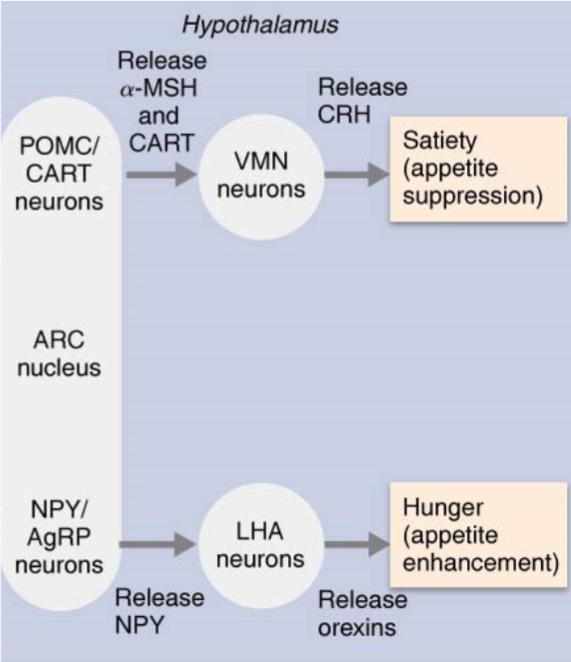
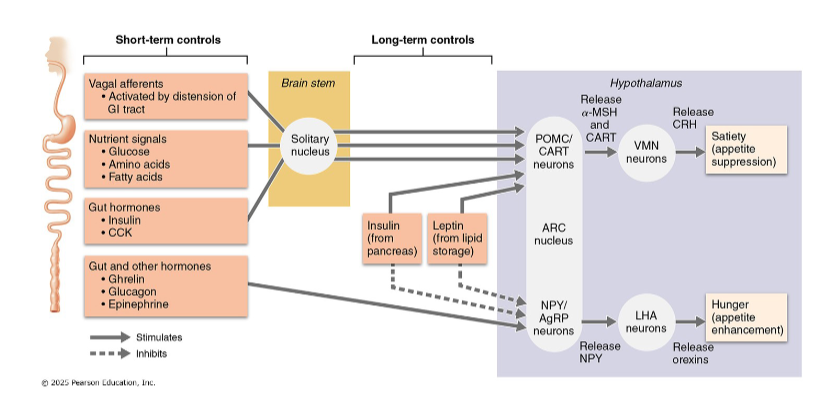
Areas of hypothalamus release peptides that influence feeding behavior
Arcuate nucleus (ARC): controls hunger, fullness, and regulating body weight
stimulates/inhibits:
Ventromedial Nucleus (VMN)
Lateral Hypothalamic Area (LHA)
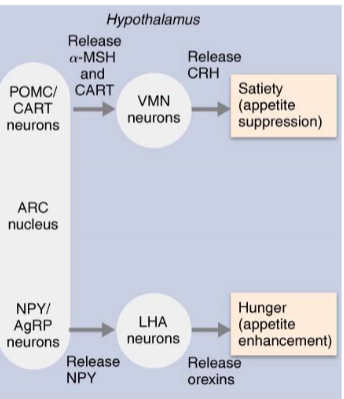
Hunger-promoting neurons
Some ARC neurons release neuropeptide Y (NPY) and agouti-related peptides(AgRP) that enhance appetite.
These increase appetite by stimulating release of orexins from Lateral hypothalamic area (LHA) neurons
orexins increase in food-seeking behavior AND trying to reduce energy expenditure
too much NPY can trigger obesity
With type 1 diabetes, lack of insulin will not prevent food-seeking behavior
Type 2 diabetes, downstream of insulin isn’t functioning also leading to food seeking behavior
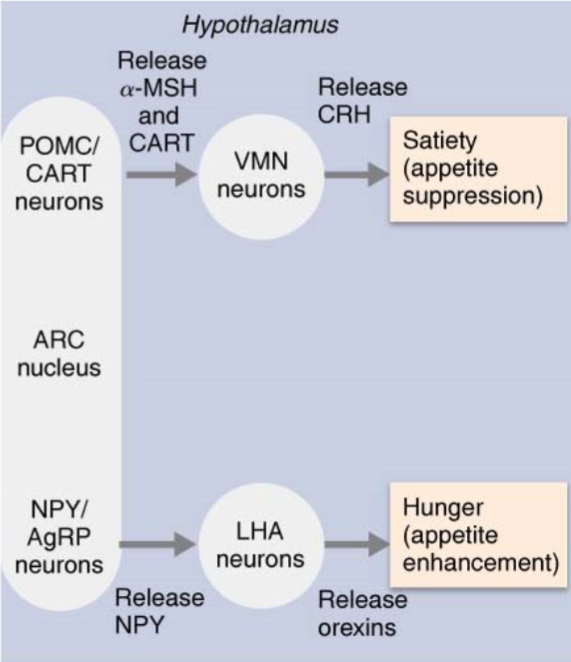
Satiety-promoting neurons
Other ARC neurons release pro- opiomelanocortin (POMC) and cocaine-/amphetamine-regulated transcript (CART), which suppress appetite
These act on the ventromedial nucleus (VMN), causing it to release CRH (important appetite suppressor) when energy supply is sufficient
if VMN is damaged, continuous feeding will occur
What is feeding behavior and hunger regulated by?
Neural signals from digestive tract via vagus nerve
Bloodborne signals related to body energy stores (glucose, amino acids, fatty acids)
Hormones(grehlin, etc..)
To lesser extent, body temperature and psychological factors
All operate through brain thermoreceptors, chemoreceptors, and others
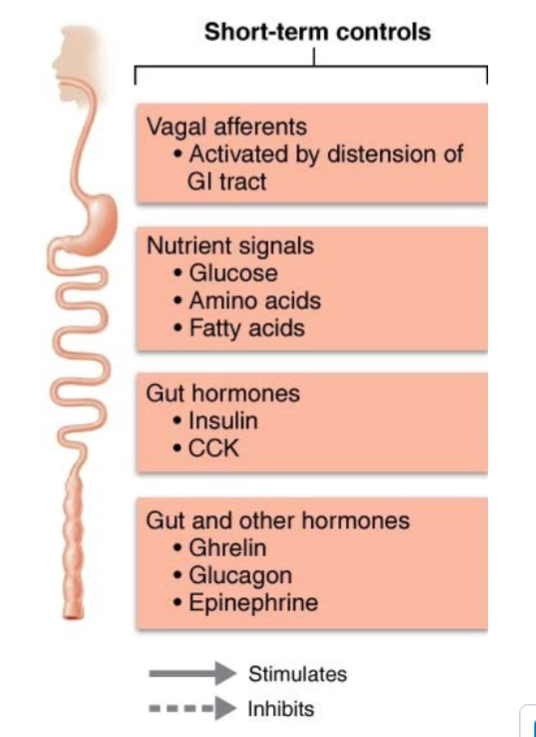
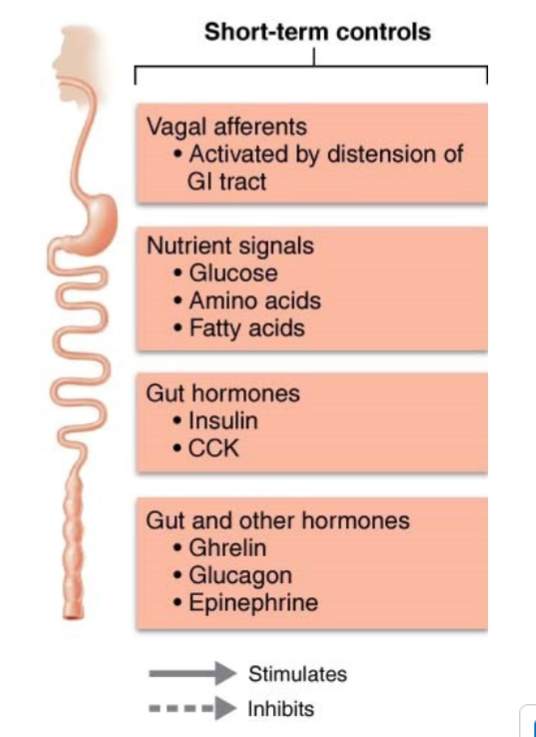
Food intake is subject to both short- and long-term controls
What contributes to short-term regulation of food intake
Neural signals from digestive tract
Nutrient signals related to energy stores
Hormones
How do neural signals from digestive tract play a role in short-term regulation of food intake
High protein content of meal increases and prolongs afferent vagal signals
Distension sends signals to mechanoreceptors along vagus nerve that suppress hunger center
How do nutrient signals related to energy stores play a role in short-term regulation of food intake
Increased nutrient levels in blood depress eating
Rising blood glucose levels
Elevated blood amino acid levels
Blood levels of fatty acids
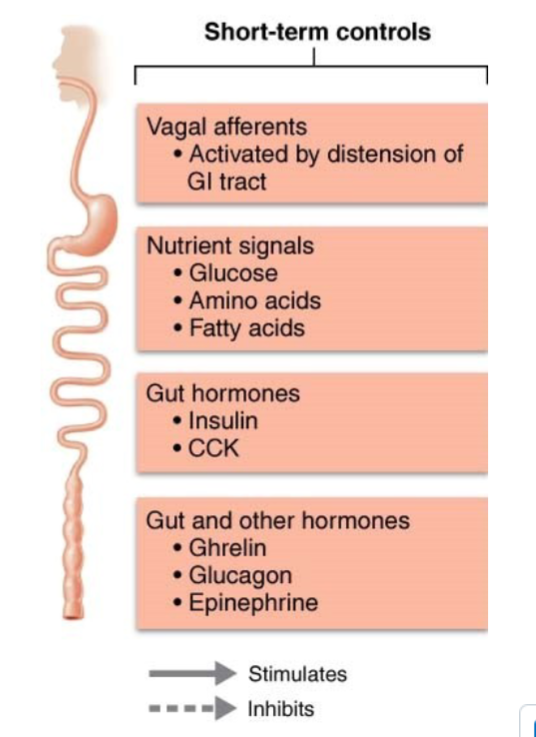
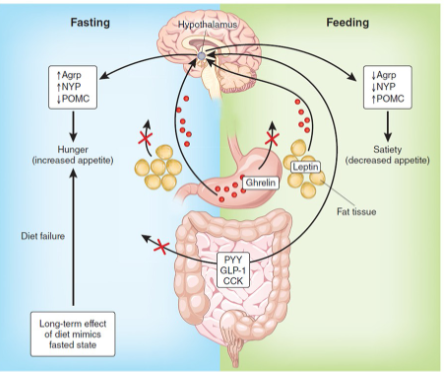
How do hormones play a role in short-term regulation of food intake
Gut hormones (e.g., insulin and CCK are activated in presence of nutrients. CCK is present during entire digestive process) signal satiety and depress hunger
Glucagon and epinephrine released during fasting and stimulate hunger
Ghrelin (Ghr) from stomach is a powerful appetite stimulant. Body’s main hunger hormone
Levels peak prior to mealtime and drop after a meal
How does Leptin play a role in LONG-term regulation of food intake
Hormone secreted by fat cells in response to increased body fat mass
If fat mass increases, leptin levels rise; more leptin binds to receptors in
ARC that:
Stimulate expression of CART
Suppress release of NPY (most potent appetite stimulant known)
Decreasing release of appetite-enhancing orexins from LHA
Decreasing appetite/food intake, eventually promoting weight loss
If fat stores decrease, leptin levels fall, producing opposite effect
Increasing appetite/food intake, eventually promoting weight gain
Rising leptin level causes some weight loss but is no “magic bullet” for obese patients
Obese people have high leptin levels but seem to be resistant to its action (unknown reason)
Consensus: leptin’s main role is to protect against weight loss in times of nutritional deprivation
6 additional factors play a role in regulation of food intake
Temperature: cold activates hunger
Stress: depends on individual
Psychological factors
Adenovirus infections
Sleep deprivation
Composition of gut bacteria
Metabolic rate
total heat produced by chemical reactions and mechanical work of body
How is metabolic rate measured
Directly: calorimeter measures heat liberated into water chamber
Indirectly: respirometer measures oxygen consumption (directly proportional to heat production)
Basal metabolic rate
MINIMUM amount of energy body needs to perform its most essential activities
Measured in fasting state (12-hour fast)
reclining position
relaxed mentally & physically
at a certain room temperature 20–25°C
Not lowest metabolic state, that’s during sleep (skeletal muscles fully relaxed)
Recorded as kilocalories per square meter of body surface per hour (kcal/m2/h)
Example: 70 kg adult BMR = 66 kcal/h
BMR is not the lowest metabolic rate (that occurs when sleeping)
5 major influences on BMR
Age and gender: BMR decreases with age
Males have disproportionately higher BMR due to higher muscle mass
higher in children
lower in females, EXCEPT during pregnancy
Body temperature: BMR increases with temperature
Stress: BMR increases with stress
Thyroxine: increases oxygen consumption, cellular respiration, and BMR
Hyperthyroidism
level of thyroid hormone is higher in the body
causes many problems resulting from the high BMR it produces
Body catabolizes stored fats and tissue proteins
Person often loses weight despite increased hunger and food intake
Bones weaken, and muscles, including heart, begin to atrophy
Hypothyroidism results in slowed metabolism, obesity, and diminished thought processes due to decrease of thyroid hormone
Total metabolic rate(TMR)
sum of all calories burned in a 24hr period
Rate of energy consumption to fuel all ongoing activities
e.g. female whose energy needs are ~ 2000 kcal/day may spend about 1400 kcal supporting vital body activities
Increases with skeletal muscle activity
Even slight increases in muscular work significantly increase TMR and heat production
TMR also increases with food ingestion (food-induced thermogenesis)
Greatest with protein ingestion
Fasting or very low caloric intake depresses TMR
Total metabolic rate (TMR) = Total daily energy expenditure (TDEE)
Components are
Basal metabolic rate (BMR)
The thermic effect of food (TEF)
Energy expended on physical activity (thermic effect of activity = TEA)
Regulation of body temperature
Only ~ 40% of energy released by catabolism can be captured by ATP; the rest is lost as heat
Cannot be used to do work
Warms the tissues and blood
Helps maintain the homeostatic body temperature
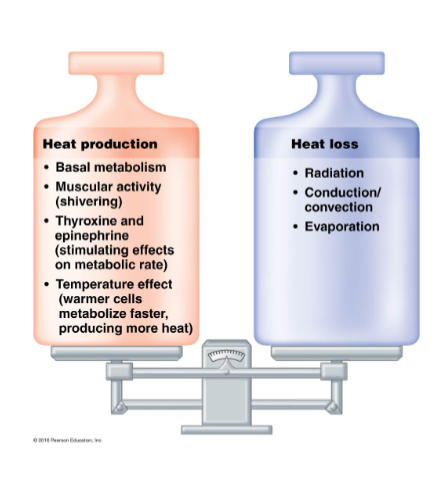
Body temperature reflects the balance between heat production and heat loss
At rest, the liver, heart, brain, kidneys & endocrine organs generate most heat
Inactive skeletal muscles account for only ~ 20 – 30%
During exercise, heat production from skeletal muscles increases dramatically
Active muscle can produce 30-40X more heat than the rest of the body
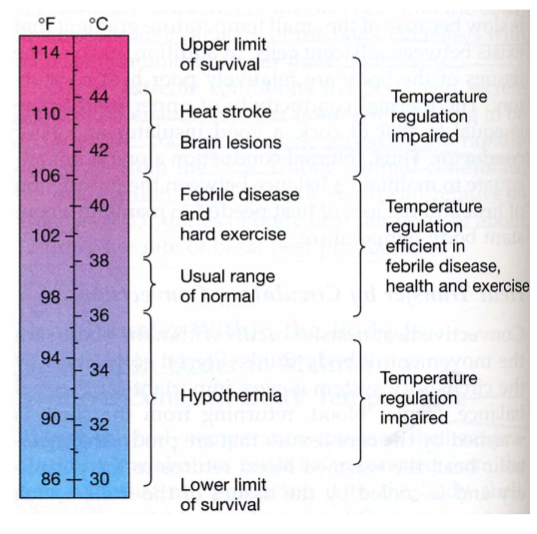
What is normal body temperature
Normal body temperature = 37°C
Optimal enzyme activity at this temperature
Increased temperature denatures proteins and depresses neurons
Rate of chemical reactions increases ~10% for each 1°C rise in temperature
Body can handle the cold better than heat
In children under 5, temperature of 41°C (106°F) can lead to convulsions
~43°C (109°F) is the limit for life
Tissues can tolerate low body temperatures better
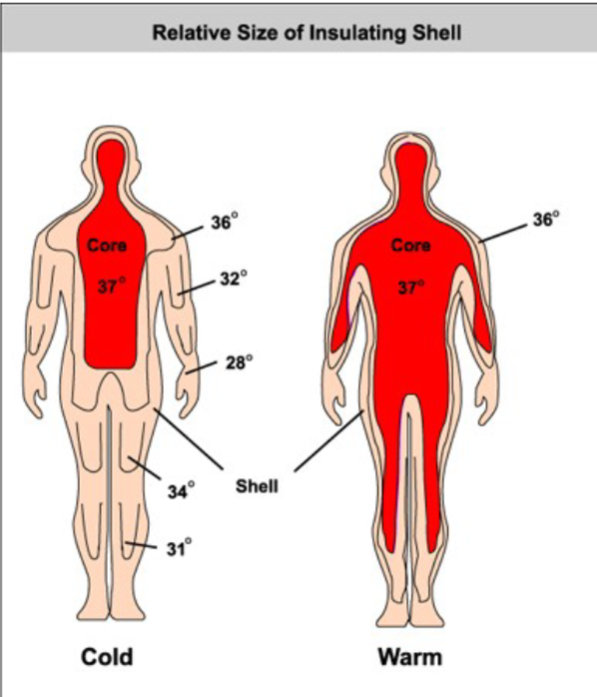
Core and shell temperature
Core (organs within skull and thoracic and abdominal cavities) has highest temperature
Rectal temperature is best clinical indicator
Shell (skin) has lowest temperature
Fluctuates between 20°C and 40°C
Core temperature is regulated and is fairly constant.
Blood is major agent of heat exchange between core and shell
4 mechanisms of heat transfer
Radiation
Conduction
Convection
Evaporation
Radiation as a mechanism of heat transfer
loss of heat by infrared rays ; objects are not in contact (receiving heat from the sun)
Explains why cold room warms up after it fills with people
Normally accounts for about 50% of body’s heat loss

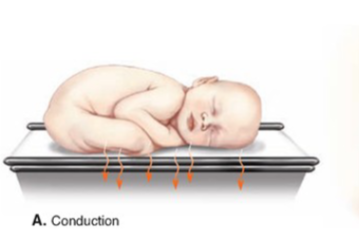
Conduction
heat transfer between molecules of objects in direct contact
E.g., transfer of heat from hot tub water to skin
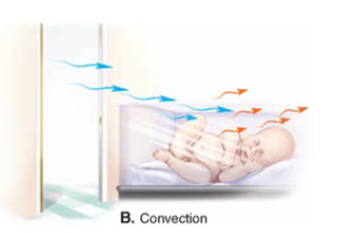
Convection
heat transfer to surrounding air or water
warm air expands and rises (away from skin) and denser cool air falls (replacing warm air)
Conduction and Convection account for 15– 20% of body’s heat loss
Ex: cooling down from a fan
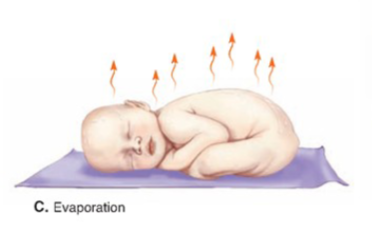
Evaporation
heat loss due to evaporation of water from body surfaces; heat absorbed by water during evaporation is known as heat of vaporization
a mechanism of cooling the body down
Insensible heat loss
accompanies insensible water loss from lungs, oral mucosa, and skin
unnoticeable
Loss ~ 10% of basal heat production
Sensible heat loss
when body temperature rises and sweating increases water vaporization
Factors contributing to heat balance
Thermoregulatory centers
preoptic region of hypothalamus is main integrating center for thermoregulation
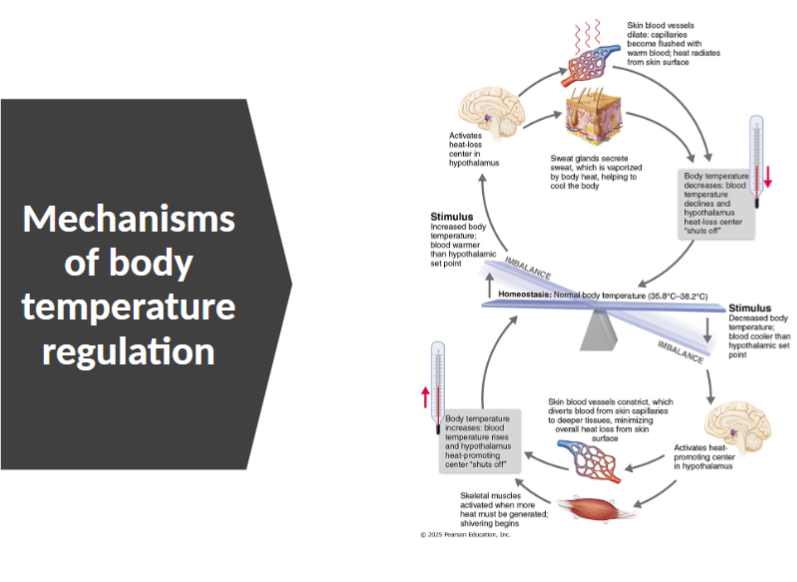
2 thermoregulatory centers of hypothalamus
Heat-loss center: as core warms up, dissipates heat
Heat-promoting center: as body feels cold, body will generate heat
Where does hypothalamus receive afferent input from
Peripheral thermoreceptors in shell (skin)
Central thermoreceptors in core (some in hypothalamus
Initiates appropriate heat-loss and heat-promoting activities
Central thermoreceptors have more influence, but varying inputs from peripheral probably alert hypothalamus to the need to prevent temperature changes in the core
Heat promoting mechanisms
prevents hypothermia
When external temperature is low (or blood temperature falls), heat-promoting center is activated, triggering one or more of the following mechanisms:
Constriction
shivering
increases in metabolic rate
enhanced release of thyroxine
Constriction of cutaneous blood vessels as a heat-promoting mechanism
Regulated by sympathetic nervous system
shivering as a heat-promoting mechanism
Heat from skeletal muscle activity and activation increases heat
increases in metabolic rate as a heat-promoting mechanism
Chemical (non-shivering) thermogenesis: via epinephrine and norepinephrine stimulated by cold temperatures
Mechanism seen primarily in infants (in brown adipose tissue: has increased capacity to generate heat, cells don’t capture that and instead is converted to heat)
Enhanced release of thyroxine
Seen only in infants when environmental temperature decreases gradually (e.g., transition from summer to winter
Behavioral modifications (voluntary) to temp changes (cold temp)
Putting on more clothing
Drinking hot fluids
Changing posture (clasping arms across chest)
Increasing physical activity (jumping up and down)
Heat-loss mechanisms
When core body temperature rises above normal, the heat-loss center is activated, triggering one or both:
Inhibition of heat-promoting center
Dilation of cutaneous blood vessels: increasing heat loss by radiation, conduction, and convection
Enhanced sweating: works well in dry air but is less effective when humidity is high
Voluntary measures of heat-loss mechanisms include…
Wearing light-colored, loose-fitting clothing
take off a sweater, turn on a fan, get a cold drink
Reducing activity and seeking a cooler environment
Mechanisms of body temperature regulation
Hyperthermia (high body temperature)
Elevated body temp overwhelms the heat loss processes
At ~ 41°C hypothalamus is depressed (heat loss ceases) leading to positive- feedback cycle
heat stroke results is not corrected
Can be fatal if not corrected
Heat exhaustion (exertion-induced heat exhaustion)
Heat-associated extreme sweating and collapse during or following vigorous physical exertion due to dehydration and low blood pressure
Causes elevated body temperature and mental confusion and/or fainting
As heat-loss mechanisms struggle to function, may progress to heat stroke
Hypothermia (low body temp)
Caused by prolonged cold exposure
Vital signs (respiratory and heart rate, blood pressure) decrease as cellular (enzymatic) activities slow
Person begins to feel drowsy, even (oddly) comfortable (no longer feels cold)
Shivering stops at core temperature of 30-32°C
Can progress to coma and finally death (by cardiac arrest) at ~21°C
Fever
Controlled hyperthermia
Cause: mostly due to infection, but also cancer, allergies, or CNS injuries
Function: rising temp enhances immune response, speeds healing, and inhibits bacterial growth
Macrophages release cytokines called pyrogens that cause release of prostaglandins, resetting hypothalamic thermostat higher than normal temperature.
Triggers heat-producing mechanisms, and temperature rises
The set-point temperature of the body will remain elevated until
prostaglandins (PGE) are no longer present
Natural body defenses or antibiotics reverse disease process
Thermostat returns to normal after infection (or disease process) is controlled
Heat-loss mechanisms active again; sweating begins, skin becomes flushed and warm (signs that fever has broken