Looks like no one added any tags here yet for you.
above the clavicle that is where the apex of the lung is located
where do you first listen to the lungs sounds ANTERIORLY?
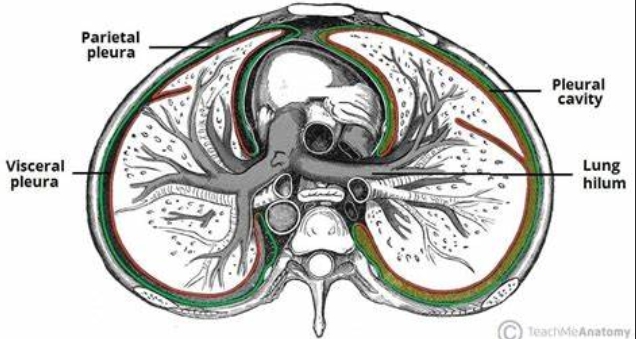
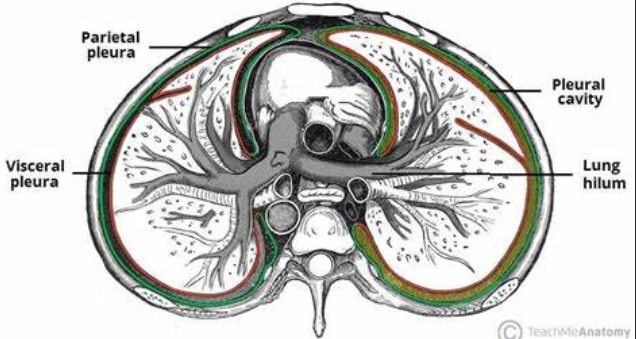
pleura/pleurae
2 serous membranes that cover the outer surface of the lung
visceral pleura
parietal pleura
visceral pleura
lies Next to lungs
No sensory Nerves;
parietal pleura
lines the inner rib cage & upper surface of the diaphragm
Rich nerve innervation;
Lines inner rib cage
inflammation produces pleuritic pain with deep inspiration, for example, in pleurisy, pneumonia, and pulmonary embolism
pleural effusion
accumulation of fluid between the pleurae
pt with pleuritis will avoid taking deep breaths due to pain. worsening sharp pain often occurs during breathing, coughing, or sneezing. These actions cause pleura to move, which aggravates the inflammation. As a result, the patient may take shallow breaths in an attempt to reduce discomfort.
Is the patient with pleuritis, taking deep breaths? WHY?
risk of shallow breathing include atelectasis (alveoli collapse due to underinflation), pneumonia (due to buildup of mucus), and hypoxemia (reduced amount of O2 body receives)
what is the risk of patient with pleuritis?
inspiration
primary muscle is diaphragm
muscles contract & thorax expands
expiration
muscle relax and thorax contracts
shortness of breath
wheezing
cough
hemoptysis
purulent sputum
chest pain
what are common or concerning symptoms that SHOULD BE assessed?
sputum
a mixture of saliva and mucus coughed up from the respiratory tract
accessory muscles
includes
sternocleidomastoid (aid in inspiration)
scalenes (neck)
abdominal muscles (aid in expiration)
dyspnea
air hunger, a nonpainful but uncomfortable awareness of breathing that is inappropriate to the level of exertion commonly termed “shortness of breath”
SERIOUS warrants full explanation & assessment
can result from pulmonary or cardiac disease
severity must be determined based on the patient’s ability to talk and complete daily activities
how must the severity of the patient’s dyspnea be determined?
pneumonia
pump failure (HF)
pulmonary embolism
possible foreign body (in airway)
pulmonary/bronchial constriction
pneumothorax
what are the 6P’s of dyspnea?
spontaneous pneumothorax
leakage of air into pleural space through blebs on visceral pleura with resulting partial or complete collapse of the lung
timing: sudden onset of dyspnea
associated symptoms: pleuritic pain, cough
wheezes
are musical respiratory high-pitched sounds that may be audible to the patient & others
caused by partial obstruction of the lower airways. the airway may be narrowed by bronchoconstriction, edema, secretions (asthma) or a foreign body
emphysema
they should be broad and open-ended, not specific. this allows patients to talk and provide more insight
when gathering health history how should questions be asked?
pneumocystis jiiroveci, pneumonia
Fever, dry nonproductive cough, and diminished breath sounds may indicate?
cystic fibrosis
tenacious sputum is seen in?
true
ACE inhibitors may produce a persistent dry cough as a side effect. T/F?
mucous membranes (lips, gums, around the eyes) and nails
In dark skinned individuals cyanosis may be easier to see in the?
tracheal deviation & fluid buildup
tracheal deviation happens because the fluid buildup causes enough pressure in the pleural space to push the trachea away from the side of the effusion, potentially indicating a large or clinically significant pleural effusion.
True
low oxygenation produces anxiety & restlessness. a decreased level of consciousness indicates poor oxygenation to the brain & other disease processes. T/F?
inspecting pt for signs of respiratory difficulty
observe facial expressions (relaxed & calm not anxious)
observe LOC
assess pt’s color for cyanosis (face & mucous membranes & nail beds)
listen to breathing sounds (wheezing, stridor)
inspect neck (see is accessory muscles are used)
observe shape of chest
pneumothorax, pleural effusion, or atelectasis
lateral displacement of the trachea may be seen in?
pneumothorax
during palpation (posterior chest examination), Unequal chest expansion, decreased or absent tactile fremitus, tracheal deviation to the unaffected side is associated with?
fremitus
refers to the palpable vibrations transmitted through the bronchopulmonary tree to the chest wall as the patient is speaking
helps assess the density and consistency of lung tissue
normal findings: should be equal & symmetrical vibrations felt on both sides
intensity is generally stronger over upper part of chest and weaker near the lower ribs
increased tactile fremitus
abnormal finding*** suggests that sound vibrations are transmitted more easily through the lung tissue, which can occur in conditions where the lung becomes denser or more consolidated
causes include unilateral pneumonia (consolidation of lung tissue, when air filled sacs become filled w/ fluid, cells or other substances in the alveoli causing lung tissue to become more solid)
decreased/absent tactile fremitus
suggests that sound vibrations are less effectively transmitted through the lung tissue, often because there is something preventing sound transmission (often seen with fluid or air in the pleural space)
causes include:
unilateral pleural effusion
pneumothorax
neoplasm from decreased transmission of low-frequency sounds
COPD, emphysema
percussion
produces audible sound, helps establish whether tissues are air-filled, fluid-filled or solid
Normal finding: should be RESONANT (hollow low-pitched sound) when tapped over air filled lung tissue NOT DULL
Dullness occurs when the lung tissue is less air-filled and more solid or fluid-filled such as in lobar pneumonia (dull) or pleural effusion (flat)
why is dullness an abnormal finding during percussion?
unaffected side
when there is a pneumothorax, the trachea deviates to the?
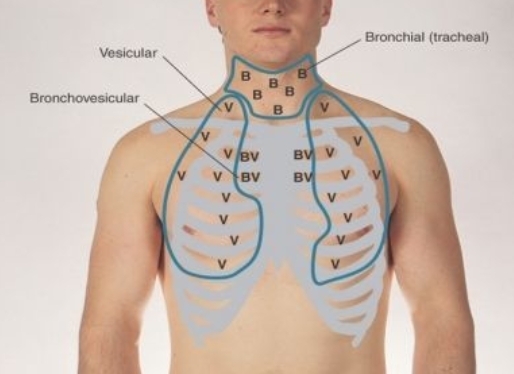
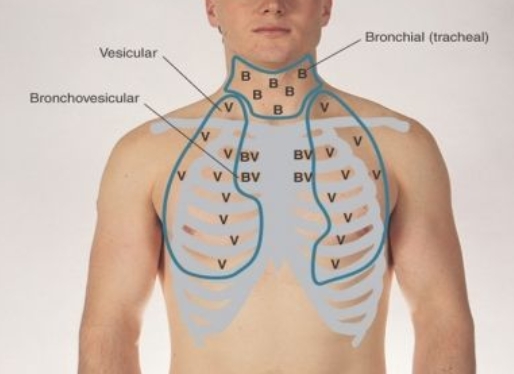
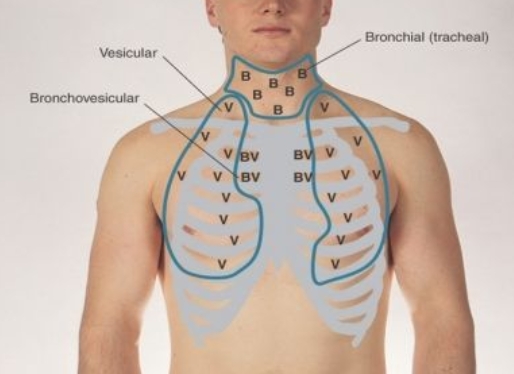
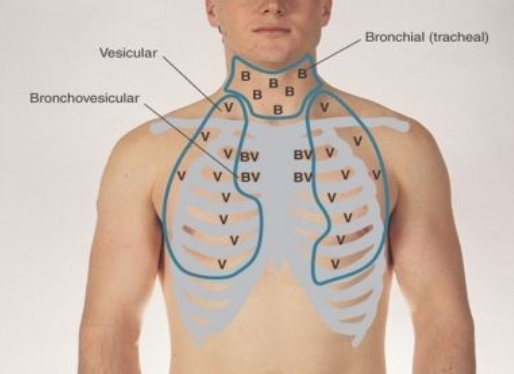
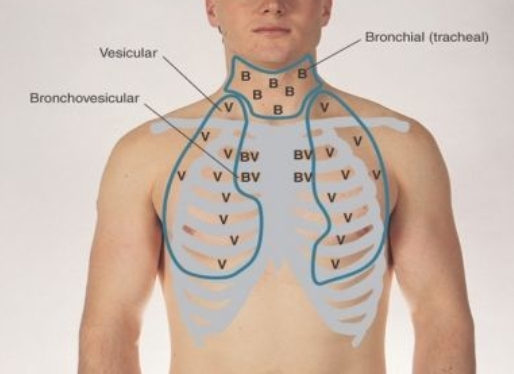
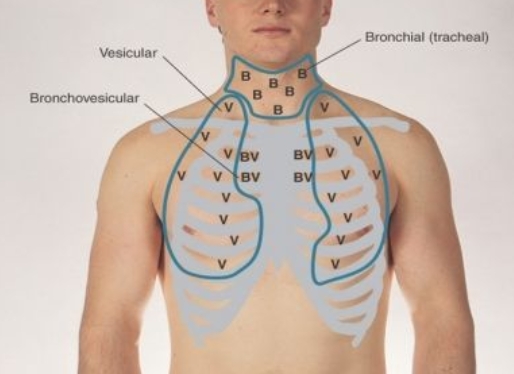
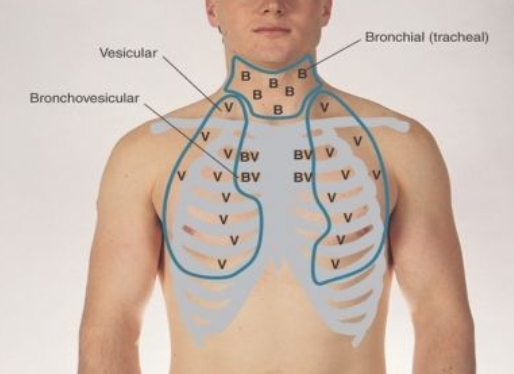
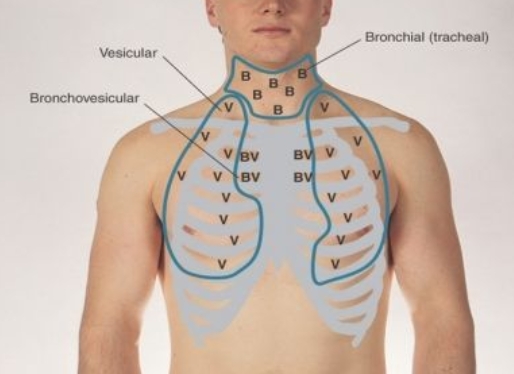
vesicular breath sounds
soft and low pitched
are heard throughout the periphery of the lungs. They are soft, low-pitched, rustling sounds.
bronchial breath sounds
are heard over the larynx, trachea, and posterior nape of the neck. They are high-pitched, hollow, tubular breath sounds.
bronchovesicular breath sounds
often heard in the first & second intercostal spaces anteriorly and between scapulae
are heard anteriorly over the mid-chest anterior intercostal spaces. These are medium-pitched sounds.
fine crackles
discontinuous nonmusical sounds
Intermittent, nonmusical, and brief
soft, higher pitched, & more frequent but brief 5-10 msec
EX:
Pneumonia
CHF
Pulmonary Fibrosis
Atelectasis
COPD
coarse crackles
somewhat louder, lower in pitch, brief (20 to 30 msec)
change or disappear with coughing and are transmitted through the mouth result from “boluses of gas passing through the airways as they open & close intermittently
EX:
Pneumonia
CHF
Pulmonary Fibrosis
Atelectasis
COPD
continuous, somewhat louder, lower in pitch, brief (20 to 30 msec)
wheezes and rhonchi are what type of sounds?
rhonchi
relative low pitched (≤200 Hz) with snoring quality, are a variant of wheezing but lower in pitch; may disappear with coughing; secretions are involved
EX: bronchitis, COPD
stridor
a continuous high-frequency, high pitched musical sound produced during airflow through a narrowing in the upper respiratory tract
best heard in the neck
causes of underlying airway obstruction include tracheal stenosis from intubation, airway edema after device removal, epiglottitis, foreign body, anaphylaxis & croup
pleural friction rub
a discontinuous, low frequency, grating sound that arises from inflammation & roughening the visceral pleura as it slides against the parietal pleura
“2 pieces of leather rubbing together”
best heard in axilla & base of lungs
egophony
when “ee” is heard as “ay”, an E-to-A change
is present indicates that the patient's lungs are consolidated (from pneumonia) or fluid-filled, or that the lung may have collapsed. It's most easily detected when comparing different areas of the lungs.
coronary artery disease
COPD mortality
lung cancer mortality
stroke
what are the adverse effects of smoking?
precontemplation
“I don’t want to quit.”
contemplation
“I am concerned but not ready to quit now.
preparation
“I am ready to quit.”
Action
“I just quit.”
maintenance
“I quit 6 months ago.”
S1
is the first heart sound heard and is made by the tricuspid and mitral valves closing.(lub)
S2
is the second heart sound heard and is made by the aortic and pulmonic valves closing. (dub)
SA Node
located in Right atrium, natural pacemaker of heart
AV node
located in atrial septum
bundle of HIS
located in ventricular myocardium
cardiac output
the amount of blood the heart pumps or ejects from each ventricle per minute usually 4-6L per minute
SV x HR = CO
stroke volume
the volume of blood ejected with each heartbeat
preload
refers to the load that stretches the cardiac muscle before contraction
myocardial contractility
refers to the ability of the cardiac muscle, when given a load, to contract or shorten
afterload
refers to the degree of vascular resistance to ventricular contraction
jugular venous pressure
refers to the pressure within the jugular veins, which are the veins that carry blood from the head and neck back to the heart
important clinical index of right heart pressures & function. reflects right atrial pressure which in turn equals central venous pressure
measured while pt is in semi-reclining position (30-45 degrees), will look for pulsations in internal jugular vein then compared to sternal angle
NORMAL JVP <3-4cm
True
JVP falls with loss of blood and increases with right or left heart failure, pulmonary hypertension, tricuspid stenosis, and pericardial compression or tamponade (abnormal accumulation of fluid between the layers of the pericardium which places pressure on the heart; if severe it impairs cardiac pumping function). T/F?
it causes decreased blood flow to the brain and induce syncope.
why should both carotids never be pressed at the same time?
if carotid has obstruction, kinking, or thrills
brachial artery should be assessed if?
flat
assessing JVP reflects pressure in the right atrium. starting point for HOB should be 30 degrees. when hypovolemic, HOB should be?
may need to be higher
assessing JVP reflects pressure in the right atrium. starting point for HOB should be 30 degrees. when hypervolemic, HOB should be?
diaphragm
is better for picking up the relatively high-pitched sounds of S1 and S2, the murmurs of aortic and mitral regurgitation, and pericardial friction rubs.
bell
is more sensitive to the low-pitched sounds of S3 and S4 and the murmur of mitral stenosis. Pressing the bell firmly on the chest makes it function more like the diaphragm by stretching the underlying skin
mitral murmurs, s3, s4, especially mitral stenosis
left lateral decubitus position accentuates?
aortic murmurs, soft diastolic murmur of aortic regurgitation may be missed if not listened to this position
Sitting Leaning Forward, exhale completely and stop breathing in expiration accentuates?
may indicate heart failure
inspect feet, ankles & legs (peripheral edema). Why?
metabolic syndrome
large waist circumference W: >35, M: >40
high blood pressure: >130, >85, undergoing Tx
high fasting blood sugar: >100mg/dL
high triglycerides: >150, or under Tx
low HDL: should be >40 Men, >50 Women
HTN modifications
salt intake <6g, 2300mg
3,500 mg of potassium
complete cessation of smoking
limit alcohol intake 1:W, 2:M
•Mushrooms
•Oranges and orange juice
•Peas
•Potatoes
•Prunes and prune juice
•Raisins and dates
•Spinach
•Tomatoes, tomato juice and tomato sauce
•Tuna
what are some foods rich in potassium?
malnutrition
Poverty (eating healthy is expensive), old age, social isolation, physical disability (is patient able to drive, can they cook, go shopping for food), emotional or mental impairment, lack of teeth, ill-fitting dentures, alcoholism, and drug abuse increase the likelihood of?
protein, vitamin C or Zinc deficiency
sore throat that won’t heal can be indicative of?
protein deficiency
edema (CV system) can be indicative of?
vitamin C or K deficiency
petechiae or ecchymosis can be indicative of?
kwashiorkor
is due to diets that may be high in calories but contain little or no protein
(e.g., low-protein liquid diets, fad diets, and long-term use of dextrose-containing intravenous fluids).
The serum albumin would be less than 3.5 g/dL.
right upper quadrant
ascending colon
duodenum
gallbladder
right kidney
liver
pancreas (head)
transverse colon
ureter (right)
right lower quadrant
appendix
ascending colon
cecum
rectum
ovary, uterus, fallopian tubes
prostate, spermatic cord
small intestine
ureter
left upper quadrant
descending colon
left kidney
pancreas (body & tail)
spleen
stomach
transverse colon
ureter (left)
left lower quadrant
parietal pain
originates from inflammation in the parietal peritoneum, also known as peritonitis. It is a steady, aching pain that is usually more severe than visceral pain and more precisely localized over the involved structure.
It is typically aggravated by movement or coughing.
Patients with parietal pain usually prefer to lie still.
referred pain
is felt in more distant sites, which are innervated at approximately the same spinal levels as the inflamed structures. this type of pain often develops as the initial pain becomes more intense and thus seems to radiate or travel from the initial site. It may be palpated superficially or deeply but is usually well localized.
Pain of duodenal or pancreatic origin may be referred to the back;
pain from the biliary tree, to the right scapular region or the right posterior thorax.
Pain from pleurisy or inferior wall myocardial infarction may be referred to the epigastric area.
dyspepsia
is a chronic or recurrent discomfort or pain centered in the upper abdomen which is characterized by postprandial fullness, early satiety, and epigastric pain or burning
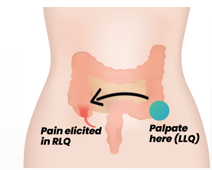
rovsing’s sign
Palpation of left lower abdomen causes pain in the right lower abdomen.
positive in appendicitis
psoas sign
is elicited by having the patient lie on his or her left side while the right thigh is flexed backward. Pain may indicate an inflamed appendix overlying the psoas muscle.
obturator sign
is a clinical sign of acute appendicitis, it is defined as discomfort felt by the subject/patient on the slow flexion & internal rotation of the hip joint, while the right knee is flexed. It indicates an inflamed pelvic appendix that is in contact with the obturator internus muscle
murphy’s sign
is elicited in patients with acute cholecystitis by asking the patient to take in and hold a deep breath while palpating the right subcostal area. If pain occurs when the inflamed gallbladder comes into contact with the examiner's hand, Murphy's sign is positive.
stress incontinence
For women, does sudden coughing, sneezing or laughing cause loss of urine? what is this referred to as?
urge incontinence
Detrusor contractions are stronger than normal and overcome the normal urethral resistance.
Hyperexcitability of sensory pathways, as in bladder infections, tumors, and fecal impaction
Deconditioning of voiding reflexes, as in frequent voluntary voiding at low bladder volume
overflow incontinence
Detrusor contractions are insufficient to overcome urethral resistance, causing urinary retention. The bladder is typically flaccid and large, even after an effort to void.
Obstruction of the bladder outlet, as in benign prostatic hyperplasia or tumor
Weakness of the detrusor muscle associated with peripheral nerve disease at S2–4 level
Impaired bladder sensation that interrupts the reflex arc, as in diabetic neuropathy
tympany
is a high pitched musical sound that indicates a hollow space filled by air or gas in the stomach or intestine.
heard during percussion
predominates because of GAS IN GI TRACT
dullness
fluid in solid or tissue organs
True
• Approximately 5% of normal adults only have a palpable spleen tip. Generally, the spleen is not palpable unless there is some pathology involved. T/F?
it may be enlarged, and palpation may cause it to rupture
why should you Never attempt to palpate the spleen after an accident?
bladder
•Normally cannot be examined unless it is distended above symphysis pubis
•Check for tenderness
•Percuss for dullness
Bladder volume must be 400 to 600 mL before dullness appears.
·Hardening of the arteries (atherosclerosis). Atherosclerosis occurs when fat and other substances build up on the lining of a blood vessel.
·High blood pressure. High blood pressure can damage and weaken the aorta's walls.
·Blood vessel diseases. ...Inherit connective tissue disorder
·Infection in the aorta. ...
·Trauma.
What are the most common causes of abdominal aneurysms?
patient breathes out around the bare abdomen at the level of the iliac crest
abdominal circumference with measuring tape should be taken when?
minute hemorrhagic spots in the skin which do not blanch with pressure. caused by blood leaking from capillaries under the skin
what is petechiae?