TYPE 2 DIABETES: TREATMENT
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
what are the aims of T2D treatment?
alleviate hyperglycaemic symptoms
improve glucose, lipids and BP
avoid excessive weight gain
improvement/ neutral impact on quality of life (no side effects)
reduce risk of hypoglycaemia
PREVENT LONG TERM COMPLICATIONS
how can T2D be treated?
non drug treatment and drug treatment
what non-drug treatment is used for T2D?
healthy eating
regular exercise
weight loss
smoking cessation
safe and sensible alcohol intake
what drug treatment can be used for T2D?
Oral or injectable
what are the classes of oral anti-diabetics?
biguanides, thiazolidinediones (glitazones), sodium glucose cotransporter-2 inhibitors (SGLT2’s), sulfonylureas, meglitinides (post-prandial regulators), DPP-4 inhibitors (gliptins), GLP-1 agonists (incretin mimetics), alpha-glucosidase inhibitors (acarbose)
what is the function of the oral anti-diabetics biguanides and thiazolidinediones (glitazones)?
sensitise body to insulin and/or decrease glucose production
how do sodium-glucose cotransporter-2 inhibitors (SGLT2s) work?
blocks glucose reabsorption in kidneys
how do sulfonylureas and meglitinides (post prandial regulators) work?
stimulates insulin production
how do DPP-4 inhibitors (gliptins) and GLP-1 agonists incretin mimetics) work?
target incretin system
how do alpha-glucosidase inhibitors (acarbose) work?
slow absorption of starch
what is the mechanism of action of biguanides?
sensitise the body to insulin and/or decrease glucose production for example metformin (only drug in class)
what are the key points for biguanides?
drug of choice in overweight patients
dose increased slowly to decrease risk of GI side effects
what is the mechanism of action of sodium-glucose cotransporter-2 inhibitors (SGLT2s)?
block glucose reabsorption in kidneys e.g. dapagliflozin and canagliflozin
what are key points with SGLT2 inhibitors?
effectiveness depends on kidney function
increased risk of urinary tract infection
what is the mechanism of action of sulfonylureas?
stimulate insulin production e.g. gliclazide and glibenclamide
what are the key points with sulfonylureas?
risk of hypoglycaemia
what is the mechanism of action with thiazolidinediones (glitazones)?
sensitise body to insulin and/or decrease glucose production e.g. pioglitazone (only drug in class)
what are the key points with thiazolidinediones (glitazones)?
should not be used in patients with heart failure or a history of heart failure
requires liver function monitoring
what is the mechanism of action of DPP-4 inhibitors (gliptins)?
target incretin system- block effect of enzyme DPP-4 (increased insulin secretion) e.g. alogliptin and vildagliptin
what are key points with DPP-4 inhibitors (gliptins)?
weight neutral
What is the mechanism of action of GLP-1 agonists (incretin mimetics)?
target incretin system: activate GLP-1 (increased insulin secretion) e.g. liraglutide, semaglutide
what are key points with GLP-1 agonists (incretin mimetics)?
SC injection
slight weight loss
increased risk of hypoglycaemia with sulfonylureas
what clinical evidence is there for treatment of type 2 diabetes?
UKPDS, >5000 newly diagnosed patients, median age is 54 years, lasted >20 years, median follow up 10 years
what was the aim of the UKPDS study?
to determine if intensive blood glucose control could reduce the risk of microvascular and macrovascular complications
additional sub trials helped determine the effect of tight vs less tight blood pressure control on the risk of macrovascular and microvascular complications
what treatment groups were involved in the UKPDS?
control group and intervention group
what was required from the control group in the UKPDS trial?
conventional therapy
dietary advice from dietician every three months
minimal drug treatment (if FPG >15mmol/L)
what was required from the intervention group in the UKPDS trial?
intensive therapy
dietary advice from dietician every three months
sulfonylurea or insulin treatment
what are the goals of treatment for the control group in the UKPDS trial?
FPG <15 mmol/L without symptoms of hypoglycaemia
what are the goals of treatment of the intervention group in the UKPDS trial?
FPG <6mmol/L
what is the pattern of incidence of complications from the UKPDS trial?
conventional treatment more likely to have an event
what is the pattern in median HBA1c and median FPG from the UKPDS trial?
conventional treatment has a higher HBA1c and FPG however both increase as time passes
what are the target HbA1c levels for diabetes managed by lifestyle/diet, or lifestyle/diet and single drug not associated with hypoglycaemia?
HbA1c: 48mmol/mol (6.5%)
what are the HbA1c target levels for drug associated with hypoglycaemia?
53mmol/mol (7.0%)
NICE algorithm for first line treatments
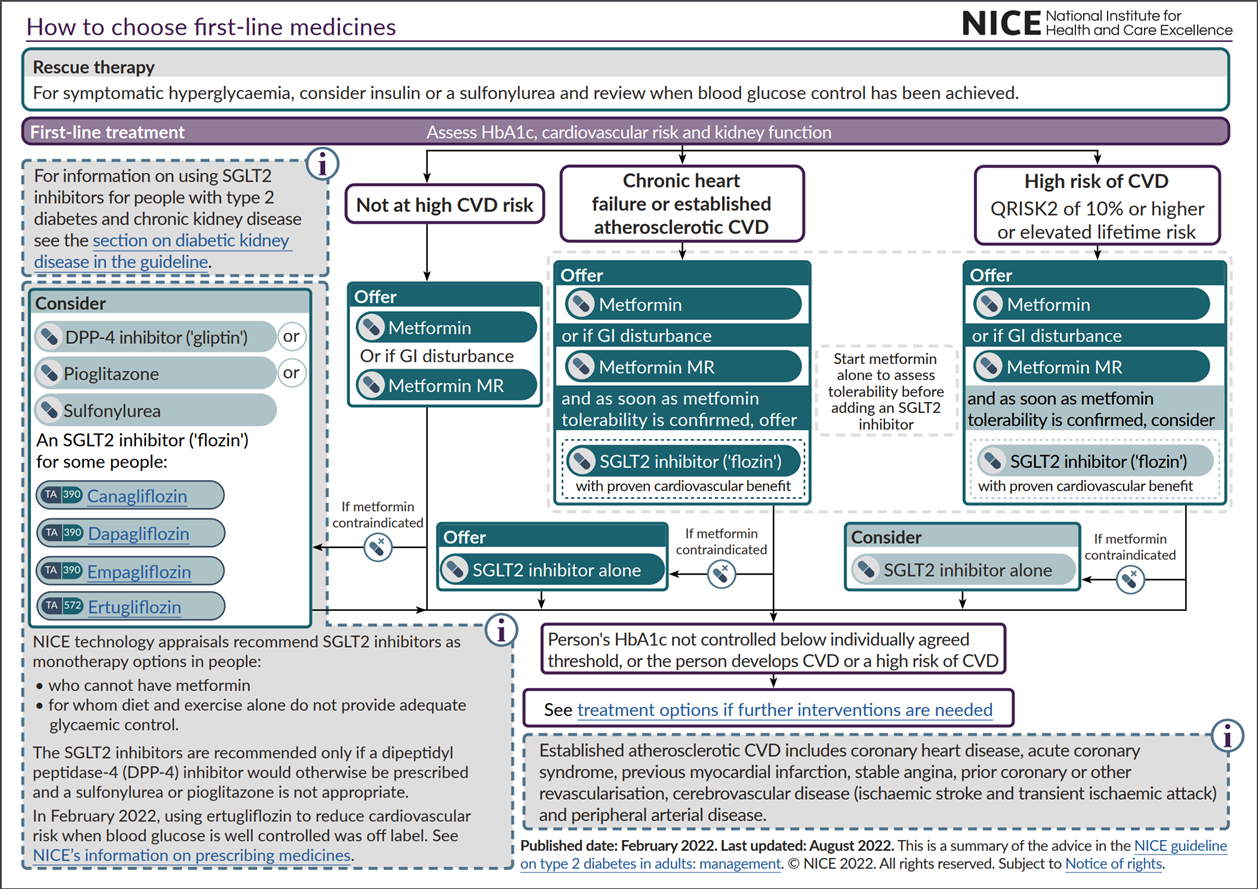
what must be identified when a person is being diagnosed with T2D?
identification of those with either atherosclerotic cardiovascular disease (ASCVD), chronic heart failure or high risk of CVD———→ at diagnosis and at subsequent reviews
what is high CVD risk defined as?
A QRISK2 score of >10% in adults aged 40 years and over, or
an elevated lifetime risk of CVD: defined as presence of one or more risk factors in someone <40 years
hypertension, dyslipidaemia, smoking, obesity and family history
what is the 1st line T2D treatment for people not at high CVD risk?
metformin (increase dose gradually)
metformin MR- if GI disturbance
IF metformin is c/i then give dpp-4 inhibitor, pioglitazone, sulfonylurea, SGLT2 inhibitor (alternative option to a DPP-4 inhibitor if neither a sulfonylurea or pioglitazone appropriate)
what is the first line T2D treatment for people with ASCVD, heart failure, high CVD risk?
metformin/ metformin MR
SGLT2 inhibitor (start as soon as tolerability to metformin is confirmed)
if metformin is c/i then give a SGLT2 inhibitor alone
NICE guidnace on how to choose medicines for further treatment options
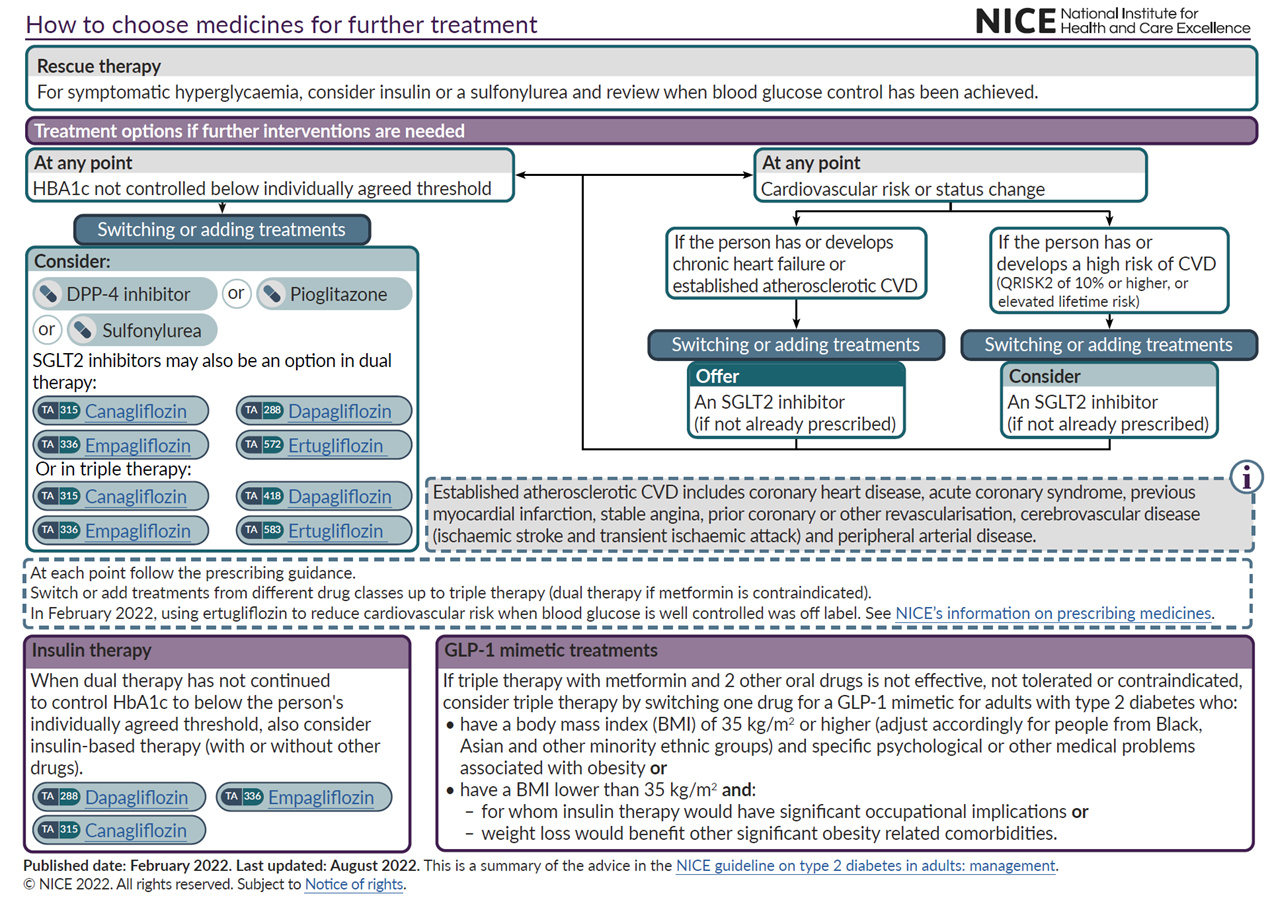
how should patients requiring further treatment be managed?
patients previously on metformin and not at high CVD risk
CVD risk or status changes then offer SGLT2 inhibitor (if not already prescribed)
when can dual therapy be considered?
if monotherapy with metformin is not controlling HbA1c band is below agreed threshold
what are the options for dual therapy?
metformin and a DPP-4 inhibitor
metformin and pioglitazone
metformin and sulfonylurea
metformin and SGLT2 inhibitor
what is triple therapy?
switch or add treatments from different drug classes, dual therapy if metformin is c/i, follow prescribing guidelines
what are examples of triple therapy?
metformin, sulfonylurea, DPP-4 inhibitor
metformin, sulfonylurea, SGLT2 inhibitor
metformin, sulfonylurea, pioglitazone
what are the NICE guidelines for GLP-1 receptor agonists for treating T2D?
If triple therapy with metformin and 2 other oral drugs is not effective/contraindicated/not tolerated: consider triple therapy
switch one drug for a GLP-1 mimetic
IF
BMI 35kg/m2 or higher
OR
BMI lower than 35kg/m2 and insulin therapy would have significant occupational implications
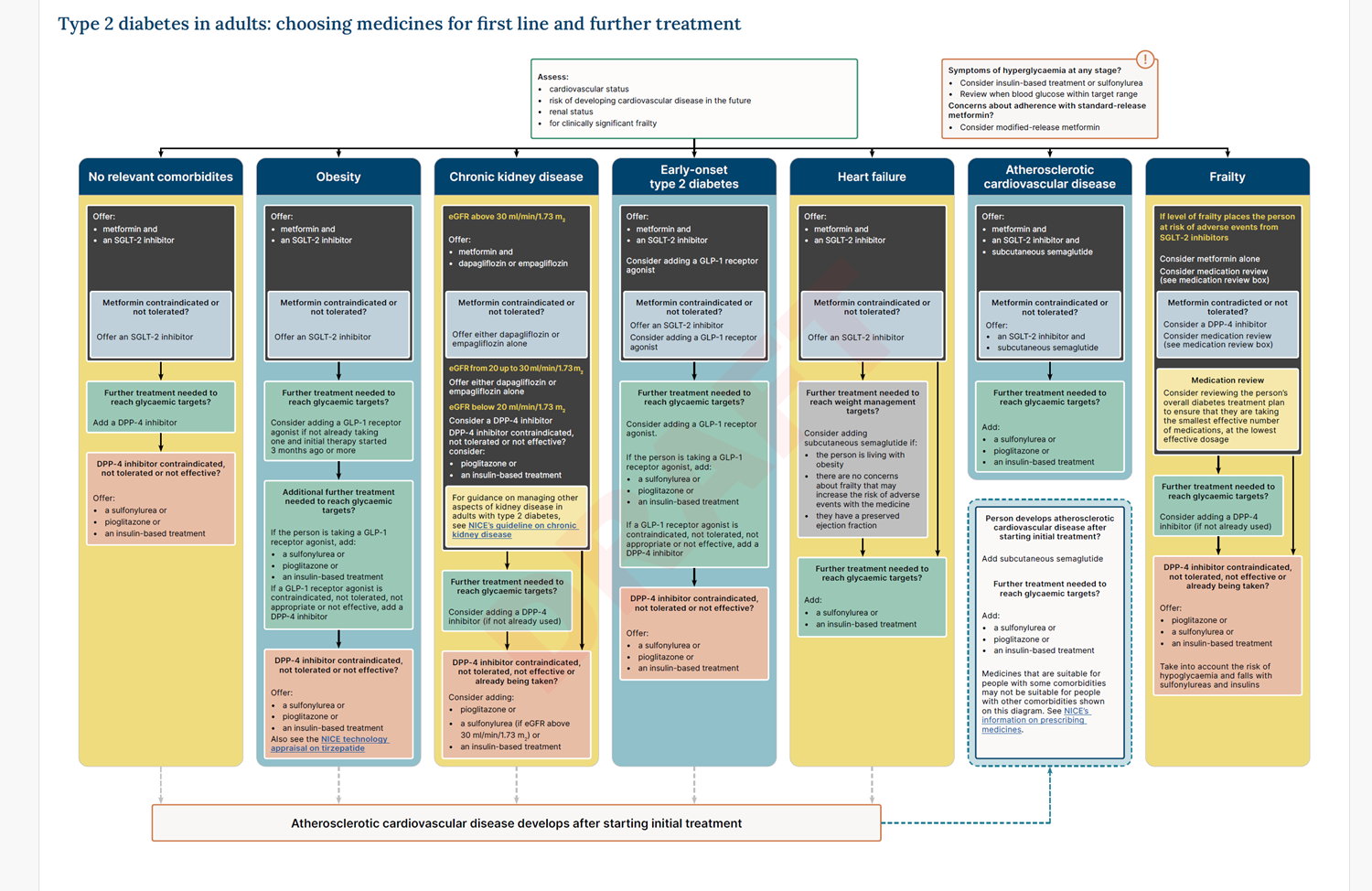
NICE draft guidelines for T2D
how much does insulin production decrease by each year?
around 5%, as patients age more insulin is required
when should patients with T2D be started on insulin?
dual therapy has not controlled HbA1c to below agreed threshold
metformin continued
other oral antidiabetics reviewed and stopped if necessary
what are some challenges experienced by insulin managed patients?
if the insulin dose is too high then the patinet may experience hypoglycaemia and weight gain, and HbA1c can become too low
how can insulin be given?
basal insulin injection at night or twice a day (human isophane insulin, prolonged action analogues)
biphasic insulin injected once or twice a day
intensive basal bolus
how is blood glucose monitored for patients not on insulin?
self monitoring only necessary for specific reasons
during periods of illness
when diabetes medication changed
patients troubled by hypoglycaemia
to monitor lifestyle changes e.g. weight loss, change of diet, exercise etc.
test twice on one day per week
how is blood glucose monitored for patients on insulin?
continuous glucose monitoring (CGM) should be offered to patients if certain conditions apply. for example
have recurrent or severe hypoglycaemia
have impaired hypoglycaemia awareness
unable to self-monitor by capillary glucose monitoring