Lewis - Ch 38 Heart Failure
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
While assessing a 68-yr-old with ascites, the nurse also notes jugular venous distention (JVD) with the head of the patient's bed elevated 45 degrees. The nurse knows this finding indicates
a. decreased fluid volume.
b. jugular vein atherosclerosis.
c. increased right atrial pressure.
d. incompetent jugular vein valves.
c. increased right atrial pressure.
The jugular veins empty into the superior vena cava and then into the right atrium, so JVD with the patient sitting at a 45-degree angle reflects increased right atrial pressure. JVD is an indicator of excessive fluid volume (increased preload), not decreased fluid volume. JVD is not caused by incompetent jugular vein valves or atherosclerosis.
DIF: Cognitive Level: Understand (comprehension) REF: 739
TOP: Nursing Process: Assessment MSC: NCLEX: Physiological Integrity
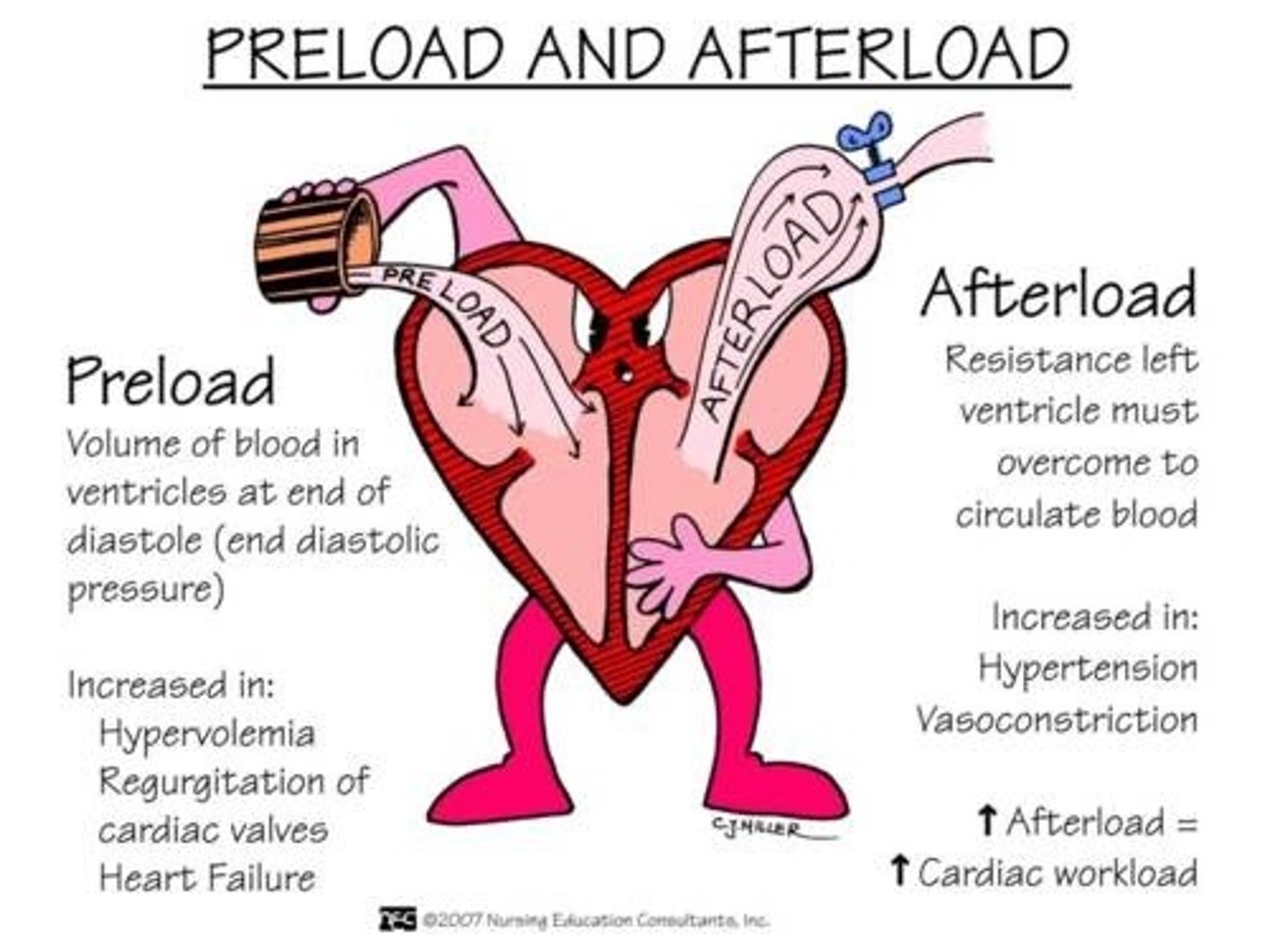
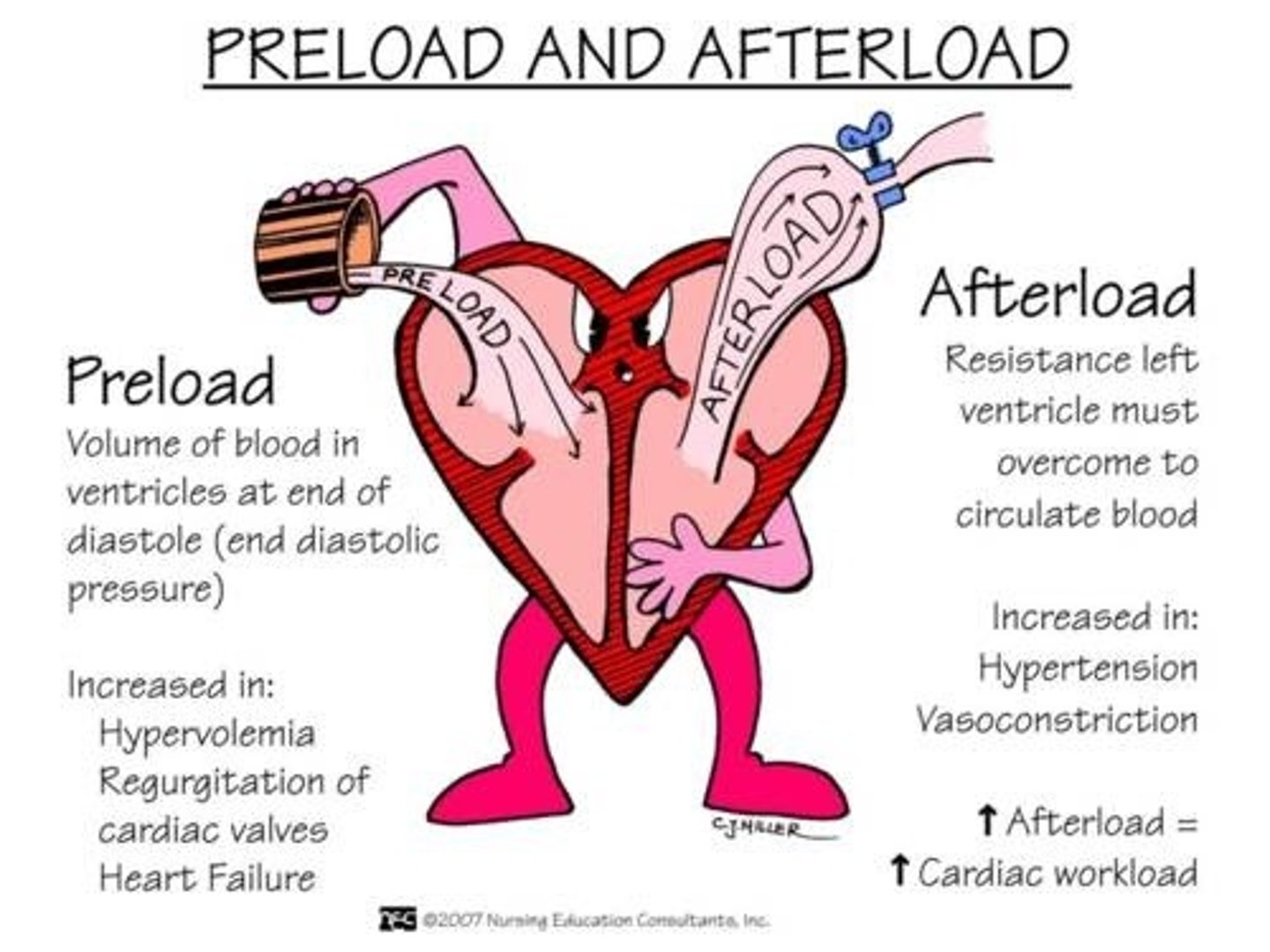
Preload/Afterload
The nurse is caring for a patient who is receiving IV furosemide (Lasix) and morphine for the treatment of acute decompensated heart failure (ADHF) with severe orthopnea. Which clinical finding is the best indicator that the treatment has been effective?
a. Weight loss of 2 lb in 24 hours
b. Hourly urine output greater than 60 mL
c. Reduction in patient complaints of chest pain
d. Reduced dyspnea with the head of bed at 30 degrees
d. Reduced dyspnea with the head of bed at 30 degrees
Because the patient's major clinical manifestation of ADHF is orthopnea (caused by the presence of fluid in the alveoli), the best indicator that the medications are effective is a decrease in dyspnea with the head of the bed at 30 degrees. The other assessment data may also indicate that diuresis or improvement in cardiac output has occurred but are not as specific to evaluating this patient's response.
Which topic will the nurse plan to include in discharge teaching for a patient with heart failure with reduced ejection fraction (HFrEF)?
a. Need to begin an aerobic exercise program several times weekly
b. Use of salt substitutes to replace table salt when cooking and at the table
c. Importance of making an annual appointment with the health care provider
d. Benefits and side effects of angiotensin-converting enzyme (ACE) inhibitors
d. Benefits and side effects of angiotensin-converting enzyme (ACE) inhibitors
The core measures for the treatment of heart failure established by The Joint Commission indicate that patients with an ejection fraction below 40% should receive an ACE inhibitor to decrease the progression of heart failure.
HFrEF (systolic failure) is the inability to pump blood effectively. Caused by:
- impaired contractile function
- increased afterload (HTN, peripheral vascular resistance)
- mechanical abnormalities
Decreased LV ejection fraction (LVEF) is <40% (can be seen on Echocardiogram)
(Adams lecture)
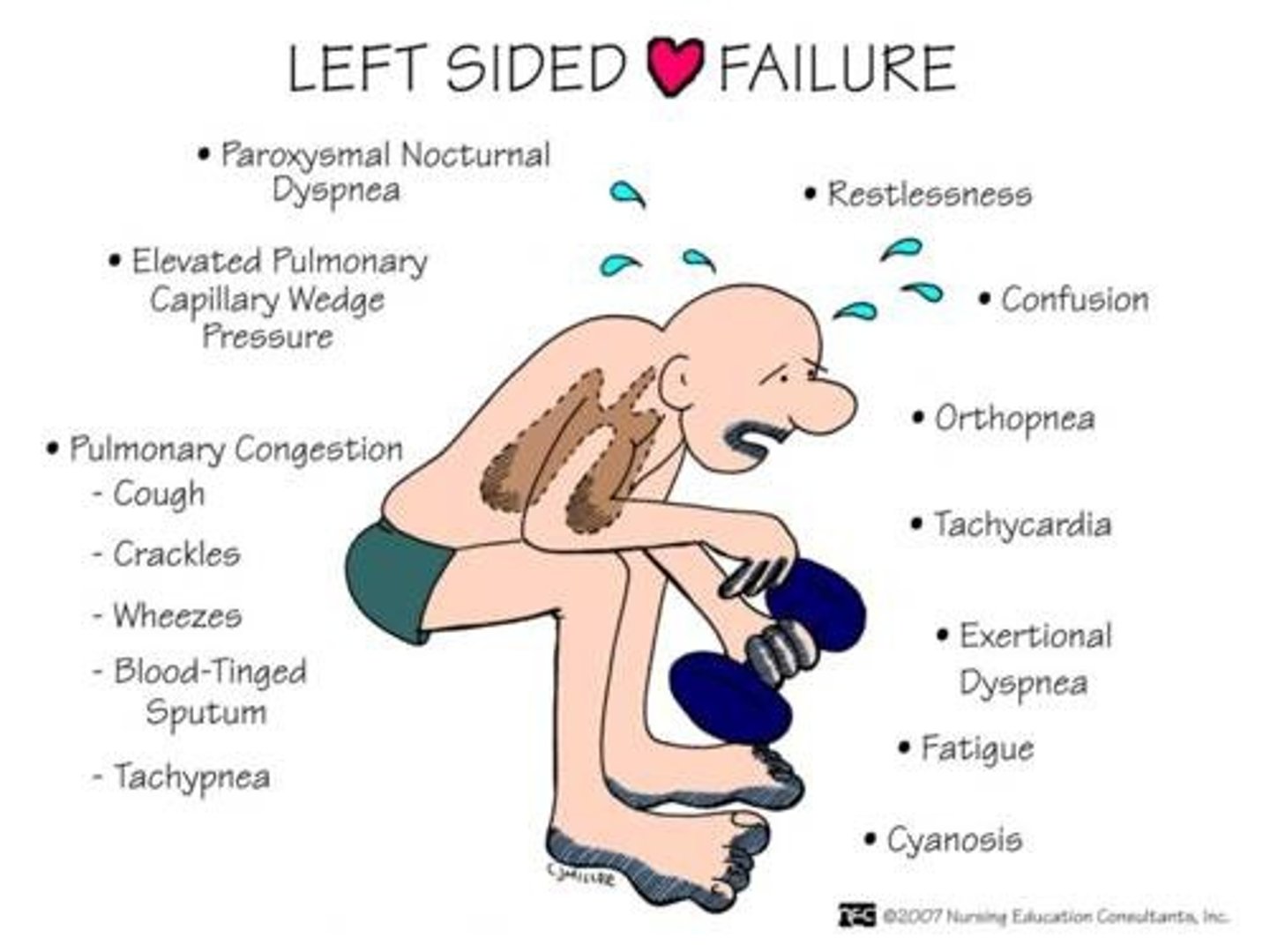
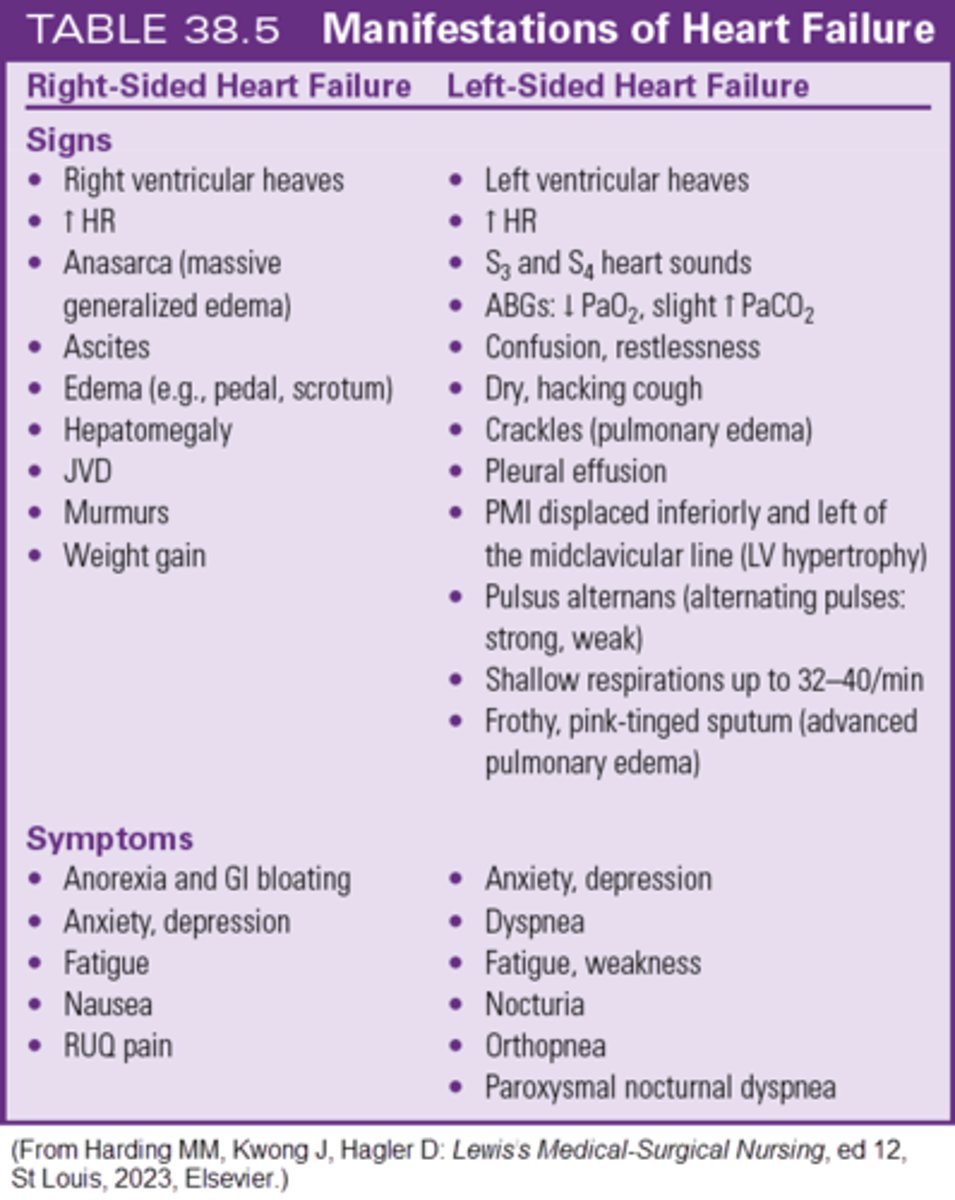
Left sided heart failure
Which assessment finding is consistent with right sided HF?
a. JVD
b. Presence of S3 and S4 heart sounds
c. Paroxysmal nocturnal dyspnea (PND)
d. Displacement of the point of maximal impulse (PMI)
a. JVD
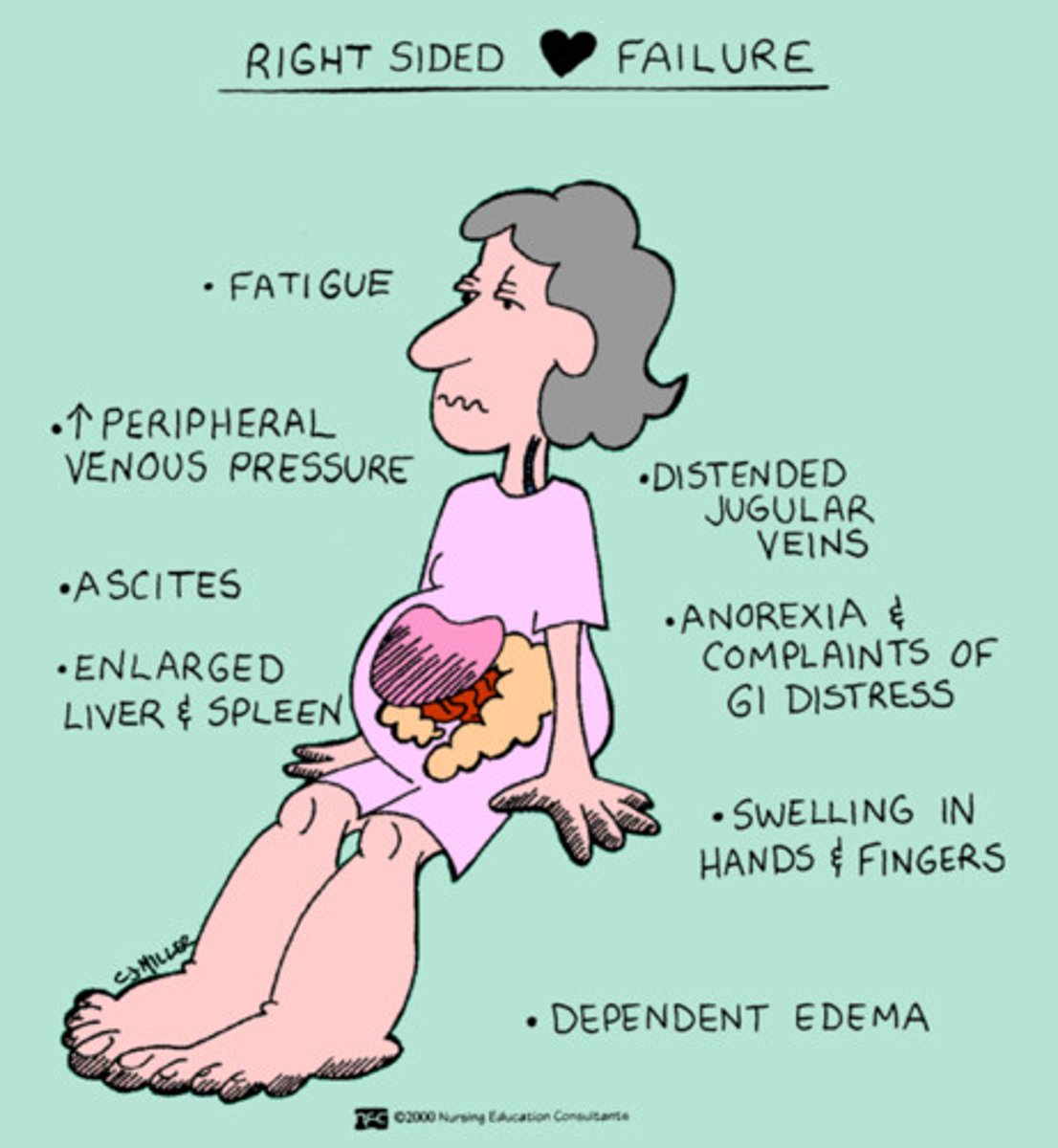
JVD is a sign of right sided HF. Right sided HF occurs when the right ventricle (RV) does not pump effectively. When the RV fails, fluid backs up into he venous system. Their causes movement of fluid into the tissues and organs (e.g., peripheral edema, abdominal ascites, hepatomegaly, JVD.)
The other choices are associated with left sided HF.
Pg. 862, 865
Right sided heart failure
RV does not pump effectively to the lungs
Fluid backs up into the venous system
Fluid moves into the tissues and organs (increase in JVD, ascites, peripheral edema)
Left sided HF is most common cause.
Other causes include RV infarction, PE, and Cor pulmonale (RV dilation and hypertorphy)
The nurse would monitor for which condition in a patient with left sided heart failure?
a. Pedal edema
b. Hepatomegaly
c. Splenomegaly
d. Pulmonary congestion
d. Pulmonary congestion
When the LV fails, blood backs up onto the left atrium (LA). This causes fluid accumulation in the lungs. The increased pulmonary hydrostatic pressure causes fluid leakage from the pulmonary capillary bed into the interstitial and then the alveoli. This results in pulmonary congestion and edema.
Right sided HF, which occurs when the right ventricle fails to contract effectively, causes pedal edema, hepatomegaly, and splenomegaly. Pg. 861
Biventricular Heart Failure
both ventricles fail, paroxysmal nocturnal dyspnea, dyspnea at rest, dysrhythmias, cardiogenic shock
Visual of HFpEF vs HFrEF
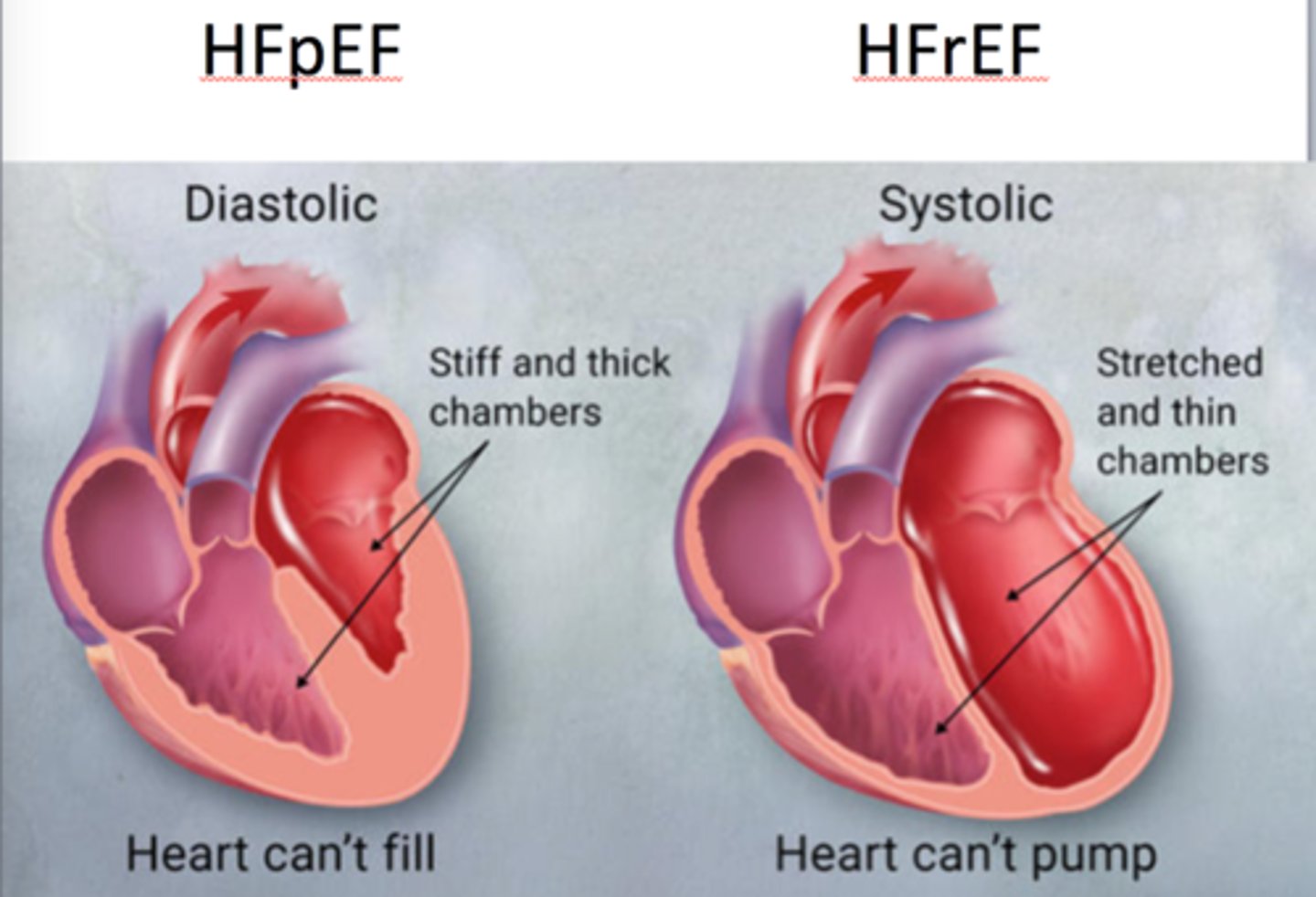
HFpEF (diastolic HF)
The inability of the ventricles to relax and fill during diastole, resulting in
IV sodium nitroprusside is ordered for a patient with acute pulmonary edema. During the first hours of administration, the nurse will need to titrate the nitroprusside rate down if the patient develops
a. ventricular ectopy.
b. a dry, hacking cough.
c. a systolic BP below 90 mm Hg.
d. a heart rate below 50 beats/min.
c. a systolic BP below 90 mm Hg.
Sodium nitroprusside is a potent direct acting vasodilator (reduces circulating blood volume) and the major adverse effect is severe hypotension.
Indication: For immediate reduction of blood pressure of patients in hypertensive crises, reduce bleeding during surgery, and for the treatment of acute congestive heart failure
ADHF Drug Therapy (Adams Lecture)
A patient who has chronic heart failure tells the nurse, "I was fine when I went to bed, but I woke up in the middle of the night feeling like I was suffocating!" The nurse will document this assessment finding as
a. orthopnea.
b. pulsus alternans.
c. paroxysmal nocturnal dyspnea.
d. acute bilateral pleural effusion.
c. paroxysmal nocturnal dyspnea.
Paroxysmal nocturnal dyspnea is caused by the reabsorption of fluid from dependent body areas when the patient is sleeping and is characterized by waking up suddenly with the feeling of suffocation. Pulsus alternans is the alteration of strong and weak peripheral pulses during palpation. Orthopnea indicates that the patient is unable to lie flat because of dyspnea. Pleural effusions develop over a longer time period.
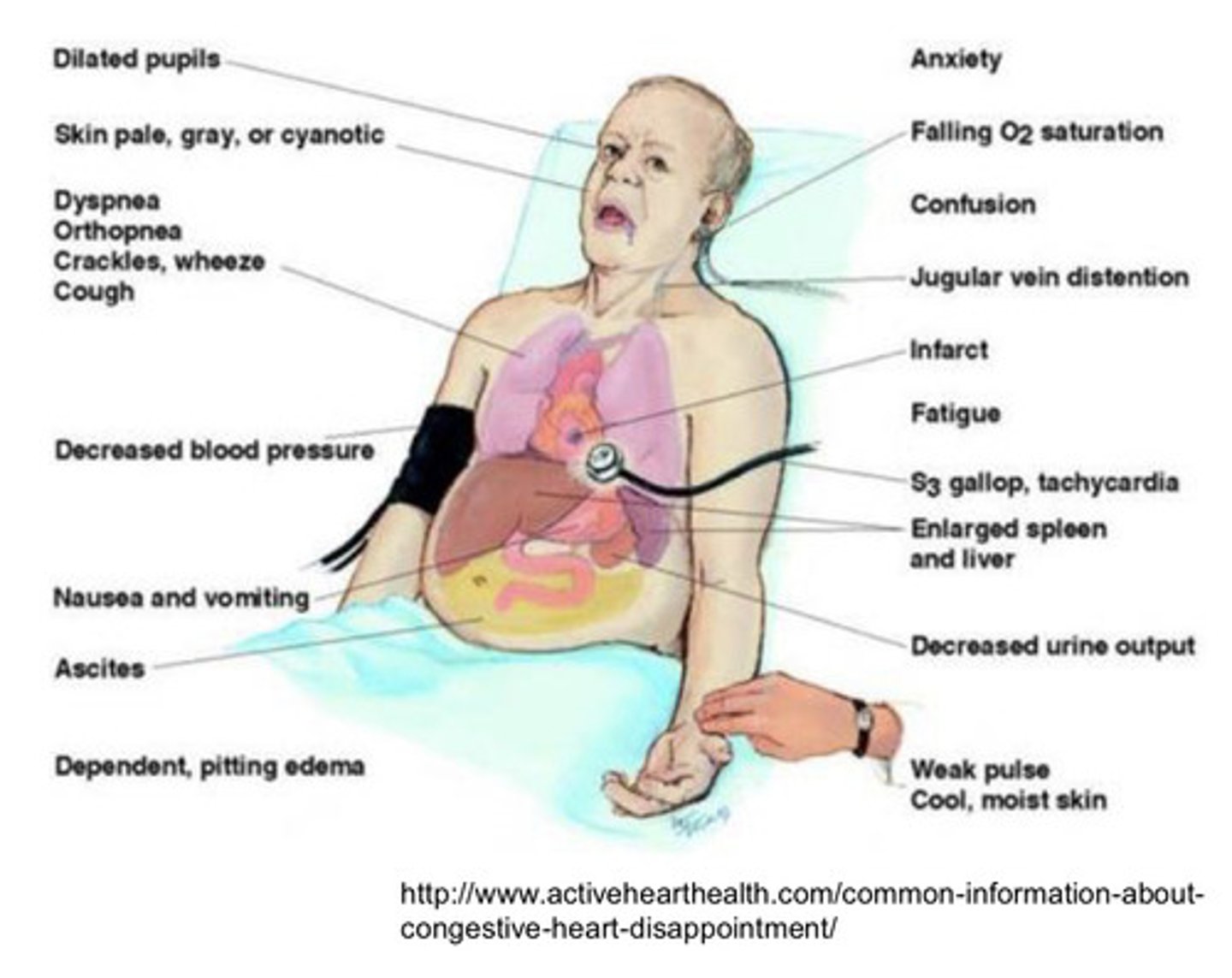
Clinical manifestations of ADHF (acute decompensated HF)
Increase (usually sudden) in symptoms of HF
Requires rapid escalation of therapy and hospitalization
Pulmonary edema (life threatening)
SOB, orthopnea, JFD, tachypnea, crackles
Clinical manifestations of HF
Chronic from HTN, develops overtime, progressive
Fatigue (from lack of cardiac output)
Dyspnea (orthopnea, PND)
Cough (chronic, nonproductive)
Tachycardia, Palpitaions (may come from Afib- most common in HF)
Edema
Decreased Urinary Output
Skin (gray, mottled)
Mental Status (dizziness, light headed, syncope)
weight changes up or down
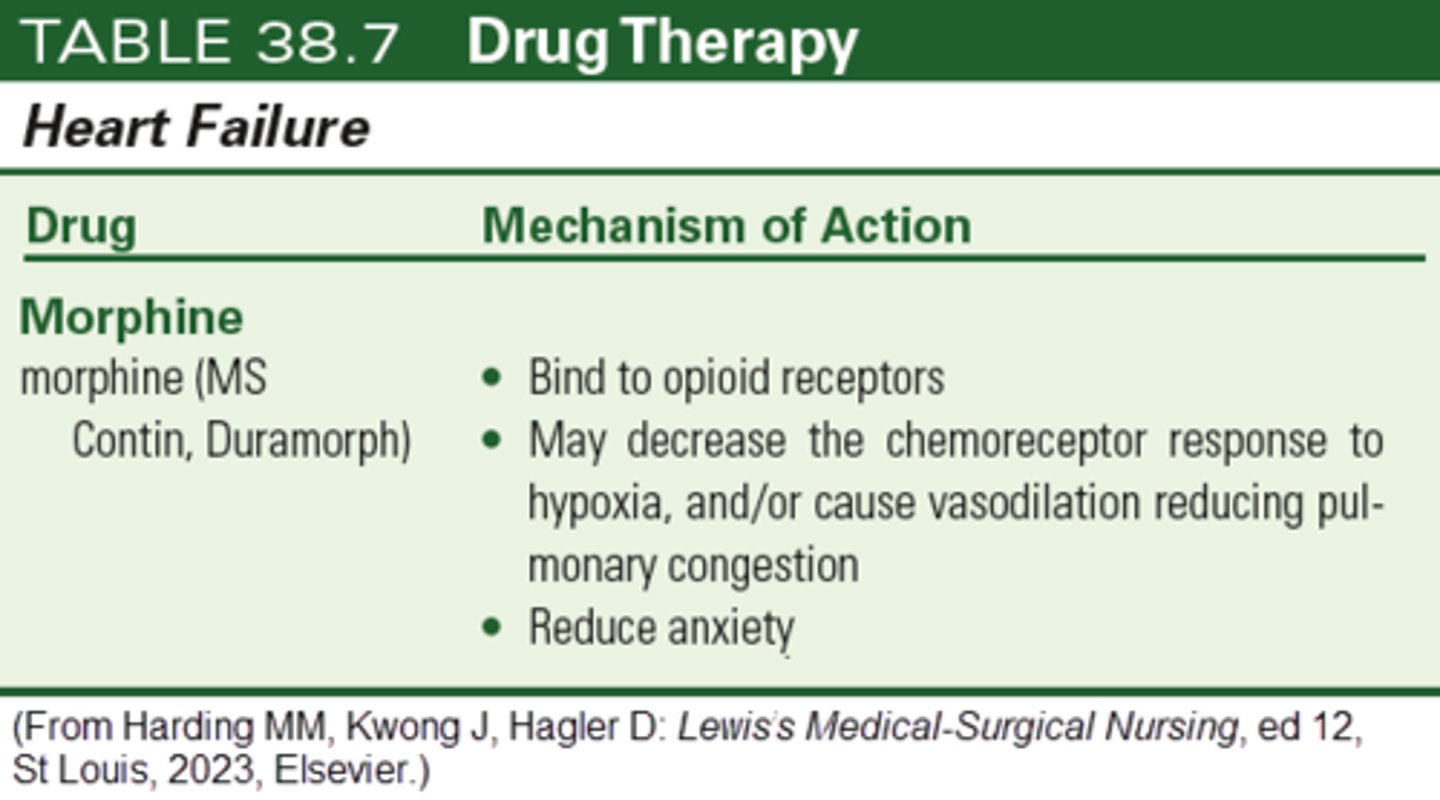
The nurse anticipates that which medication will be prescribed for a patient with HF who experience severe anxiety during dyspneic episodes?
a. Digoxin
b. Morphine
c. Dopamine
d. Metolazone
b. Morphine
Morphine is an opioid analgesic used to both reduce anxiety and treat HF. It may decrease the chemoreceptor response to hypoxia and/or cause vasodilation, reducing pulmonary congestion.
Digoxin is a cardiac glycoside and is used to increase cardiac contractility.
Dopamine is a positive inotrope that is used to treat HF.
Metolzaone is a thiazide like diuretic that is used to treat HF. Pg. 869
During a visit to a 78-yr-old patient with chronic heart failure, the home care nurse finds that the patient has ankle edema, a 2-kg weight gain over the past 2 days, and complains of "feeling too tired to get out of bed." Based on these data, a correct nursing diagnosis for the patient is
a. activity intolerance related to fatigue.
b. impaired skin integrity related to edema.
c. disturbed body image related to weight gain.
d. impaired gas exchange related to dyspnea on exertion.
a. activity intolerance related to fatigue.
The patient's statement supports the diagnosis of activity intolerance. There are no data to support the other diagnoses, although the nurse will need to assess for additional patient problems.
The nurse working on the heart failure unit knows that teaching an older female patient with newly diagnosed heart failure is effective when the patient states that
a. she will take furosemide (Lasix) every day at bedtime.
b. the nitroglycerin patch is to be used when chest pain develops.
c. she will call the clinic if her weight goes up 3 pounds in 1 week.
d. an additional pillow can help her sleep if she is short of breath at night.
c. she will call the clinic if her weight goes up 3 pounds in 1 week.
Teaching for a patient with heart failure includes information about the need to weigh daily and notify the health care provider about an increase of 3 lb in 2 days or 3 to 5 lb in a week.
- Nitroglycerin patches are used primarily to reduce preload (not to prevent chest pain) in patients with heart failure and should be used daily, not on an "as needed" basis.
- Diuretics should be taken earlier in the day to avoid nocturia and sleep disturbance.
- The patient should call the clinic if increased orthopnea develops rather than just compensating by further elevating the head of the bed.
When teaching the patient with newly diagnosed heart failure about a 2000-mg sodium diet, the nurse explains that foods to be restricted include
a. canned and frozen fruits.
b. yogurt and milk products.
c. fresh or frozen vegetables.
d. eggs and other high-protein foods.
ANS B
Yogurt and milk products (e.g., cheese) naturally contain a significant amount of sodium, and the intake of these should be limited for patients on a diet that limits sodium to 2000 mg daily. The other foods listed have minimal levels of sodium and can be eaten without restriction.
DIF: Cognitive Level: Apply (application) REF: 749
TOP: Nursing Process: Implementation MSC: NCLEX: Physiological Integrity
The nurse plans discharge teaching for a patient with chronic heart failure who has prescriptions for digoxin (Lanoxin) and hydrochlorothiazide. Appropriate instructions for the patient include
a. limit dietary sources of potassium.
b. take the hydrochlorothiazide before bedtime.
c. notify the health care provider if nausea develops.
d. take the digoxin if the pulse is below 60 beats/min.
c. notify the health care provider if nausea develops.
Nausea is a sign of digoxin toxicity and should be reported to the HCP so that digoxin levels can be checked, and prescription adjusted if needed.
- The patient will need to include potassium-containing foods in the diet to avoid hypokalemia.
- Patients should be taught to check their pulse daily before taking the digoxin and if the pulse is less than 60 beats/min, to call their provider before taking the digoxin.
- Diuretics should be taken early in the day to avoid sleep disruption.
While admitting an 82-yr-old patient with acute decompensated heart failure to the hospital, the nurse learns that the patient lives alone and sometimes confuses the "water pill" with the "heart pill." When planning for the patient's discharge the nurse will facilitate a
a. plan for around-the-clock care.
b. consultation with a psychologist.
c. transfer to a long-term care facility.
d. referral to a home health care agency.
ANS D
The data about the patient suggest that assistance in developing a system for taking medications correctly at home is needed. A home health nurse will assess the patient's home situation and help the patient develop a method for taking the two medications as directed. There is no evidence that the patient requires services such as a psychologist consult, long-term care, or around-the-clock home care.
DIF: Cognitive Level: Apply (application) REF: 752
TOP: Nursing Process: Planning MSC: NCLEX: Physiological Integrity
Following an acute myocardial infarction, a previously healthy 63-yr-old develops clinical manifestations of heart failure. The nurse anticipates discharge teaching will include information about
a. Adrenergic blockers.
b. calcium channel blockers.
c. digitalis and potassium therapy regimens.
d. angiotensin-converting enzyme (ACE) inhibitors.
d. angiotensin-converting enzyme (ACE) inhibitors.
ACE inhibitor therapy is currently recommended to prevent the development of heart failure in patients who have had a myocardial infarction and as a first-line therapy for patients with chronic heart failure.
- Digoxin therapy for heart failure is no longer considered a first-line measure, and digoxin is added to the treatment protocol when therapy with other drugs such as ACE-inhibitors, diuretics, and -adrenergic blockers is insufficient.
- Calcium channel blockers are not generally used in the treatment of heart failure.
- The -adrenergic blockers are not used as initial therapy for new onset heart failure.
A 53-yr-old patient with stage D heart failure and type 2 diabetes asks the nurse whether heart transplant is a possible therapy. Which response by the nurse is most accurate?
a. "Your heart failure has not reached the end stage yet."
b. "You could not manage the multiple complications of that surgery."
c. "The suitability of a heart transplant for you depends on many factors."
d. "Because you have diabetes, you would not be a heart transplant candidate."
ANS C
Indications for a heart transplant include end-stage heart failure (stage D), but other factors such as coping skills, family support, and patient motivation to follow the rigorous posttransplant regimen are also considered. Patients with diabetes who have well-controlled blood glucose levels may be candidates for heart transplant. Although heart transplants can be associated with many complications, there are no data to suggest that the patient could not manage the care.
DIF: Cognitive Level: Apply (application) REF: 753
TOP: Nursing Process: Implementation MSC: NCLEX: Physiological Integrity
Which diagnostic test will be most useful to the nurse in determining whether a patient admitted with acute shortness of breath has heart failure?
a. Serum troponin
b. Arterial blood gases
c. B-type natriuretic peptide
d. 12-lead electrocardiogram
c. B-type natriuretic peptide
B-type natriuretic peptide (BNP) is secreted when ventricular pressures increase, as they do with heart failure. Elevated BNP indicates a probable or very probable diagnosis of heart failure. A 12-lead electrocardiogram, arterial blood gases, and troponin may also be used in determining the causes or effects of heart failure but are not as clearly diagnostic of heart failure as BNP.
-BNP levels (substance that is released in the blood when the heart stretches because it is holding excess fluid- correlates with left ventricular dysfunction), higher number worse it is:
-under 100 HF highly improbable
-100-500 HF probable
-over 500 HF highly probable
(Adams lecture)
Diagnostic Studies for HF
We want to determine and treat the underlying cause
-echo first- ultrasound of heart- shows EF, provides info on LVEF, heart valves, presence of effusion or thrombus
- ECG, ambulatory heart monitors, chest X-ray, 6 minute walk test, MUGA scan, Cardiac MRI, cardiopulmonary exercise stress test, cardiac catheterization/ angiogram, EMB
-BNP levels (substance that is released in the blood when the heart stretches because it is holding excess fluid- correlates with left ventricular dysfunction), higher number worse it is:
-under 100 HF highly improbable
-100-500 HF probable
-over 500 HF highly probable
Which action should the nurse include in the plan of care when caring for a patient admitted with acute decompensated heart failure (ADHF) who is receiving nesiritide (Natrecor)?
a. Monitor blood pressure frequently.
b. Encourage patient to ambulate in room.
c. Titrate nesiritide slowly before stopping.
d. Teach patient about home use of the drug.
a. Monitor blood pressure frequently.
Nesiritide is a potent arterial and venous dilator, and the major adverse effect is hypotension. Because the patient is likely to have orthostatic hypotension, the patient should not be encouraged to ambulate. Nesiritide does not require titration and is used for ADHF but not in a home setting.
Nesiritide (vasodilator, reduces circulating blood volume) is a medication used to treat acutely decompensated congestive heart failure with dyspnea at rest or with minimal exertion (such as talk, eating or bathing).
Adams lecture
15. A patient with heart failure has a new order for captopril 12.5 mg PO. After giving the first dose and teaching the patient about the drug, which statement by the patient indicates that teaching has been effective?
a. "I will be sure to take the medication with food."
b. "I will need to eat more potassium-rich foods in my diet."
c. "I will call for help when I need to get up to use the bathroom."
d. "I will expect to feel more short of breath for the next few days."
c. "I will call for help when I need to get up to use the bathroom."
Captopril (ACE) can cause hypotension, especially after the initial dose, so it is important that the patient not get up out of bed without assistance until the nurse has had a chance to evaluate the effect of the first dose.
- The angiotensin-converting enzyme (ACE) inhibitors are potassium sparing, and the nurse should not teach the patient to purposely increase sources of dietary potassium.
- Increased shortness of breath is expected with the initiation of -adrenergic blocker therapy for heart failure, not for ACE inhibitor therapy.
- ACE inhibitors are best absorbed when taken an hour before eating.
16. A patient who has just been admitted with pulmonary edema is scheduled to receive the following medications. Which medication should the nurse question before giving?
a. captopril 25 mg
b. furosemide (Lasix) 60 mg
c. digoxin (Lanoxin) 0.125 mg
d. carvedilol (Coreg) 3.125 mg
d. carvedilol (Coreg) 3.125 mg
Although carvedilol is appropriate for the treatment of chronic heart failure, it is not used for patients with acute decompensated heart failure (ADHF) because of the risk of worsening the heart failure. The other drugs are appropriate for the patient with ADHF.
A patient with a history of chronic heart failure is admitted to the emergency department with severe dyspnea and a dry, hacking cough. Which action should the nurse do first?
a. Auscultate the abdomen.
b. Check the capillary refill.
c. Auscultate the breath sounds.
d. Ask about the patient's allergies.
c. Auscultate the breath sounds.
This patient's severe dyspnea and cough indicate that acute decompensated heart failure (ADHF) is occurring. ADHF usually manifests as pulmonary edema, which should be detected and treated immediately to prevent ongoing hypoxemia and cardiac/respiratory arrest. The other assessments will provide useful data about the patient's volume status and also should be accomplished rapidly, BUT detection (and treatment) of pulmonary complications is the priority.
GOALS OF THERAPY
- Relieving symptoms
- Optimizing volume status
- Supporting oxygenation, ventilation, cardio output, and end organ perfusion
- identifying and addressing causes
- avoiding complicaitons
- teaching related to HF exacerbations
- Planning discharge
(Adams lecture)
Assessing/ Monitoring the patient with ADHF includes
- Ongoing monitoring and assessment of
*VS, O2 sat, Wt (best indicator of fluid status), mentation (AOx4 assessment), ECGs (looking for Afib, PVC, Vtach), indicators of volume overload (JVD, edema, wt. gain)
- place patient in High Fowler’s
-Hemodynamic monitoring if unstable
- Supplemental O2, BiPaP
- Mechanical ventilation if unstable- if cant get their O2 sat over 90, we are intubating
(Adams lecture)
A patient with chronic heart failure who is taking a diuretic and an angiotensin-converting enzyme (ACE) inhibitor and who is on a low-sodium diet tells the home health nurse about a 5-lb weight gain in the past 3 days. The nurse's priority action will be to
a. have the patient recall the dietary intake for the past 3 days.
b. ask the patient about the use of the prescribed medications.
c. assess the patient for clinical manifestations of acute heart failure.
d. teach the patient about the reduced sodium diet
c. assess the patient for clinical manifestations of acute heart failure.
The 5-lb weight gain over 3 days indicates that the patient's chronic heart failure may be worsening. It is important that the patient be assessed immediately for other clinical manifestations of decompensation, such as lung crackles.
- A dietary recall to detect hidden sodium in the diet, reinforcement of sodium restrictions, and assessment of medication compliance may be appropriate interventions but are not the first nursing actions indicated.
Adams lecture
A patient in the intensive care unit with acute decompensated heart failure (ADHF) complains of severe dyspnea and is anxious, tachypneic, and tachycardic. Several drugs have been ordered for the patient. The nurse's priority action will be to
a. give PRN IV morphine sulfate 4 mg.
b. give PRN IV diazepam (Valium) 2.5 mg.
c. increase nitroglycerin infusion by 5 mcg/min.
d. increase dopamine infusion by 2 mcg/kg/min.
a. give PRN IV morphine sulfate 4 mg.
Morphine improves alveolar gas exchange, improves cardiac output by reducing ventricular preload and afterload, decreases SOB and anxiety, and assists in reducing the subjective feeling of dyspnea. (Adams lecture)
- Diazepam may decrease patient anxiety, but it will not improve the cardiac output or gas exchange.
- Increasing the dopamine may improve cardiac output, but it will also increase the heart rate and myocardial oxygen consumption.
- Nitroglycerin will improve cardiac output and may be appropriate for this patient, but it will not directly reduce anxiety and will not act as quickly as morphine to decrease dyspnea.
ADHF Drug Therapy: Diuretics, vasodilators, Morphine, Positive Inotropes
Diuretics
- decreases volume overload (preload)
- watch potassium and magnesium levels
Vasodilators
- Reduces circulating blood volume
- IV nitroglycerin, IV sodium nitropursside, IV nesiritide
Morphine
- Reduces preload and afterload, relieves SOB and anxiety
Positive inotropes- Vasopressors
- Increases contractility
- dobutamine, dopamine, digalis, digoxin
Main Treatment goals for CHRONIC HF
Main Treatment Goals
- Treat the underlying cause and contributing factors
- Maximize Cardiac Output
- Improve quality of life
Oxygen Therapy
- relieves dyspnea and fatigue
Physical and emotional rest
- conserve energy and decrease oxygen needs
Structured exercise program
- Cardiac Rehab associated with better outcomes
After receiving change-of-shift report on four patients admitted to a heart failure unit, which patient should the nurse assess first?
a. A patient who reported dizziness after receiving the first dose of captopril
b. A patient who is cool and clammy, with new-onset confusion and restlessness
c. A patient who has crackles bilaterally in the lung bases and is receiving oxygen.
d. A patient who is receiving IV nesiritide (Natrecor) and has a blood pressure of 100/62
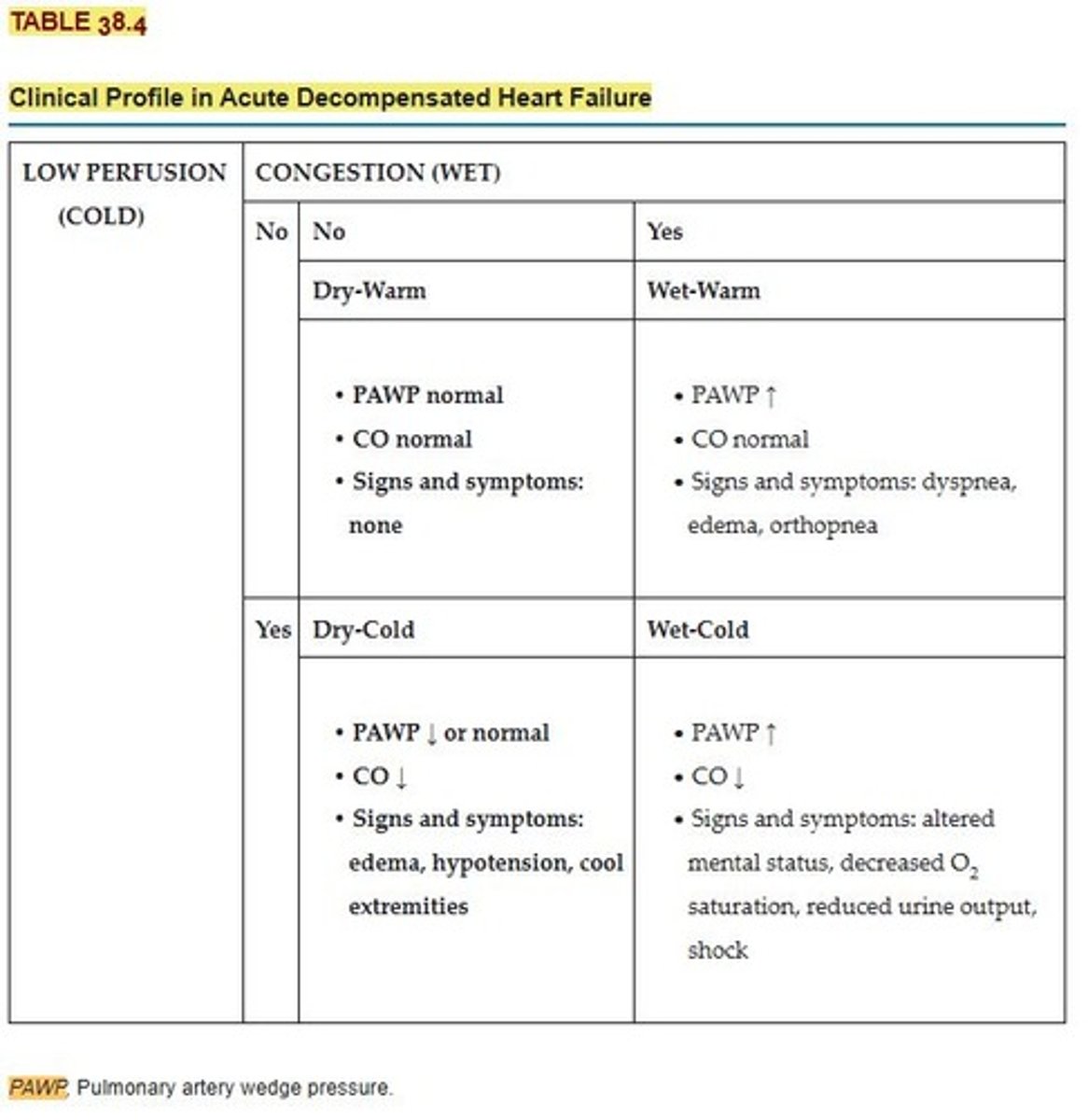
b. A patient who is cool and clammy, with new-onset confusion and restlessness
The patient who has "wet-cold" clinical manifestations of heart failure is perfusing inadequately and needs rapid assessment and changes in management. The other patients also should be assessed as quickly as possible but do not have indications of severe decreases in tissue perfusion.
Which assessment finding in a patient admitted with acute decompensated heart failure (ADHF) requires the most immediate action by the nurse?
a. O2 saturation of 88%
b. Weight gain of 1 kg (2.2 lb)
c. Heart rate of 106 beats/min
d. Urine output of 50 mL over 2 hours
a. O2 saturation of 88%
A decrease in O2 saturation to less than 92% indicates hypoxemia, and the nurse should start supplemental O2 immediately. An increase in apical pulse rate, 1-kg weight gain, and decreases in urine output also indicate worsening heart failure and require nursing actions, but the low O2 saturation rate requires the most immediate nursing action.
A patient has recently started on digoxin (Lanoxin) in addition to furosemide (Lasix) and captopril for the management of heart failure. Which assessment finding by the home health nurse is a priority to communicate to the health care provider?
a. Presence of 1+ to 2+ edema in the feet and ankles
b. Palpable liver edge 2 cm below the ribs on the right side
c. Serum potassium level 3.0 mEq/L after 1 week of therapy
d. Weight increase from 120 pounds to 122 pounds over 3 days
c. Serum potassium level 3.0 mEq/L after 1 week of therapy
Loop diuretics, such as furosemide, are widely used to reduce fluid overload in patients and are well known for their renal K-wasting effects that often produce hypokalemia.
Hypokalemia can predispose the patient to life-threatening dysrhythmias (e.g., premature ventricular contractions) and potentiate the actions of digoxin. Hypokalemia also increases the risk for digoxin toxicity, which can also cause life-threatening dysrhythmias.
The other data indicate that the patient's heart failure requires more effective therapies, but they do not require nursing action as rapidly as the low serum potassium level.
(Adams lecture)
An outpatient who has chronic heart failure returns to the clinic after 2 weeks of therapy with metoprolol (Toprol XL). Which assessment finding is most important for the nurse to report to the health care provider?
a. 2+ bilateral pedal edema
b. Heart rate of 56 beats/min
c. Complaints of increased fatigue
d. Blood pressure (BP) of 88/42 mm Hg
d. Blood pressure (BP) of 88/42 mm Hg
The patient's BP indicates that the dose of metoprolol may need to be decreased because of hypotension.
Bradycardia is a frequent adverse effect of -adrenergic blockade, but the rate of 56 is not unusual though it may need to be monitored. -Adrenergic blockade initially will worsen symptoms of heart failure in many patients and patients should be taught that some increase in symptoms, such as fatigue and edema, is expected during the initiation of therapy with this class of drugs.
Drug Therapy for Chronic HF
RAAS inhibitors
- ACE inhibitors
** "prils"
- Angiotensin II receptor blockers (ARBS)
** "artans"
- Neprilysin-angiotensin receptor inhibitors
- Aldosterone antagonists
** monitor potassium levels (hyperkalemia)
- B-adrenergic blockers
** carvedilol (Coreg), metoprolol- watch for hypotension
- Vasodilators- monitor BP, dizziness, take time standing
- Combination therapy
- Positive inotropic agents
** Digitalis, Digoxin (normals blood levels- 2mcg per mL is toxic- see low hr, nausea and vomiting) Digibind is the antidote)
A patient who is receiving dobutamine for the treatment of acute decompensated heart failure (ADHF) has the following nursing interventions included in the plan of care. Which action will be most appropriate for the registered nurse (RN) to delegate to an experienced licensed practical/vocational nurse (LPN/LVN)?
a. Teach the patient the reasons for remaining on bed rest.
b. Change the peripheral IV site according to agency policy.
c. Monitor the patient's blood pressure and heart rate ever
d. Adjust the drip rate on the pump
ANS C
An experienced LPN/LVN would be able to monitor BP and heart rate and would know to report significant changes to the RN. Teaching patients, making adjustments to the drip rate for vasoactive drugs, and inserting a new peripheral IV catheter require RN level education and scope of practice.
DIF: Cognitive Level: Apply (application) REF: 745
OBJ: Special Questions: Delegation TOP: Nursing Process: Planning
MSC: NCLEX: Safe and Effective Care Environment
25. After receiving change-of-shift report on a heart failure unit, which patient should the nurse assess first?
a. Patient who is taking carvedilol (Coreg) and has a heart rate of 58
b. Patient who is taking digoxin and has a potassium level of 3.1 mEq/L
c. Patient who is taking captopril and has a frequent nonproductive cough
d. Patient who is taking isosorbide dinitrate/hydralazine (BiDil) and has a headache
ANS B
The patient's low potassium level increases the risk for digoxin toxicity and potentially life-threatening dysrhythmias. The nurse should assess the patient for other signs of digoxin toxicity and then notify the health care provider about the potassium level. The other patients also have side effects of their drugs, but their symptoms do not indicate potentially life-threatening complications.
DIF: Cognitive Level: Analyze (analysis) REF: 748
OBJ: Special Questions: Prioritization | Special Questions: Multiple Patients
TOP: Nursing Process: Assessment MSC: NCLEX: Safe and Effective Care Environment
The home care nurse visits a 73-year-old Hispanic woman with chronic heart failure. Which clinical manifestations, if assessed by the nurse, would indicate acute decompensated heart failure (pulmonary edema)?
A. Fatigue, orthopnea, and dependent edema
B. Severe dyspnea and blood-streaked, frothy sputum
C. Temperature is 100.4o F and pulse is 102 beats/minute
D. Respirations 26 breaths/minute despite oxygen by nasal cannula
B. Severe dyspnea and blood-streaked, frothy sputum
Clinical manifestations of pulmonary edema include anxiety, pallor, cyanosis, clammy and cold skin, severe dyspnea, use of accessory muscles of respiration, a respiratory rate > 30 breaths per minute, orthopnea, wheezing, and coughing with the production of frothy, blood-tinged sputum. Auscultation of the lungs may reveal crackles, wheezes, and rhonchi throughout the lungs. The heart rate is rapid, and blood pressure may be elevated or decreased.
A 54-year-old male patient who had bladder surgery 2 days ago develops acute decompensated heart failure (ADHF) with severe dyspnea. Which action by the nurse would be indicated first?
A. Perform a bladder scan to assess for urinary retention.
B. Restrict the patient's oral fluid intake to 500 mL per day.
C. Assist the patient to a sitting position with arms on the overbed table.
D. Instruct the patient to use pursed-lip breathing until the dyspnea subsides
C. Assist the patient to a sitting position with arms on the overbed table.
The nurse should place the patient with ADHF in a high Fowler's position with the feet horizontal in the bed or dangling at the bedside. This position helps decrease venous return because of the pooling of blood in the extremities. This position also increases the thoracic capacity, allowing for improved ventilation. Pursed-lip breathing helps with obstructive air trapping but not with acute pulmonary edema. Restricting fluids takes considerable time to have an effect.
A 70-year-old woman with chronic heart failure and atrial fibrillation asks the nurse why warfarin (Coumadin) has been prescribed for her to continue at home. Which response by the nurse is accurate?
A. "The medication prevents blood clots from forming in your heart."
B. "The medication dissolves clots that develop in your coronary arteries."
C. "The medication reduces clotting by decreasing serum potassium levels."
D. "The medication increases your heart rate so that clots do not form in your
A. "The medication prevents blood clots from forming in your heart."
Chronic heart failure causes enlargement of the chambers of the heart and an altered electrical pathway, especially in the atria. When numerous sites in the atria fire spontaneously and rapidly, atrial fibrillation occurs. Atrial fibrillation promotes thrombus formation within the atria with an increased risk of stroke and requires treatment with cardioversion, antidysrhythmics, and/or anticoagulants. Warfarin is an anticoagulant that interferes with hepatic synthesis of vitamin K-dependent clotting factors.
The nurse prepares to administer digoxin (Lanoxin) 0.125 mg to an 82-year-old man admitted with influenza and a history of chronic heart failure. What should the nurse assess before giving the medication?
A. Prothrombin time
B. Urine specific gravity
C. Serum potassium level
D. Hemoglobin and hematocrit
C. Serum potassium level
Serum potassium should be monitored because hypokalemia increases the risk for digoxin toxicity. Changes in prothrombin time, urine specific gravity, and hemoglobin or hematocrit would not require holding the digoxin dose.
At a clinic visit, the nurse provides dietary teaching for a 56-year-old woman who was recently hospitalized with an exacerbation of chronic heart failure. The nurse determines that teaching is successful if the patient makes which statement?
A. "I will limit the amount of milk and cheese in my diet."
B. "I can add salt when cooking foods but not at the table."
C. "I will take an extra diuretic pill when I eat a lot of salt."
D. "I can have unlimited amounts of foods labeled as reduced sodium."
A. "I will limit the amount of milk and cheese in my diet."
Milk products should be limited to 2 cups per day for a 2500-mg sodium-restricted diet. Salt should not be added during food preparation or at the table. Diuretics should be taken as prescribed (usually daily) and not based on sodium intake. Foods labeled as reduced sodium contain at least 25% less sodium than regular.
The nurse is administering a dose of digoxin (Lanoxin) to a patient with heart failure (HF). The nurse would become concerned with the possibility of digitalis toxicity if the patient reported which symptom(s)?
A. Muscle aches
B. Constipation
C. Pounding headache
D. Anorexia and nausea
D. Anorexia and nausea
Anorexia, nausea, vomiting, blurred or yellow vision, and cardiac dysrhythmias are all signs of digitalis toxicity. The nurse would become concerned and notify the health care provider if the patient exhibited any of these symptoms.
The nurse is preparing to administer digoxin to a patient with heart failure. In preparation, laboratory results are reviewed with the following findings: sodium 139 mEq/L, potassium 5.6 mEq/L, chloride 103 mEq/L, and glucose 106 mg/dL. What should the nurse do next?
A. Withhold the daily dose until the following day.
B. Withhold the dose and report the potassium level.
C. Give the digoxin with a salty snack, such as crackers.
D. Give the digoxin with extra fluids to dilute the sodium level.
B. Withhold the dose and report the potassium level.
The normal potassium level is 3.5 to 5.0 mEq/L. The patient is hyperkalemic, which makes the patient more prone to digoxin toxicity. For this reason, the nurse should withhold the dose and report the potassium level. The physician may order the digoxin to be given once the potassium level has been treated and decreases to within normal range.
An intraaortic balloon pump (IABP) is being used for a patient who is in cardiogenic shock. Which data would indicate to the nurse that the goals of IABP treatment are being met?
a. Urine output of 25 mL/hr
b. Heart rate of 110 beats/min
c. Cardiac output (CO) of 5 L/min
d. Stroke volume (SV) of 40 mL/beat
c. Cardiac output (CO) of 5 L/min
CO of 5 L/min is normal and indicates that the IABP has been successful in treating the
shock. The low SV signifies continued cardiogenic shock. The tachycardia and low urine
output also suggest continued cardiogenic shock.
The nurse is caring for a patient who has an intraaortic balloon pump in place. Which action would the nurse include in the plan of care?
a. Avoid the use of anticoagulant medications.
b. Monitor the patient's urinary output every hour.
c. Provide passive range of motion for all extremities.
d. Position the patient supine with head flat at all times
b. Monitor the patient's urinary output every hour.
Monitoring urine output will help determine whether the patient's cardiac output has
improved. It also will help assess for balloon displacement blocking the renal arteries. The
head of the bed can be elevated up to 30 degrees. Heparin is used to prevent thrombus
formation. Limited movement is allowed for the extremity with the balloon insertion site to
prevent displacement of the balloon
While waiting for heart transplantation, a patient with severe cardiomyopathy has a ventricular assist device (VAD) implanted. Which action would the nurse include in the plan of care for this patient?
a. Preparing the patient for a permanent VAD
b. Teaching the patient the reason for bed rest
c. Monitoring the incision for signs of infection
d. Administering immunosuppressants medications
c. Monitoring the incision for signs of infection
The insertion site for the VAD provides a source for transmission of infection to the
circulatory system and requires frequent monitoring. Patients with VADs can have some
mobility and may not be on bed rest. The VAD is a bridge to transplantation, not a permanent
device. Immunosuppression is not necessary for nonbiologic devices such as the VAD.
What is the priority assessment by the nurse caring for a patient receiving IV nesiritide (Natrecor) to treat heart failure?
A. Urine output
B. Lung sounds
C. Blood pressure
D. Respiratory rate
C. Blood pressure
Although all identified assessments are appropriate for a patient receiving IV nesiritide, the priority assessment would be monitoring for hypotension, the main adverse effect of nesiritide.
A patient admitted with heart failure appears very anxious and complains of shortness of breath. Which nursing actions would be appropriate to alleviate this patient's anxiety (select all that apply)?
A. Administer ordered morphine sulfate.
B. Position patient in a semi-Fowler's position.
C. Position patient on left side with head of bed flat.
D. Instruct patient on the use of relaxation techniques.
E. Use a calm, reassuring approach while talking to patient.
A. Administer ordered morphine sulfate.
B. Position patient in a semi-Fowler's position.
D. Instruct patient on the use of relaxation techniques.
E. Use a calm, reassuring approach while talking to patient.
Morphine sulfate reduces anxiety and may assist in reducing dyspnea. The patient should be positioned in semi-Fowler's position to improve ventilation that will reduce anxiety. Relaxation techniques and a calm reassuring approach will also serve to reduce anxiety.
A male patient with a long-standing history of heart failure has recently qualified for hospice care. What measure should the nurse now prioritize when providing care for this patient?
A. Taper the patient off his current medications.
B. Continue education for the patient and his family.
C. Pursue experimental therapies or surgical options.
D. Choose interventions to promote comfort and prevent suffering.
D. Choose interventions to promote comfort and prevent suffering.
The central focus of hospice care is the promotion of comfort and the prevention of suffering. Patient education should continue, but providing comfort is paramount. Medications should be continued unless they are not tolerated. Experimental therapies and surgeries are not commonly used in the care of hospice patients.
What should the nurse recognize as an indication for the use of dopamine (Intropin) in the care of a patient with heart failure?
A. Acute anxiety
B. Hypotension and tachycardia
C. Peripheral edema and weight gain
D. Paroxysmal nocturnal dyspnea (PND)
B. Hypotension and tachycardia
Dopamine is a β-adrenergic agonist whose inotropic action is used for treatment of severe heart failure accompanied by hemodynamic instability. Such a state may be indicated by tachycardia accompanied by hypotension. PND, anxiety, edema, and weight gain are common signs and symptoms of heart failure, but these do not necessarily warrant the use of dopamine.
A patient with a recent diagnosis of heart failure has been prescribed furosemide (Lasix) in an effort to physiologically do what for the patient?
A. Reduce preload.
B. Decrease afterload.
C. Increase contractility.
D. Promote vasodilation.
A. Reduce preload.
Diuretics such as furosemide are used in the treatment of HF to mobilize edematous fluid, reduce pulmonary venous pressure, and reduce preload. They do not directly influence afterload, contractility, or vessel tone.
A patient with a diagnosis of heart failure has been started on a nitroglycerin patch by his primary care provider. What should this patient be taught to avoid?
A. High-potassium foods
B. Drugs to treat erectile dysfunction
C. Nonsteroidal antiinflammatory drugs
D. Over-the-counter H2-receptor blockers
B. Drugs to treat erectile dysfunction
The use of erectile drugs concurrent with nitrates creates a risk of severe hypotension and possibly death. High-potassium foods, NSAIDs, and H2-receptor blockers do not pose a risk in combination with nitrates.
A stable patient with acute decompensated heart failure (ADHF) suddenly becomes dyspneic. Before positioning the patient on the bedside, what should the nurse assess first?
A. Urine output
B. Heart rhythm
C. Breath sounds
D. Blood pressure
D. Blood pressure
The nurse should evaluate the blood pressure before dangling the patient on the bedside because the blood pressure can decrease as blood pools in the periphery and preload decreases. If the patient's blood pressure is low or marginal, the nurse should put the patient in the semi-Fowler's position and use other measures to improve gas exchange.
The patient has heart failure (HF) with an ejection fraction of less than 40%. What core measures should the nurse expect to include in the plan of care for this patient (select all that apply)?
A. Left ventricular function is documented.
B. Controlling dysrhythmias will eliminate HF.
C. Prescription for digoxin (Lanoxin) at discharge
D. Prescription for angiotensin-converting enzyme (ACE) inhibitor at discharge
E. Education materials about activity, medications, weight monitoring, and what to
A. Left ventricular function is documented.
D. Prescription for angiotensin-converting enzyme (ACE) inhibitor at discharge
E. Education materials about activity, medications, weight monitoring, and what to do if symptoms worsen
The Joint Commission has identified these three core measures for heart failure patients. Although controlling dysrhythmias will improve CO and workload, it will not eliminate HF. Prescribing digoxin for all HF patients is no longer done because there are newer effective drugs and digoxin toxicity occurs easily related to electrolyte levels and the therapeutic range must be maintained.
After having an MI, the nurse notes the patient has jugular venous distention, gained weight, developed peripheral edema, and has a heart rate of 108/minute. What should the nurse suspect is happening?
A. ADHF
B. Chronic HF
C. Left-sided HF
D. Right-sided HF
D. Right-sided HF
An MI is a primary cause of heart failure. The jugular venous distention, weight gain, peripheral edema, and increased heart rate are manifestations of right-sided heart failure.
Beyond the first year after a heart transplant, the nurse knows that what is a major cause of death?
A. Infection
B. Acute rejection
C. Immunosuppression
D. Cardiac vasculopathy
D. Cardiac vasculopathy
Beyond the first year after a heart transplant, malignancy (especially lymphoma) and cardiac vasculopathy (accelerated CAD) are the major causes of death. During the first year after transplant, infection and acute rejection are the major causes of death. Immunosuppressive therapy will be used for posttransplant management to prevent rejection and increases the patient's risk of an infection.
The patient with chronic heart failure is being discharged from the hospital. What information should the nurse emphasize in the patient's discharge teaching to prevent progression of the disease to ADHF?
A. Take medications as prescribed.
B. Use oxygen when feeling short of breath.
C. Only ask the physician's office questions.
D. Encourage most activity in the morning when rested.
A. Take medications as prescribed.
The goal for the patient with chronic HF is to avoid exacerbations and hospitalization. Taking the medications as prescribed along with nondrug therapies such as alternating activity with rest will help the patient meet this goal. If the patient needs to use oxygen at home, it will probably be used all the time or with activity to prevent respiratory acidosis. Many HF patients are monitored by a care manager or in a transitional program to assess the patient for medication effectiveness and monitor for patient deterioration and encourage the patient. This nurse manager can be asked questions or can contact the health care provider if there is evidence of worsening HF.
heart failure definition
inadequate pumping and/or filling of the heart
-perfusion insufficient to meet O2 needs of tissues
characterized by 1. ventricular failure, 2. reduced exercise tolerance, 3. diminished quality of life, 4. shortened life expectancy
congestive heart failure
older term, not all heart failure causes pulmonary congestion
new terms: acute vs. chronic heart failure
etiology of heart risk factors
1. CAD 2. age. 3. HTN 4. diabetes, 5. tobacco use, 6. obesity, 7. high serum cholesterol
HF etiology
Any interference with normal regulating mechanisms for CO. Changes lead to decreased ventricular function.
1) preload
2) afterload
3) myocardial contractility
4) heart rate
Mechanisms that regulate CO
1) preload
2) afterload
3) myocardial contractility
4) heart rate
Ejection fraction, normal
the amount of blood ejected from the left ventricle with each contraction, normally 55-60%
EF in systolic HF
decreases, <45%
normally 55-60%
Clinical sign of HF (9)
FACES: fatigue, limited activities, chest congestion, edema, SOB
1) fatigue
2) dyspnea
3) tachycardia
4) edema
5) nocturia
6) skin changes
7) behavioral changes
8) chest pain
9) weight changes
10) muscle wasting, thin arms and legs
Fatigue (symptom of HF)
Early symptom
Unable to perform usual activities
Caused by: decreased CO, impaired perfusion, decreased oxygenation, anemia
Anemia (HF)
Caused by poor nutrition, renal disease or drug therapy
Dyspnea (symptom of HF)
Common manifestation
Caused by increased pulmonary pressure secondary to interstitial and alveolar edema.
Mild exertion, at rest
Adaptive behaviors, sleeping with more pillows
Paroxysmal nocturnal dyspnea (PND)
Reaborption of fluid from dependent body when pt is flat.
Awake with panic, feeling of suffocation, impulse to sit or stand up.
Cough is first clinical symptom: dry, nonproductive cough not relieved by position change or OTC medication
Tachycardia (symptom of HF)
Early clinical symptom
Compensate for failing ventricle-> increase HR
Decrease CO activates SNS
May be reduced or absent in pt on beta-blockers
Edema (symptom of HF)
Common sign, pitting edema, weight gain more than 3 lb in 2 days
-Dependent body parts (peripheral edema)
-Liver (hepatomegaly)
-Abdominal cavity (acites)
-Lungs (Pulmonary edema and effusion)
Nocturia (symptom of HF)
Increased renal blood flow and diuresis
When they lie down to sleep fluid moves from interstitial space back into circulatory system, cardiac workload decreases at rest
Skin changes (symptom of HF)
-dusky skin, increased capillary O2 extraction
-swollen shiny lower extremity, diminished or absent hair, pigment changes
Behavior changes (symptom of HF)
-decreased cerebral ciruculation
-restlessness, confusion, decreased attention span or memory
-secondary to poor gas exchange
-often in late stages
chest pain (symptom of HF)
-angina, chest pain
-decreased coronary artery perfusion from decreased CO
Weight changes (symptom of HF)
-fluid retention partially due to renal failure
-abdominal fullness, ascites
-hepatomegaly-> anorexia and nausea
-
cachexia
-wasting, muscle loss, atrophy
-weakness, fatigue
Primary risk factors for HF
-hypertension
-CAD
Contributing factors, HF
-advanced age
-diabetes
-tobacco use
-obesity
-high serum cholesterol
• Important nursing responsibilities in the care of a patient with HF include
1) teaching the patient about the physiologic changes that have occurred,
(2) assisting the patient to adapt to both the physiologic and psychologic changes, and
(3) integrating the patient and the patient's family or support system in the overall care plan.
(4) Many patients with HF are at high risk for anxiety and depression.
(5) Patients should be taught to evaluate the action of the prescribed drugs and to recognize the manifestations of drug toxicity.
(6) teach patients to take own pulse rate, esp. if taken digitalis and beta blockers
(7) instruct on home bp monitoring
(8) teach signs of hyper/hypokalemia if taking diuretics
(9) have PT instruct on energy conservation
(10) sodium reduction diet, medications, exercise, slowing progression of disease
Key complications after transplantation include
1. acute rejection,
2. risk for sudden cardiac death,
3. infection, and
4. cardiac transplant vasculopathy.
5. Life-time immunosuppression plus corticosteroids are necessary.
6. Endomyocardial biopsies are typically used to detect rejection.
• Nursing management throughout the posttransplant period focuses on
1. promoting patient adaptation to the transplant process,
2. monitoring cardiac function,
3. managing lifestyle changes, and
4. providing ongoing teaching of the patient and family.
After the first year following a heart transplant, the nurse knows that which is the major cause of death?
malignancy (especially lymphoma) and cardiac vasculopathy (accelerated coronary artery disease [CAD]) are the major causes of death
During the first year following a heart transplant, the nurse knows that which is the major cause of death?
infection and acute rejection are the major causes of death.
The diagnosis of diastolic heart failure is based on the presence of heart failure symptoms with
a normal ejection fraction, which is between 55% and 60%. Diastolic failure is characterized by high filling pressures because of stiff ventricles
Absolute contraindications for heart transplant include
1. physiologic age over 65,
2. presence of advanced cerebral or vascular disease, and
3. severe pulmonary disease that may depend on the patient being ventilator-dependent after transplant.
Indications for heart transplant include recurrent life-threatening dysrhythmias not responsive to maximal interventions and cardiac abnormalities that severely limit normal function.
Cardiac dilation is an
enlargement of the heart chambers, usually the ventricles; it occurs when pressure in the heart chambers is elevated over time
symptoms of digitalis toxicity
1. Poor appetite,
2. low heart rate
3. altered mental status, and
4. seeing halos around lights
5. Anorexia,
6. nausea,
7. vomiting,
8. blurred or yellow vision, and
9. cardiac dysrhythmias are all signs of digitalis toxicity
Dopamine is a β-adrenergic agonist whose inotropic action is used .
for treatment of severe heart failure accompanied by hemodynamic instability. Such a state may be indicated by tachycardia accompanied by hypotension
When preparing to administer the vasodilator nitroprusside (Nitropress), the nurse should
1. assess the patient's blood pressure before the administration.
2. ensure a slow rate of IV administration to prevent a sudden reduction in blood pressure.
3. The blood pressure should be assessed again every 5 to 10 minutes during administration to avoid hypotension
Cor pulmonale is the .
dilation of the right ventricle caused by pulmonary diseases. It manifests as right heart failure
Carvedilol is a β-adrenergic blocker
and prevents catecholimines from affecting the heart by increasing the rate. β-adrenergic blocking medications block or prevent catecholamines affecting the heart by increasing heart rate.