Looks like no one added any tags here yet for you.
Two domains of prokaryotes
Archaebacteria
Eubacteria
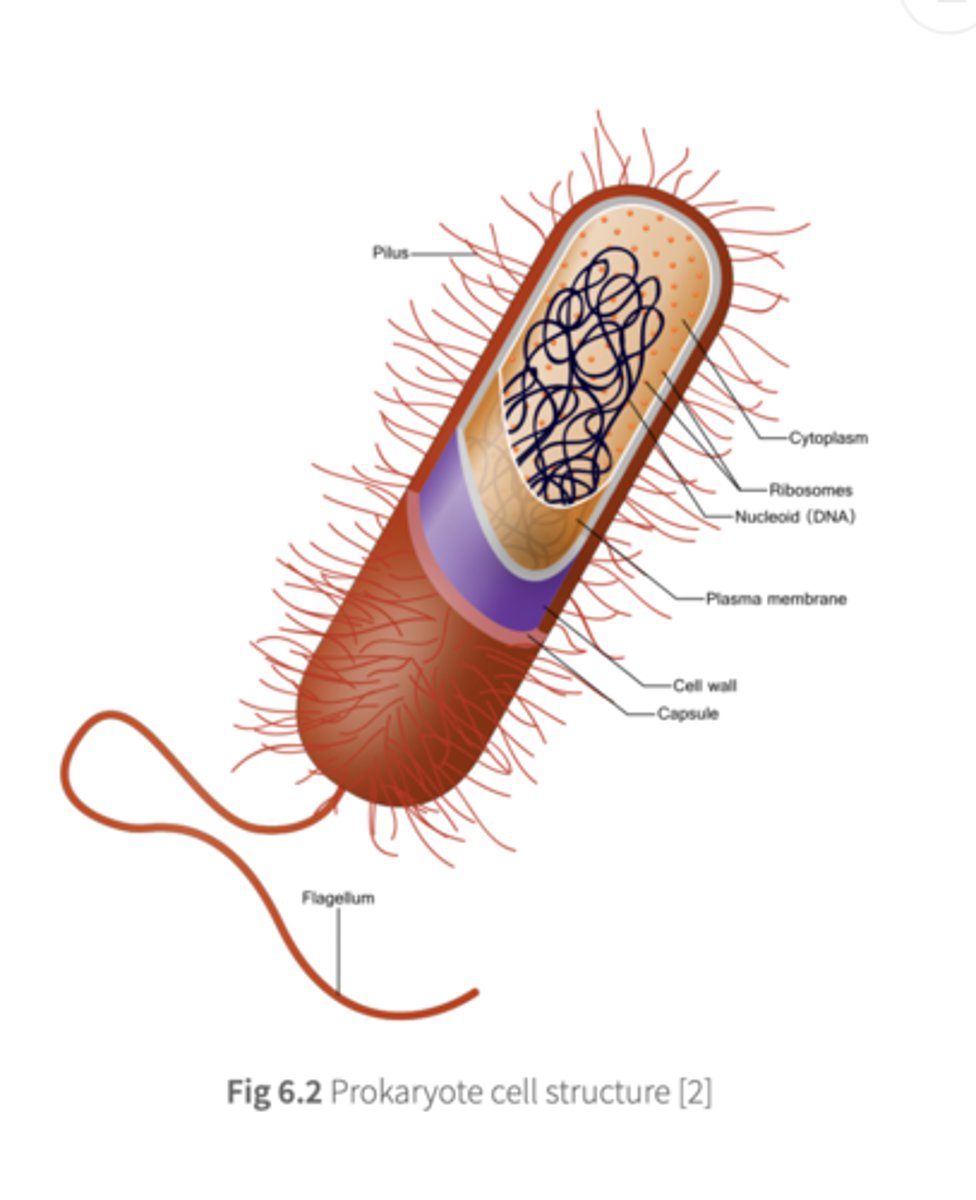
Features of prokaryotes not found in eukaryotes
- Cell wall made of peptidoglycans
- Nucleoid: chromosomal region with with no membrane
Features of eukaryotes not found in prokaryotes
- Nucleus
- Cytoplasmic organelles: mitochondria, ER, golgi(except ribosomes)
Polymeric compound found in bacterial cell walls and not found in eukaryotes
Peptidoglycan
Advantage to having a peptidoglycan cell wall
Increased resistance to osmotic pressure
Basis of medical treatments that target bacteria
They target the unique features of bacteria, such as the peptidoglycan cell wall (suceptible to known drug classess) and prokaryotic ribosomes
Fimbrae and pili functions
hair-like projections that allow bacteria to adhere to surfaces and form a conduit for genetic exchange between cells.
Glycocalyx function
protects bacteria from phagocytosis
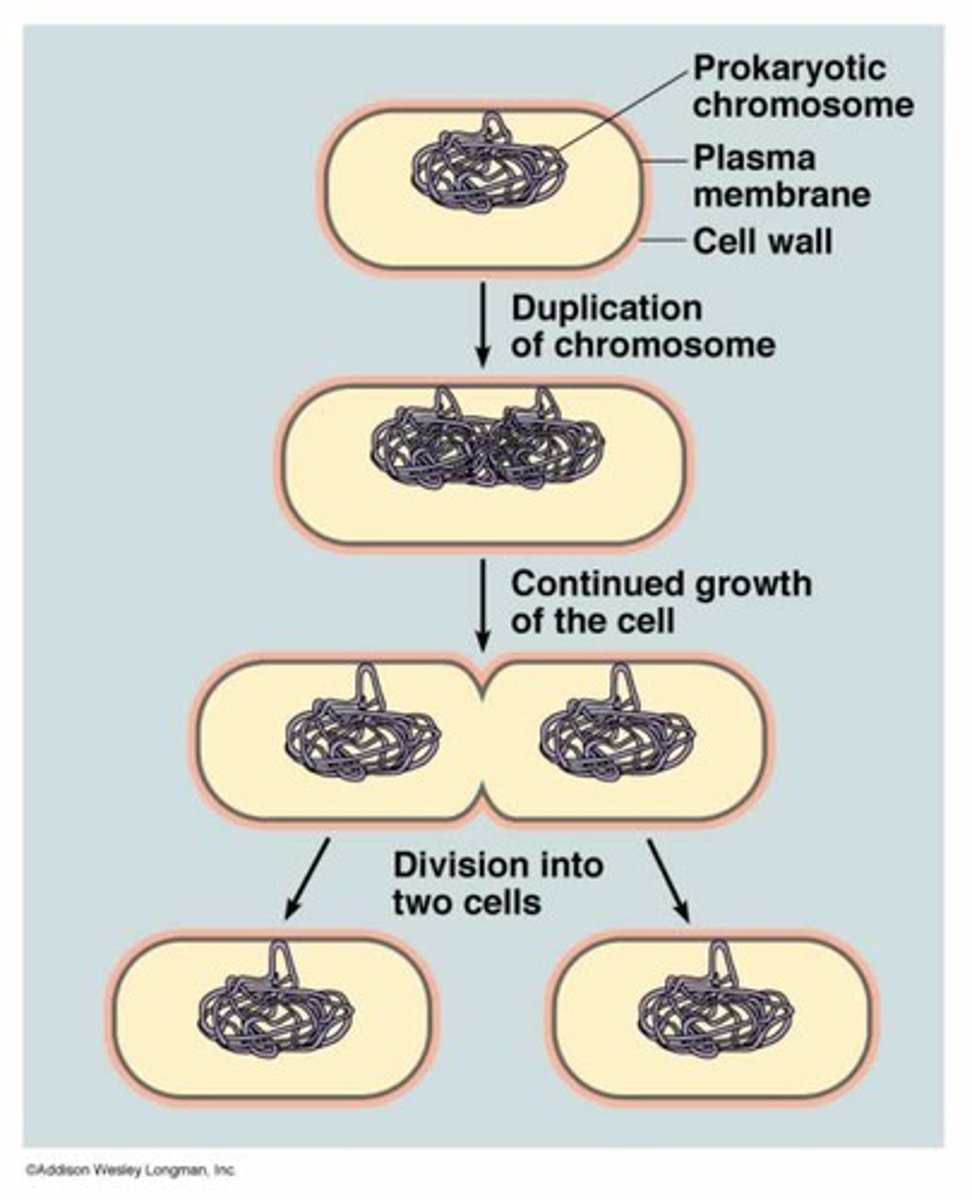
Mechanism for bacterial reproduction
Binary fission
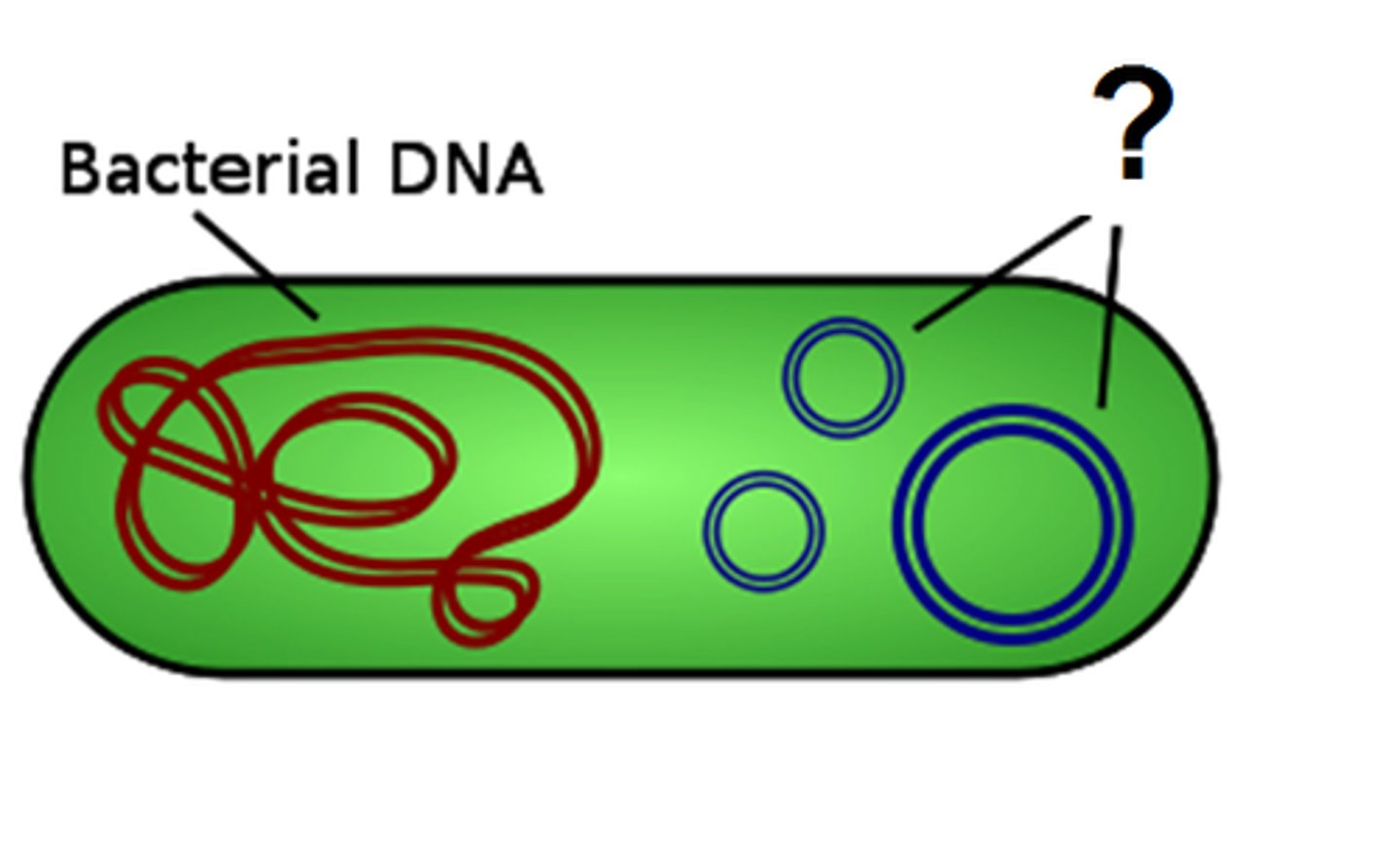
Plasmids
Where additional bacterial genes are carried in smaller, extra chromosomal DNA circlets
- contain genes capable of being transmitted to other bacterial cells
Binary fission
Single circular chromosomal DNA is copied and assorted into two progeny cells
Factors that influence bacterial cell division rate
- Varies among species
- Nutrient availability
- Temperature
- pH
- Osmolarity
How are bacterial pathogens identified in lab?
- nutrient requirements are used for different microbiological identification
- nutrients are restriced and supplied in culture media
- bacterial pathogens identified from samples of infected tissue or bod fluids
- bacteria grows into visible patterns or colonies: identification of bacterial species
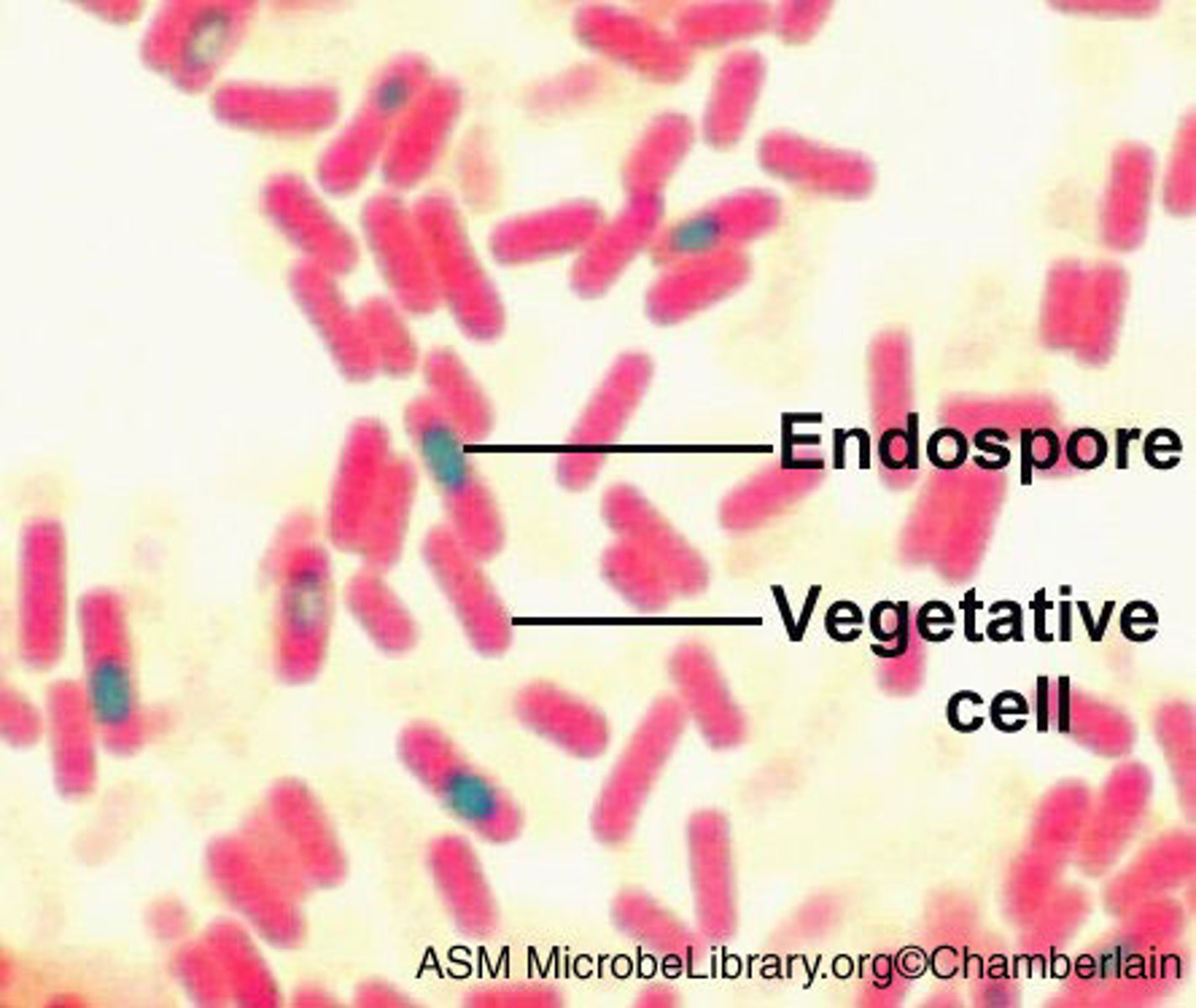
Endospores
- Produced by some bacteria when growth conditions are unfavourable.
- Highly durable and able to persist in a dormant state for hundreds of years
- resistant to extreme cold and heat
Vegetative bacterial cells
What endospores germinate and grow into when conditions permit
- the metabolically active, growing, and reproducing form of bacteria; contrast to dormant, resistant endospore
Ways to classify bacteria
- Staining (Gram negative/positive)
- Cell shape (cocci, diplococci, etc)
- Special features, ex. pathogenicity and antibiotic resistance
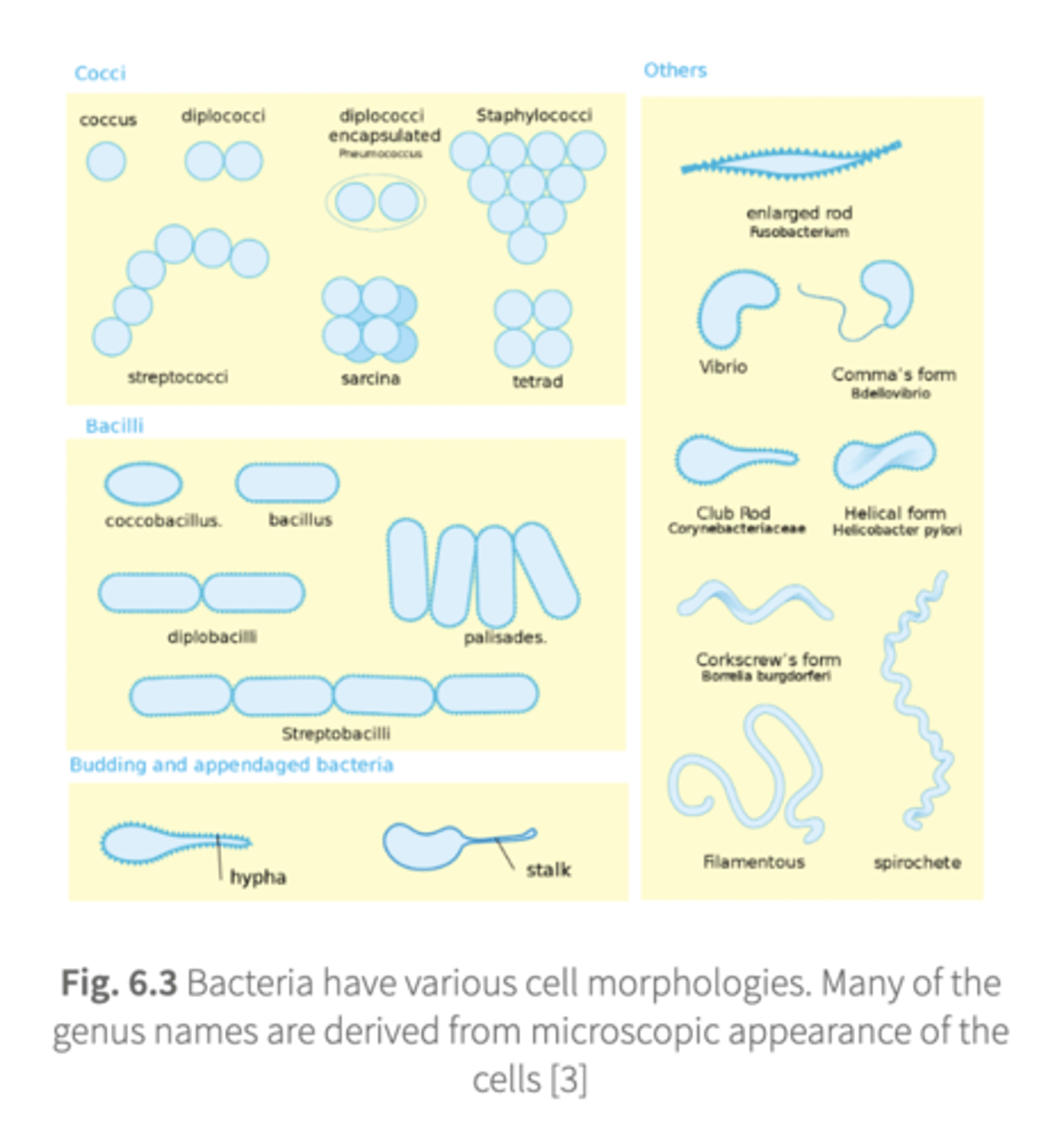
Where are genus names derived from?
Microscopic appearance of cell
Various cell morphologies of bacteria
- diplococci encapsulated (shape): pneumococcus (bacteria)
- enlarged rod: fusobacterium
- comma's form: bdellovibrio
- club rod: corynebacteriaceae
- helical form: helicobacter pylori
- corksrew's form: borrelia burgdorferi
Glycocalyx
Polysaccharide coating on bacteria
If most species are non-pathogenic, what causes bacterial species to expand in number and range?
- if host resistance is compromised and opportunistic infections present a challenge
- true pathogens: more virulent and cause tissue damage/clinical manifestations
What the virulence of bacteria partly depends on?
- Ability to resist phagocytic attack from host defenses
What polysaccharide coating do pathogenic streptococcus have which protects them?
Glycocalyx
Examples of virulence
- glycocalyx of streptococcus
- collagenase and lecithinase of clostridium perfringens breaks down connective tissue (cellulitis)
- tuberculosis bacillus survives phagocytosis and continues dividing
- bacteria producing toxins/seek refuge in host cells
Factors that influence the extent of host tissue injury caused by pathogenic bacteria
- Number of bacteria present
- Virulence of bacteria (especially the type of toxins it contains/produces)
- Site of infestation
- Resistance of the tissue
What is an important part of the pathogenic ability of bacteria?
- Produce toxins
- Both types of toxins (endotoxin and exotoxin) are produced by a range of bacteria species and diffuse into blood/fluids- acts at sites distal from bacterial proliferation
Bacteremia
Presence of bacteria in the blood
Septicemia
Infection of the blood
Main chemical classes of bacterial toxins
- Proteins (secreted exotoxins)
- Lipopolysaccharides (endotoxins derived from Gram negative cell walls)
Differences between gram-positive and gram-negative
Gram-Positive Bacteria
- Thick peptidoglycan layer (appears purple)
- No outer membrane
- Small or absent periplasmic space
- Lacks LPS (endotoxins) but can produce exotoxins
- More susceptible to antibiotics - but can adapt to be resistant (e.g., penicillin [b-lactamase causes resistance], vancomycin)
- Examples: Staphylococcus aureus, Streptococcus pyogenes, Bacillus, Clostridium
Gram-Negative Bacteria
- Thin peptidoglycan layer (appears pink/red)
- Has an outer membrane (provides antibiotic resistance)
- Large periplasmic space (contains enzymes that break down antibiotics)
- Contains LPS (endotoxins), which can trigger severe immune responses
- More resistant to antibiotics
- Examples: Escherichia coli, Pseudomonas aeruginosa, Salmonella, Neisseria
Class of bacteria that are able to produce endotoxins
Gram-negative bacteria, since endotoxins are derived from their cell walls
Examples of how different toxins are produced by many species of bacteria
- Vibrio cholerae: causes cholera and releases a toxin which binds to G protein in intestinal epithelium, leading to disruption in normal cell signalling, resulting in flood of intestinal water= diarrhea
- Clostridium botulinum: causes botulism- releases an exotoxin that acts at neuromuscular junction
T or F: Exotoxins are produced only by Gram positive bacteria
False. Virulent Gram negative species also produce exotoxins
Clostridium tetanii
- Tetanus toxin
- Inhibits inhibitory neurons in CNS → rigid paralysis
Vibrio cholerae
- Cholera toxin
- Activation of adenylyl cyclase → promotes intestinal secretion of fluid and electrolytes → diarrhea
Bordatella pertussis
- Pertussis toxin
- Inhibits adenylyl cyclase → reduced phagocytosis → "whooping cough"
Corynebacterium diphtheriae
- Diphtheria toxin
- Inhibits protein synthesis → cell death → tracheal pannus
Escherichia coli
- E. coli heat labile protein
- Similar to cholera toxin → diarrhea
Shigella dysenteriae and family
- Shiga protein
- Inhibits protein synthesis → cell death → diarrhea
Clostridium botulinum
- Botulinum toxin
- Inhibits acetylcholine at neuromuscular junction → flaccid paralysis
Bacillus anthracis
- Anthrax toxin
- Cytokine secretion
Staphylococcus aureus
- Exfoliatin B
- Separation of skin layers
Virulent bacterial strains produce ___, while other strains do not
Toxins
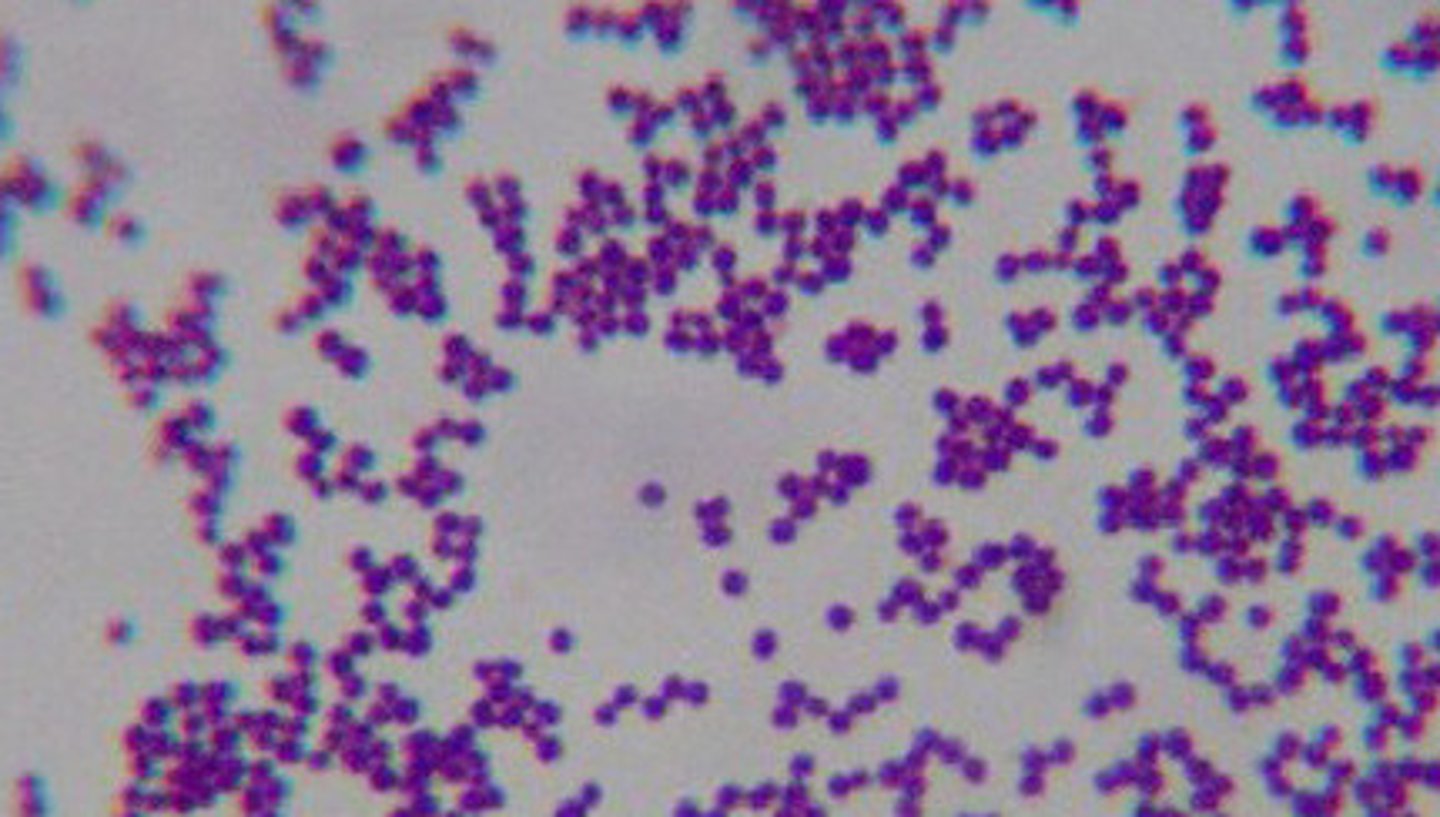
Gram-positive cocci
- Staphylococci: S. aureus, S. epidermis
- Streptococci: S. pyogenes, S. agalactiae, Viridans group, S. pneumoniae
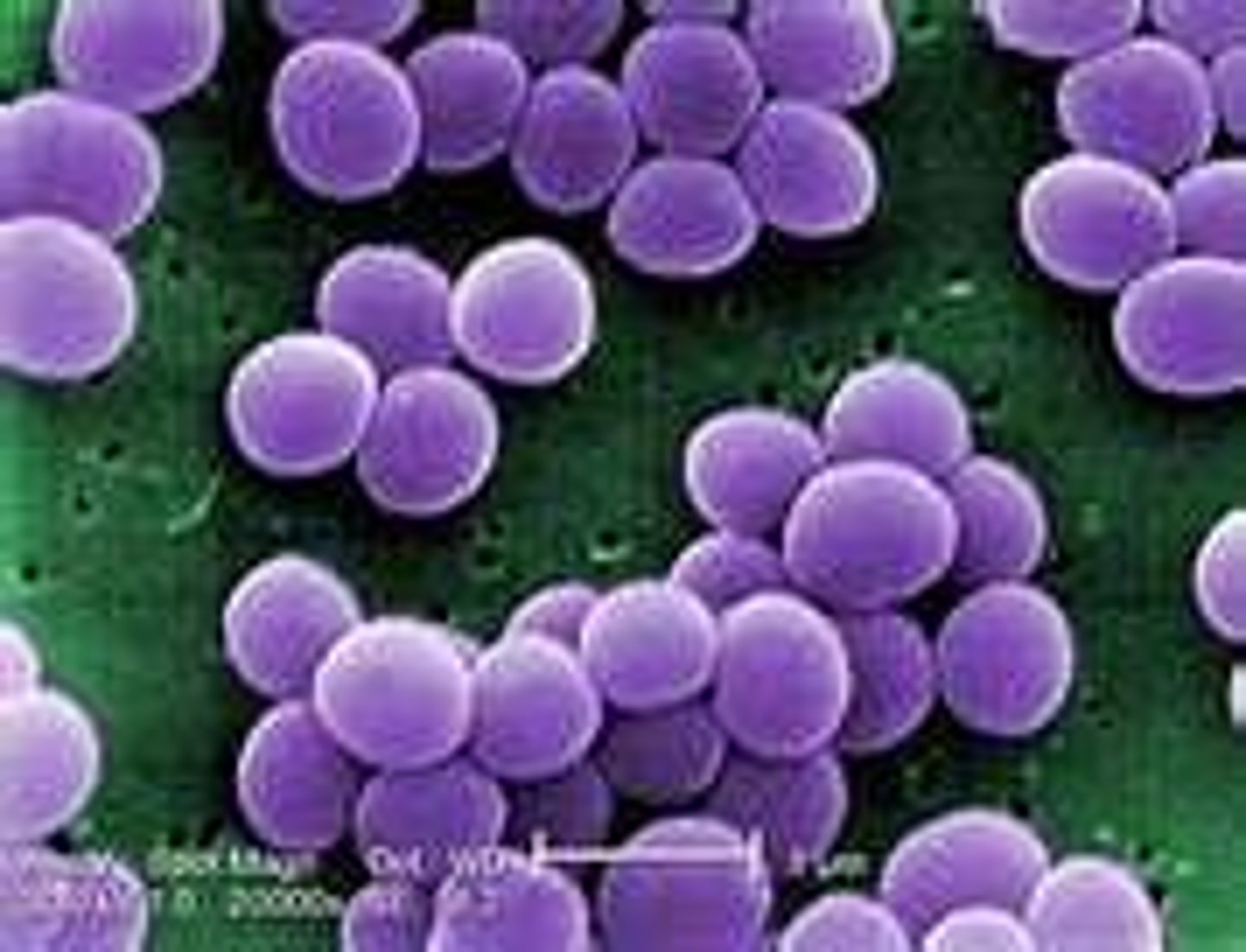
General characteristics of staphylococci
•Common inhabitant of the skin and mucous membranes
•Spherical cells arranged in irregular clusters
•Gram-positive
•Lack spores and flagella
•May have capsules
Staphylococcus aureus (S. aureus)
- One of the most important bacterial pathogens.
- A nosocomial infection
- Grows in large, round, opaque colonies
- Optimum temperature of 37.C
-Facultative anaerobe
- Most resistant of the non-spore producing bacteria: Withstands high salt, extremes in pH, and high temperatures
- Carried in nasopharynx and skin
- Produces many virulence factors
Infections that Staphylococcus aureus is a common cause of
- Boils
- Impetigo
- Wound infections
- Pneumonia
- Osteomyelitis
- Endocarditis
Staphylococcus aureus enzyme virulence factors
- Coagulase (coagulates blood)
- Hyaluronidase (digests connective tissue)
- Staphylokinase (digests blood clots)
- DNase (digests DNA)
- Lipases (digests oils; enhances colonization on skin)
- Penicillinase (inactivates penicillin)
Staphylococcus aureus virulence factors
- Hemolysin (lyses RBCs, skeleal muscles, heart cells, renal tissue)
- Coagulase (coagulates blood and plasma)
- Leukocidin (lyses neutrophils and macrophages)
- Enterotoxin (induces GI distress)
- Exfoliative toxin (separates epidermis from dermis)
- Toxic shock syndrome toxin (induces fever, shock, vomit, systemic organ damage)
Epidemiology and pathogenesis of S. aureus
•frequently in human environments
•present in fomites
•Carriage rate: 20-60%.
•Carriage in anterior nares, skin, nasopharynx, intestine.
•predisposing factors: poor hygiene and nutrition, tissue injury, preexisting primary infection, diabetes, immunodeficiency.
•Increase in community acquired methicillin resistance - MRSA
Localized cutaneous infections of staphylococcal disease
invade skin through wounds, follicules, glands
- folliculitis
- furuncle
- carbuncle
- impetigo
folliculitis
superficial inflammation of hair follicle; usually resolved with no complications but can progress
furuncle
• boil; inflammation of hair follicle or sebaceous gland progresses into abscess or pustule
carbuncle
larger and deeper lesion created by aggregation of cluster of furuncles
impetigo
bubble-like swellings that can break and peel away; most common in newborns
Systemic infections that staphylococcus aureus causes
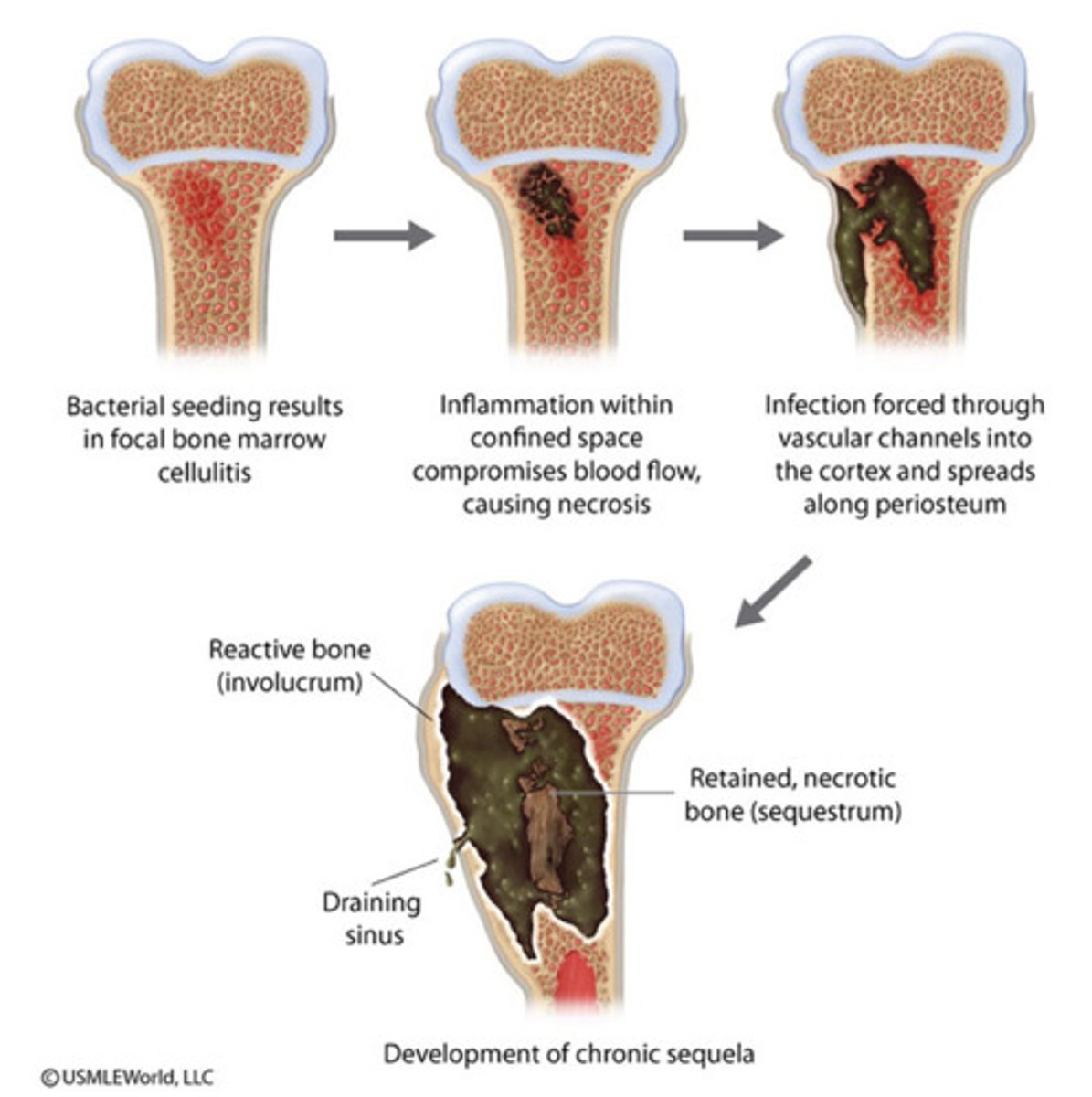
- Osteomyelitis
- Bacteremia
Osteomyelitis
- infection in metaphysis; abscess forms
bacteremia
originates from bacteria of infected site or medical device; endocarditis possible
Toxigenic disease of staph disease
- Staphylococcal food poisoning: ingestion of heat stable enterotoxins; GI distress
- Staphylococcal scalded skin syndrome: bright red flush blisters; desquamation of epidermis, peels skin layers; in eyes or umbilicus of newborn
- Toxic shock syndrome: shock and organ failure; menstrual tampons
Coagulase-negative staphylococcus
Causes wound infections by penetrating skin: 3 of these
- s. epidermis: skin, mm, endocarditis, bacteremia, UTI
- s. hominis: apocrine sweat glands
- s. capitis: scalp, face, external ear
- s. saprophyticus: skin, intestine, UTI
Reason why >80% of S. aureus strains are resistant to penicillin
They express the enzyme β-lactamase which hydrolyzes penicillin
- also resistant to: methicillin, oxacillin, cepalothin
Staphylococcus epidermidis
- commensal organism
- opportunistic pathogen and nosocomial infection
- Infections not life-threatening just difficult to treat
Commensal organism
Part of normal human flora
The most common nosocomial infection; opportunistic pathogen
Staphylococcus epidermidis; associated with catheters
How are staph identified in samples?
- present in pus, tissue exudates, sputum, urine, and blood
- cultivation, catalase, biochemical testing, coagulase
What is the treatment for staphylococcal disease?
- 95% have penicilinnase: resistant to penicillin and ampicillin
- MRSA carry multiple resistance
- abcesses are surgically perforated
- systemic infections require lengthy therapy
Prevention of staph infections
hygiene and cleansing; universal precautions by HCP
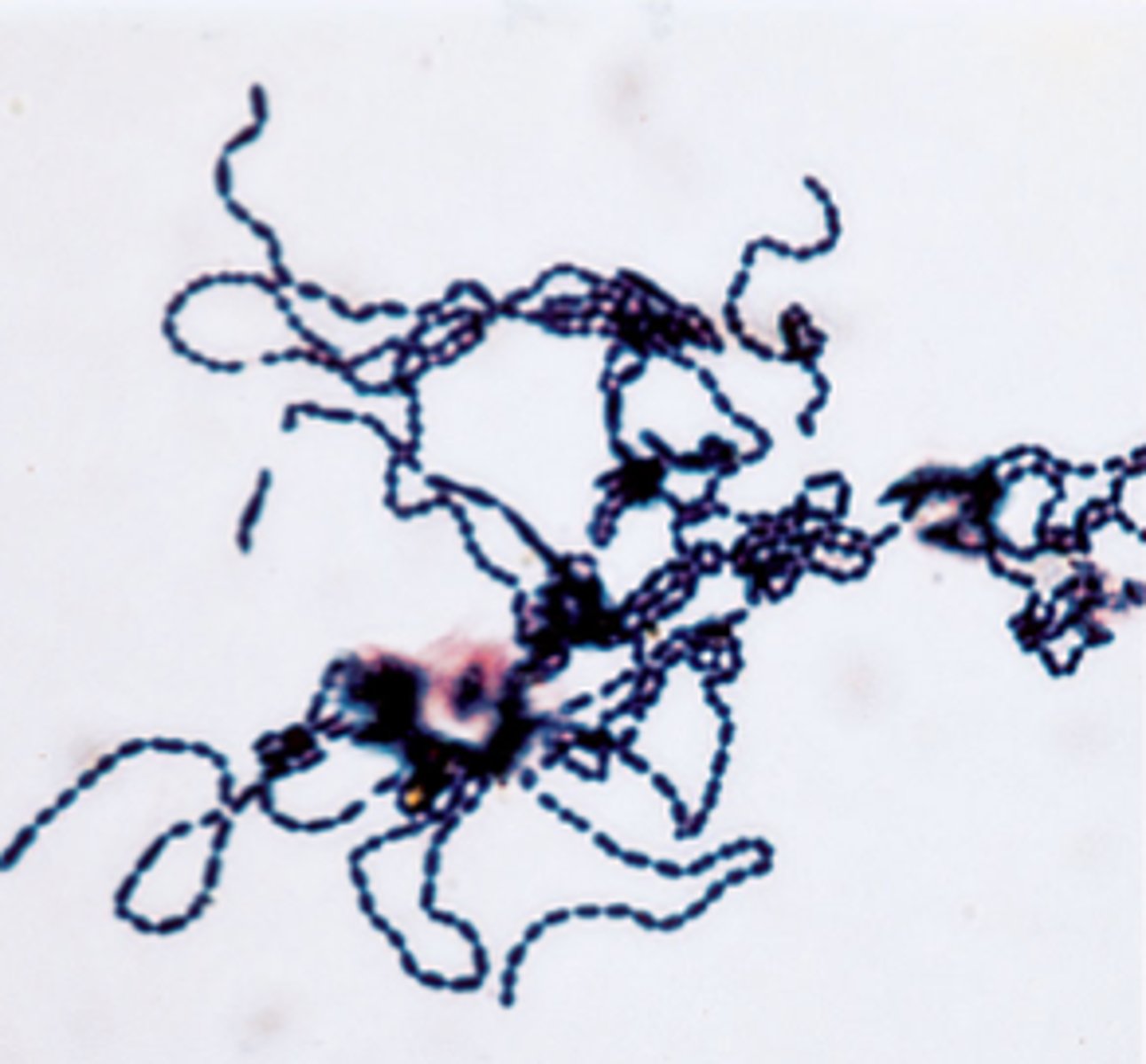
Streptococci
- gram-positive spherical cocci in long chains; in pairs
- non-spore forming; nonmotile
- can form capsules and slime layers
- facultative anaerobes
- do not form catalase
- has peroxidase system
- sensitive to drying, heat, and disinfectants
Classes of streptococci based on hemolysis reactions (virulence)
α-hemolytic: S. pneumoniae, S. viridans
β-hemolytic: S. agalactiae, S. pyogenes (A, B, C, G, D)
- Lancefield classification system based on cell-wall antigens (A, B, C....)
beta-hemolytic strep that are bacitracin sensitive and bacitracin resistant
- bacitracin-sensitive: group A (S. pyogenes)
- bacitracin-resistant: group B, C (S. agalactiae)
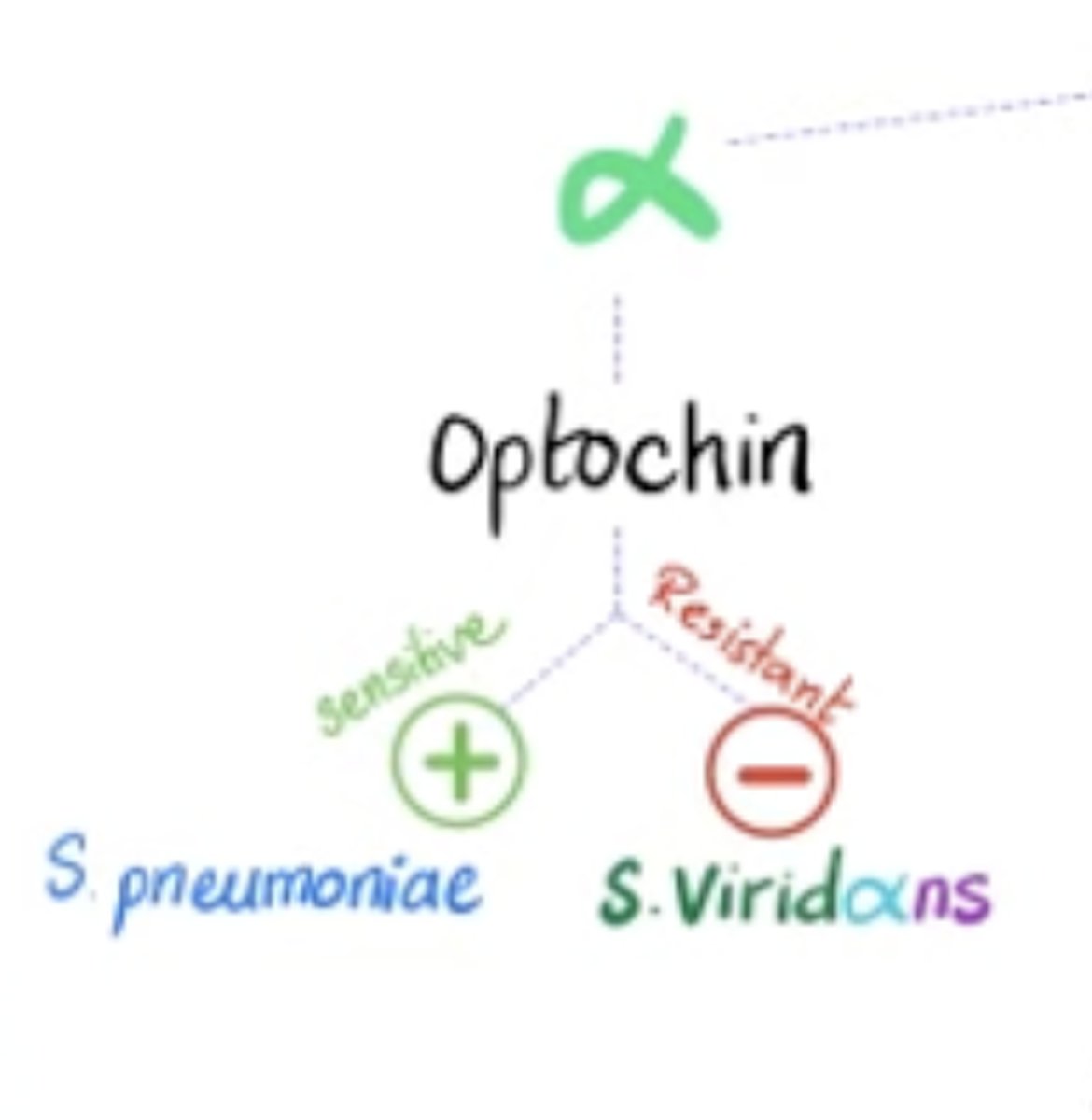
alpha-hemolytic strep that are optochin sensitive and optochin resistant
- optochin-sensitive: s. pneumoniae
- optochin-resistant: group D and viridans strep
α-hemolytic strep bacteria
Streptococcus pneumoniae
Streptococcus viridans
Group A strep bacteria (β-hemolytic)
S. pyogenes
Streptococcus pyogenes
Most virulent of the group A (β-hemolytic) streptococci
Group B strep bacteria (β-hemolytic)
S. agalactiae
Group D strep bacteria (β-hemolytic)
- E. faecalis, E. faecium, E. durans
- in large intestine
- cause opportunistic urinary, wound, and skin infections, particularly in debilitated persons
Group C and G strep bacteria (β-hemolytic)
Common animal flora
Streptococcal pathogens
S. pyogenes
S. agalactiae
Viridans group
S. pneumoniae
Enterococcus faecalis
Surface antigens virulence factors of S. pyogenes
C-carbohydrates- protects against lysozyme
Fimbriae- adherence
M-protein- resistance to phagocytosis
Hyaluronic acid capsule- provokes no immune response
Extracellular toxins (virulence factors) of S. pyogenes
Streptolysins- hemolysins; SLO and SLS- cause cell and tissue injury
Pyrogenic toxin (induces fever)
Superantigens (monocyte and lymphocyte stimulants; causes release of tissue necrotic factor)
Extracellular enzymes of S. pyogenes
Streptokinase (digests blood clots)
Hyaluronidase (digests connective tissue)
DNase (hydrolyzes DNA)
Epidemiology and pathogenesis of S.pyogenes
•Humans only reservoir
•Inapparent carriers
•Transmission - contact, droplets, food, fomites
•Portal of entry: skin or pharynx
•Children predominant group affected- cutaneous and throat infections
Skin infections that S. pyogenes can cause
Impetigo- superficial lesions that break and form highly contagious crust
Erysipelas- pathogen enters through a break in the skin and eventually spreads to the dermis and subcutaneous tissues; superficial or systemic
Throat infection that S. pyogenes can cause
Streptococcal pharyngitis 'strep throat'
Systemic infections that S. pyogenes can cause
- Scarlet fever- strain of S. pyogenes that codes for pyrogenic toxin; can sequelae
- Septicemia
- Pneumonia
- Streptococcal toxic shock syndrome
Long-term complications of group A infection (S. pyogenes)
- Rheumatic fever: follows pharyngitis; carditis, arthritis, chorea, fever
- Acute glomerulonephritis- nephritis, increased blood pressure, occasionally heart failure; can become chronic leading to kidney failure
Group B: Streptococcus agalactiae
- resides in vagina, pharynx, and large intestine
- can be transferred to infant during delivery: if passed to nenonates- can cause meningitis and septicemia in children
- in debilitated people: wound and skin infections, endocarditis
Common cause of pharyngitis
Streptococcus pyogenes; can lead to rheumatic fever and glomerulonephritis if untreated
Treatment and prevention of Streptococci
- Group A and B treated with penicillin
- sensitivity testing for enterococci
- no vaccines available
- resistant to tetracycline
a-Hemolytic Streptococci: Viridans Group
•Streptococcus mutans, S. oralis, S. salivarus,
S. sanguis, S. milleri, S. mitis
Where do the viridans group (α-hemolytic) of strep normally reside
• gums and teeth, oral cavity and also found in nasopharynx, genital tract, skin
How the viridans group (α-hemolytic) normally cause infection
Small cuts from dental procedures can facilitate entrance into the bloodstream
S. mutans
- S. mutans (viridans) produce slime layers that adhere to teeth (plaque)- involved in dental caries
- Persons with preexisting heart conditions should receive prophylactic antibiotics before surgery or dental procedures.
Infections caused by Viridans group
- bacteremia, meningitis, abdominal infection, tooth abscesses
- most serious: subacute endocarditis
- high risk: preexisting heart disease
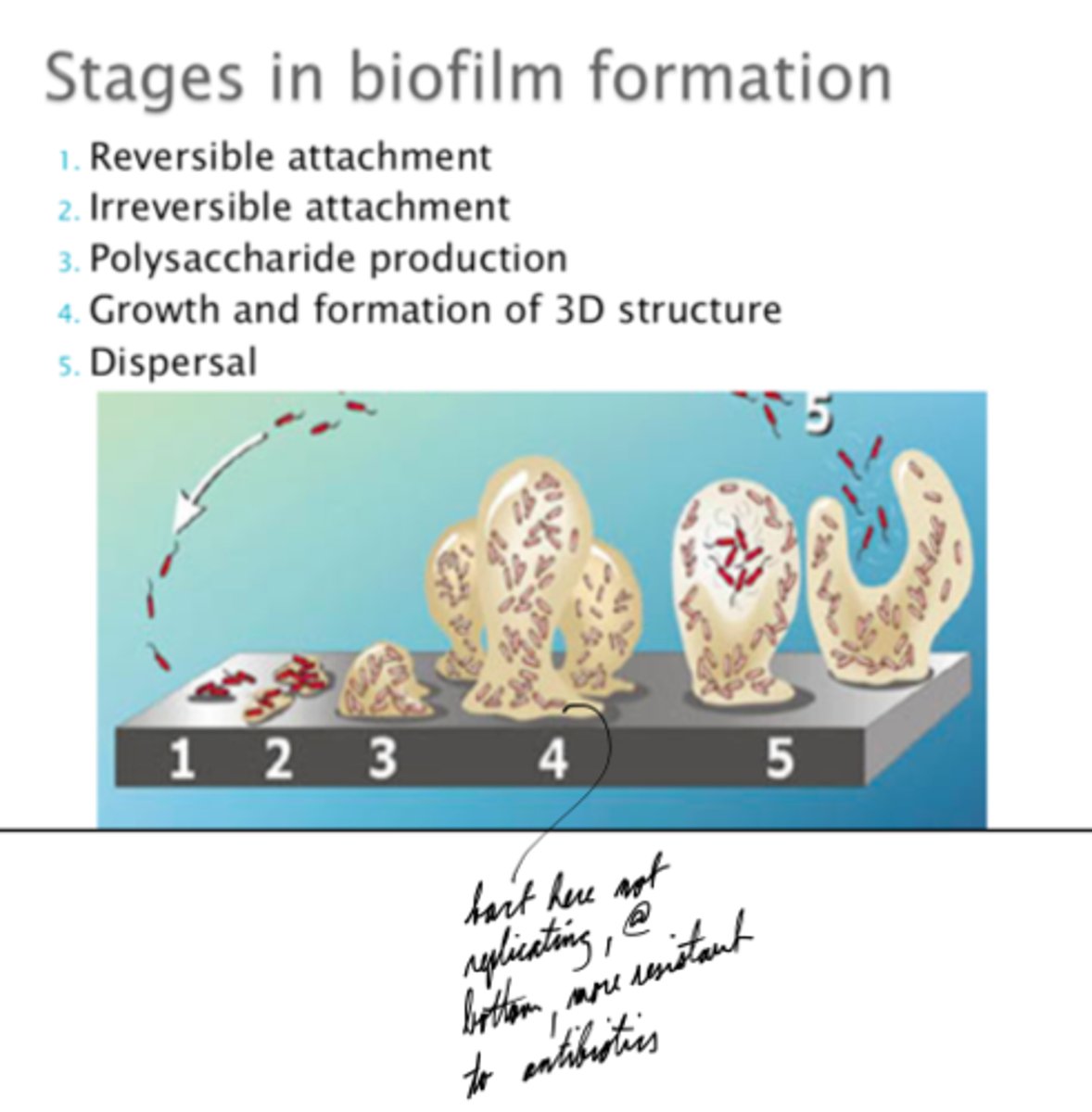
- colonizes heart by forming biofilms
Biofilms
Colonies of bacteria that adhere together and adhere to environmental surfaces.
What is subacute endocarditis?
blood-borne bacteria settle and grow on heart leading to destruction of endocardium and valves
Streptococcus pneumoniae (α-hemolytic)- Pneumococcus
- One of the causes of bacterial pneumonia- just a major one
-Having a nasopharynx helps the bacteria
- very common because our system is poorly designed (e.g. membrane between alveoli and blood is very thin)
- infections usually endogenous
- Cells are aspirated (breathed) into the lungs of susceptible individuals = pneumonia = overwhelming inflammatory response.
- causes pneumonia and otitis media
- Specific soluble substance (SSS) varies among types
How does pneumonia infect the middle ear?
When you cough or sneeze, it pushes bacteria out to eustachian tube and becomes easily infected in middle ear (e.g. kids with smaller eustachian tubes have this)
Major virulence factor of S. pneumoniae
capsule (antiphagocytic)
Treatment and prevention of S. pneumoniae
•Traditionally treated with penicillin G or V
•Increased drug resistance
•Two vaccines available for high risk individuals:
•capsular antigen vaccine for older adults and other high risk individuals-effective 5 years
•conjugate vaccine for children 2 to 23 months
Neisseriaceae Family
•Gram-negative cocci
•Residents of mucous membranes of warm-blooded animals
•Neisseria, Moraxella, Acinetobacter.
•2 main human pathogens:
•Neisseria gonorrhoeae
•Neisseria meningitidis


![<p>Gram-Positive Bacteria</p><p>- Thick peptidoglycan layer (appears purple)</p><p>- No outer membrane</p><p>- Small or absent periplasmic space</p><p>- Lacks LPS (endotoxins) but can produce exotoxins</p><p>- More susceptible to antibiotics - but can adapt to be resistant (e.g., penicillin [b-lactamase causes resistance], vancomycin)</p><p>- Examples: Staphylococcus aureus, Streptococcus pyogenes, Bacillus, Clostridium</p><p>Gram-Negative Bacteria</p><p>- Thin peptidoglycan layer (appears pink/red)</p><p>- Has an outer membrane (provides antibiotic resistance)</p><p>- Large periplasmic space (contains enzymes that break down antibiotics)</p><p>- Contains LPS (endotoxins), which can trigger severe immune responses</p><p>- More resistant to antibiotics</p><p>- Examples: Escherichia coli, Pseudomonas aeruginosa, Salmonella, Neisseria</p>](https://knowt-user-attachments.s3.amazonaws.com/37bb1fd6-afa7-4049-98f3-4083ed58612e.jpg)