Handout Questions - Physio
1/113
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
114 Terms
Subjects A and B are 70 kg men. Subject A drinks 2L of distilled water and subject B drinks 2L of isotonic NaCl. As result of these ingestions, subject B will have a
A. greater change in intracellular fluid(ICF)volume
B. higher positive free-water clearance(C H2O)
C. greater change in plasma osmolarity
D. higher urine osmolarity
E. higher urine flow rate
D
One gram of mannitol was injected into a woman. After equilibration a plasma sample had a mannitol concentration of 0.8 g/L. During the equilibration period,20% of the injected mannitol was excreted in the urine. The subject
A. extracellular fluid(ECF)volume is 1 L
B. intracellular fluid(ICF)volume is 1 L
C. ECF volume is 10 L
D. ICF volume is 10 L
E. interstitial volume is 12.5 L
C
Compared with a person who ingests 2L of distilled water, a person with water deprivation will have a:
A. higher free-water clearance(C H2O)
B. lower plasma osmolarity
C. lower circulating level of antidiuretic hormone(ADH)
D. higher tubular fluid/plasma(TF/P)osmolarity in the proximal tubule
E. higher rate of H2 O reabsorption in the collecting ducts
E
Which of the following would best distinguish an otherwise healthy person with severe water deprivation from a person with the syndrome of inappropriate antidiuretic hormone (SIADH)
A. Free-water clearance(C H2O)
B. Urine osmolarity
C. Plasma osmolarity
D. Circulating levels of antidiuretic hormone(ADH)
E. Corticopapillary osmotic gradient
C
A woman runs a marathon in 90℉ weather and replaces all volume lost in sweat by drinking distilled water. After the marathon, she will have
A. decreased total body water(TBW)
B. decreased hematocrit
C. decreased intracellular fluid(ICF)volume
D. decreased plasma osmolarity
E. increased intracellular osmolarity
D
A 58-year-old woman with coronary artery disease and chronic congestive heart failure is treated with the angiotensin converting enzyme inhibitor lisinopril, the diuretic furosemide, and the beta blocker metoprolol, as well as aspirin. She has been taking an increased amount of ibuprofen for chronic back pain, and she comes to the emergency room with increasing angina and dyspnea. She has a blood pressure of 130/80, bilateral rales, and trace peripheral edema. Her Na+ is 136 mEq/L, BUN is 60 mg/dL, creatinine is 2.4 mg/dl, and urine sediment shows no cells or casts. The basic anatomic unit of the kidney most responsible for this patient's renal related disease is:
A-the blood vessel
B-the glomerulus
C-the tubule
D-interstitium
E-the collecting system
A
A 7-year-old child presents with hypoalbuminemia, edema, hyperlipidemia, and proteinuria. The edema is in the periorbital region initially and eventually spreads to the rest of the body. The patient is given steroid therapy and the disease goes away. What is a key morphological feature of the patient’s disease?
A. Fusion of the foot processes
B. Destruction of the basement membrane
C. Destruction of the glomerulus
D. Hemosiderin laden macrophages in the kidney
A.
No hay answer so puede estar mal
Which of the following does not form part of the glomerular filtration barrier?
A-Endothelial cell fenestration
B-Sub-endothelial space
C-Glomerular basement membrane
D-Podocyte foot process slit diaphragm
E-Sub-podocyte space 3.
E
No hay answer so puede estar mal
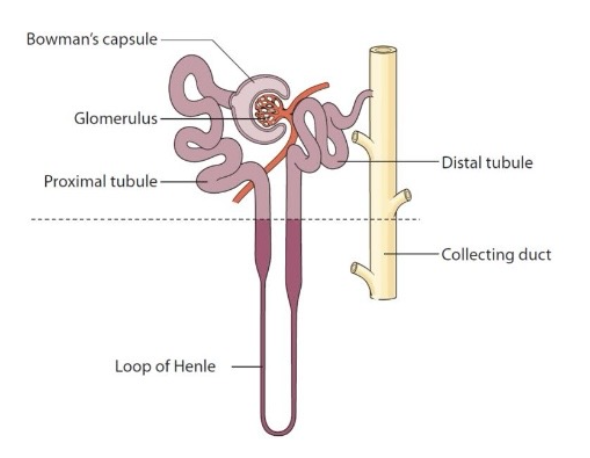
Five Segments of the Nephron
Glomerulus
Filtration
Proximal tubule
Bulk reabsorption
Loop of Henle
Countercurrent multiplication
Distal convoluted tubule
Fine regulation of electrolytes
Collecting duct
Water balance (ADH‑dependent)
Acid‑base regulation
The renal "countercurrent" mechanism is dependent upon the anatomic relationship between:
A. the distal tubule and the macula denza
B. the loop of Henle and the macula denza
C. the loop of Henle and the vasa recta
D. the glomerulus and the afferent and efferent arterioles
E. the glomerulus and the proximal tubule
C
No Hay answer so puede estar mal
The tonicity of the urine as it enters the renal collecting duct is:
A. isotonic
B. hypotonic or isotonic, but never hypertonic
C. hypotonic
D. hypertonic
E. hypertonic or isotonic, but never hypotonic
B
No Hay answer so puede estar mal
The vasa recta:
A. are the straight portions of the proximal tubules, found just proximal to the loops of Henle
B. extend from the efferent arterioles of the superficial cortical nephrons
C. are the microvilli found on the cells of the macula densa
D. comprise the capillary network found in the medulla of the kidney
E. are the small straight segments of afferent arterioles found directly next to the macula densa
D
No Hay answer so puede estar mal
The loops of Henle of the outer cortical nephrons:
A. are functionally unimportant in the renal conservation of sodium and water
B. do not contribute to the medullary osmotic gradient
C. do not participate in the urinary diluting mechanism
D. do not play any important role in overall renal function and are simply unimportant vestiges
of evolutionary development
B
No Hay answer so puede estar mal
Which of the following would cause an increase in both glomerular filtration rate (GFR) and renal plasma flow (RPF)?
A. Hyperproteinemia
B. A ureteral stone
C. Dilation of the afferent arteriole
D. Dilation of the efferent arteriole
E. Constriction of the efferent arteriole
A
If the clearance of a substance which is freely filtered is less than that of insulin
A. there is net reabsorption of the substance in the tubules
B. there is net secretion of the substance in the tubules
C. the substance is neither secreted nor reabsorbed in the tubules
D. the substance becomes bound to protein in the tubules
E. the substance is secreted in the proximal tubule to a greater degree than in the distal tubule
A
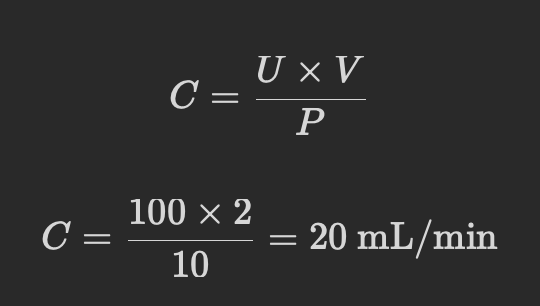
What is the clearance of a substance when is concentration in the plasma is 10 mg/dl,its concentration in the urine is 100 mg/dl, and urine flow is 2 ml/min?
A. 2 ml/min
B. 10 ml/min
C. 20 ml/min
D. 200 ml/min
E. Clearance cannot be determined from the information given
C
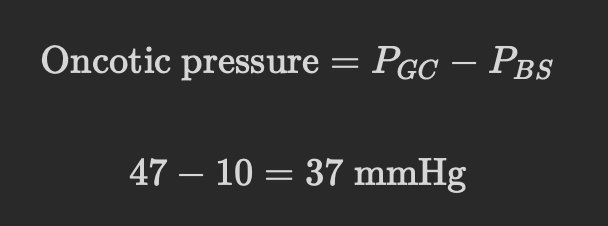
Use the values below to answer the following question.
Glomerular capillary hydrostatic pressure=47 mmHg
Bowman’s space hydrostatic pressure=10 mmHg
At what value of glomerular capillary oncotic pressure would glomerular filtration stop?
A. 57 mmHg
B. 47 mmHg
C. 37 mmHg
D. 10 mmHg
E. 0 mmHg
C
Subjects A and B are 70 kg men. Subject A drinks 2 L of distilled water,and subject B drinks 2 L of isotonic NaCl. As result of these ingestions, subject B will have a
A. greater change in intracellular fluid(ICF)volume
B. higher positive free-water clearance(C H2O)
C. greater change in plasma osmolarity
D. higher urine osmolarity
E. higher urine flow rate
D
Which agent is released or secreted after a hemorrhage and causes an increase in renal Na+ reabsorption?
A. Aldosterone
B. Angiotensin Ⅰ
C. Angiotensin Ⅱ
D. Antidiureis hormone(ADH)
E. Atrial natriuretic peptide
A
In the presence of ADH,the greatest fraction of filtered water is absorbed in the
A. proximal tubule
B. loop of Henle
C. distal tubule
D. cortical collecting duct
E. medullary collecting duct
a
On which of the following does aldosterone exert its greatest effect?
A. Glomerulus
B. Proximal tubule
C. Thin portion of the loop of Henle
D. Thick portion of the loop of Henle
E. Cortical collecting duct
e
Co-transport of glucose:
A. is equivalent to a uniport for glucose
B. will not be affected if the Na+ /K+ pump is blocked
C. cannot move glucose against its concentration gradient
D. is equivalent to an antiproton
E. depends on the interaction of Na+ with the glucose carrier
e
In the distal tubules, sodium reabsorption is increased directly by increased :
A- sympathetic nerve stimulation of the kidney .
B- atrial natriuretic hormone secretion .
C- antidiuretic hormone secretion .
D- aldosterone secretion
E-angiotensin secretion
d
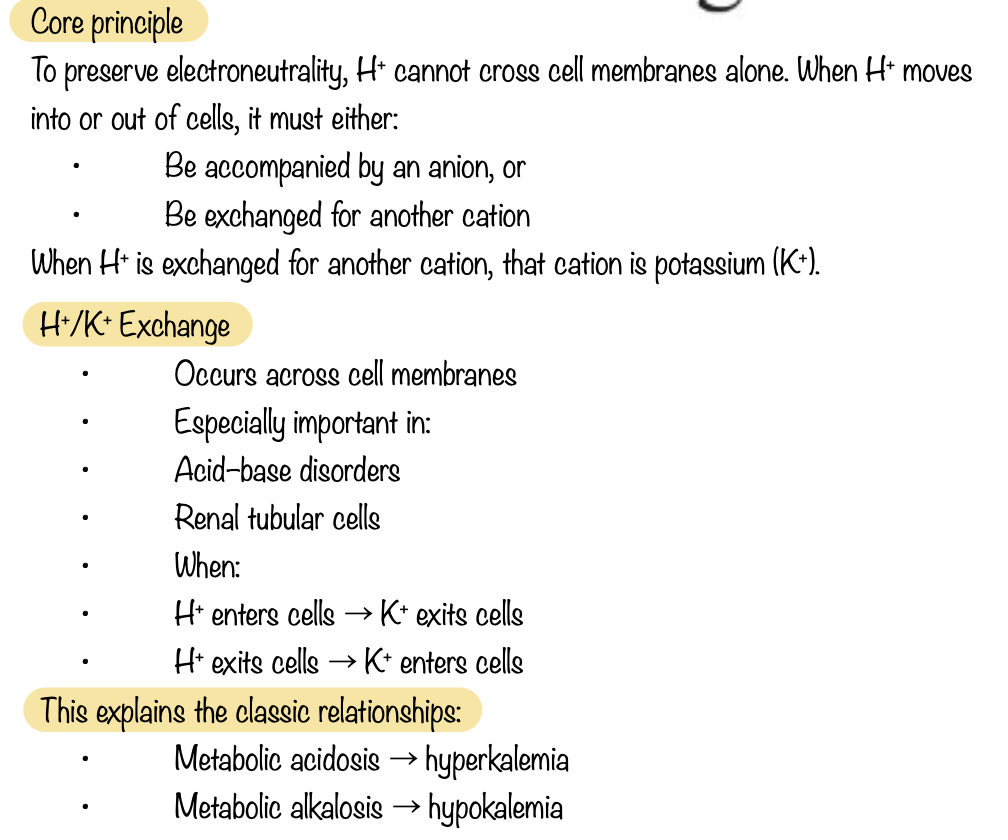
Which of the following causes hyperkalemia?
A. Exercise
B. Alkalosis
C. Insulin injection
D. Decreased serum osmolarity
E. Treatment with β-agonists
a
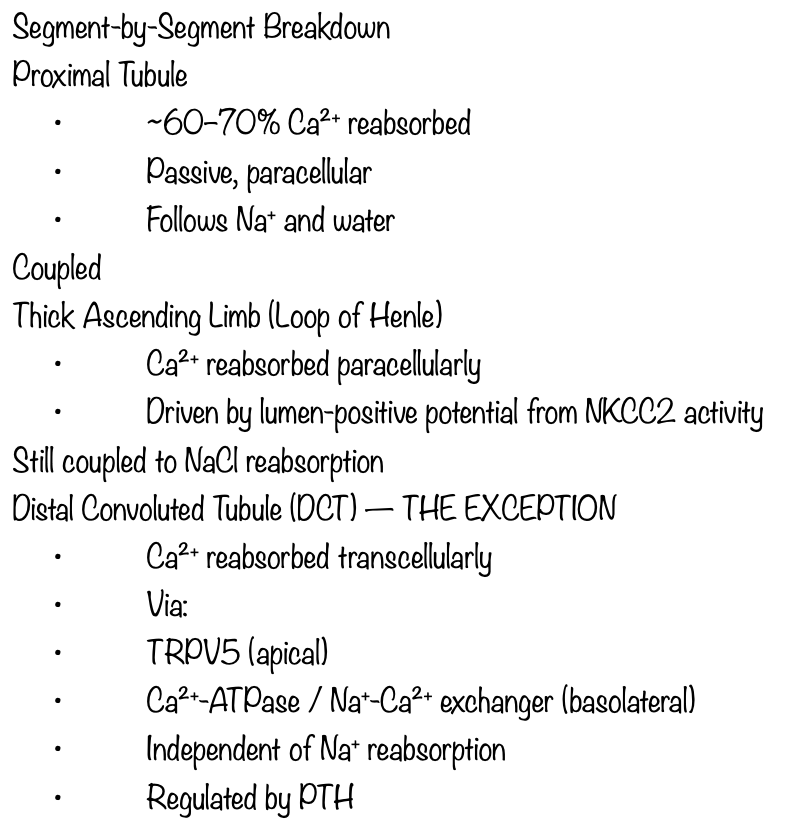
Which of the following is an action of parathyroid hormone(PTH)on the renal tubule?
A. Stimulation of adenylate cyclase
B. Inhibition of distal tubule K+ secretion
C. Inhibition of distal tubule Ca2+ reabsorption
D. Stimulation of proximal tubular phosphate reabsorption
E. Inhibition of production of 1,25-dihydroxycholecalciferol
b
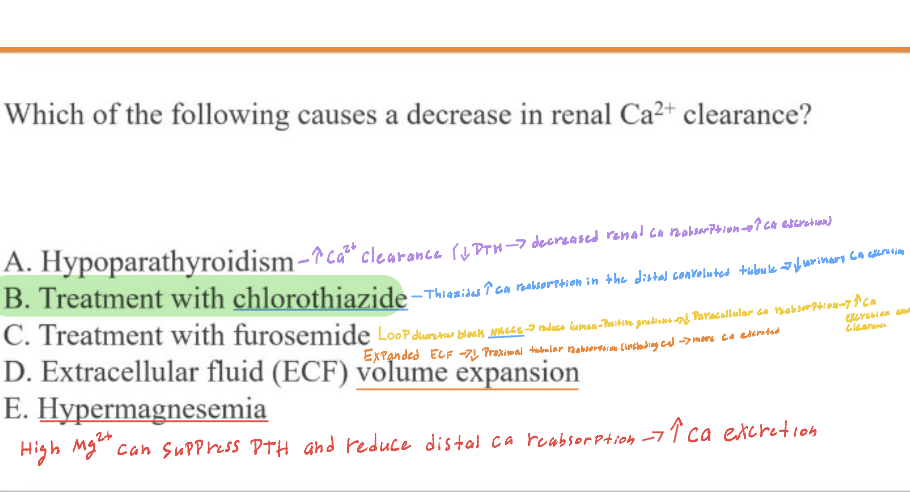
Which of the following causes a decrease in renal Ca2+ clearance?
A. Hypoparathyroidism
B. Treatment with chlorothiazide
C. Treatment with furosemide
D. Extracellular fluid (ECF volume expansion
E. Hypermagnesemia
b
K+ excretion is markedly influenced by :
A-aldosterone
B-amount of Na+ delivered to tubules
C-rate of tubular secretion of H+
D-all the above
d
Renal correction of acute hyperkalemia will result in :
A-alkalosis
B-acidosis
C-increased secretion of HCO3 –
D-increased secretion of H+
E-increased secretion of Na+
d
Each of the following diuretics is paired with a candidate side-effect. Which of the following diuretics is correctly paired with an associated side effect?
A. Furosemide : ototoxicity
B. Hydrochlorothiazide : hypoglycemia
C. Triamterene : hypokalemia
D. Bumetanide : hyperkalemia
E. Acetazolamide: metabolic alkalosis
a
Which of the following diuretics is most likely to result in hyperuricemia?
A. Acetazolamide
B. Glycerol
C. Spironolactone
D. Hydrochlorothiazide
E. Triamterene
d
Which of the following diuretics does not require access to the tubule to reach its site of action?
A. Metolazone
B. Spironolactone
C. Furosemide
D. Hydrochlorothiazide
E. Amiloride
b
A 57-year-old woman weighs 80 kg (176 lb), and her blood pressure is 140/96 mm Hg. She has pitting edema in both legs. Her physician prescribes exercise, restricted sodium intake, and a diuretic agent. Taking inappropriately high doses of which of the following diuretics would be most likely to produce profound diuresis and vascular collapse?
A. Hydrochlorothiazide
B. Spironolactone
C. Triamterene
D. Acetazolamide
E. Furosemide
e
Which of the following would be most likely to be useful as a diuretic in a patient with a history of extreme allergic sensitivity to sulfonamides?
A. Acetazolamide
B. Furosemide
C. Hydrochlorothiazide
D. Ethacrynic acid
E. Torsemide
d
A 5-year-old boy is brought to the emergency room after collapsing at his day care center. He is too ill to answer questions, his parents do not speak English and for the moment, no further history is available. An arterial blood gas shows a pH of 7.20, a pC0₂ of 64, and a HC0³⁻ of 26mtq/. Of the following, which is the most likely cause of his acid-base disturbance?
A-Overdose of salicylates '
B-Severe diarrhea"
C-Diabetic ketoacidosis x
D-Pneumonia and respiratory failure
E-Acute renal failure
d
A 20-year-old woman is referred to you by the college health service because of abnormal blood tests, following her complaint of not feeling well. Her medical history is unremarkable, she takes no medications, and her examination is notable for a blood pressure of 135/80mmHg, a heart rate of 70/minute, and clear lungs, a normal abdomen, and no edema. Arterial pH is 7.33, Na+ is 135 mEq/L, K+ is 3.5 mEq/L, Cl- is 110 mEq/L, and HC0 3- is 16mEq/L. Of the following, which is the most likely diagnosis?
A. Distal renal tubular acidosis
B-An aldosterone secreting tumor
C-Chronic renal failure
D-Excess ingestion of salicylates
a
Match the acid-base disturbance with the clinical scenario and arterial blood gases described in questions 1 through 5.
a. Metabolic acidosis with respiratory compensation
b. Metabolic alkalosis with respiratory compensation
c. Respiratory acidosis with renal compensation (chronic respiratory acidosis)
d. Respiratory acidosis without renal compensation (acute respiratory acidosis)
e. Metabolic acidosis and respiratory acidosis
1. An individual with an asthma attack:
pH=7.32;[HCO−3]=25mEq/L;PCO2=50mm Hg
2. An individual with diabetes mellitus, who forgets to take insulin:
pH=7.29;[HCO−3]=12mEq/L;PCO2=26mm Hg
3. An individual with cardiopulmonary arrest:
pH=6.85;[HCO−3]=10mEq/L;Pco2=60mmHg
4. An individual with a gastric ulcer who ingests large quantities of antacids:
pH=7.45;[HCO−3]=30mEq/L;PCO2=45mm Hg
5. An individual with a 20-year history of smoking 3 packs/day who has emphysema:
pH=7.37;[HCO−3]=28mEq/L;PCO2=50mm Hg
a. 2
b. 4
c. 5
d. 1
e. 3
A 35-year-old woman with type I diabetes mellitus for 25 years developed proteinuria. Her blood pressure is 170/100mmHg, she has neck vein distention, rales, an S3 gallop, and peripheral edema. Which of the following could be the cause of her proteinuria?
A- Damage of podocytes
B- Damage to collecting ducts
C- Change in the cortico medullary gradient
D- Lesion of the Vasa Recta
E- Destruction of the macula densa
a
A 36-year-old African American man with a ten year history of hypertension comes to the hospital with a headache. His blood pressure is 280/140 mm Hg. His urine analysis shows 2+ proteinuria and 2+ hematuria. His serum creatinine is 2.7 mg/dL and the BUN is 34 mg/dl. Which other abnormality would be expected to be present?
A-High serum calcium level
B-High level of ADH
C-High glucose level
D-Abnormal liver function tests
E-High serum K+ level
e
A 69-year-old man retired construction worker sees his primary care physician for lower back pain and poor appetite. His past medical history is remarkable for hypertension and enlarged prostate. The physical examination is remarkable for a blood pressure of 100/60mmHg, a pulse of 90/min, and tenderness over his mid-lumbar spine and pitting edema over his shins. Urinalysis reveals specific gravity 1.015, pH 5.0, protein trace, blood trace. The protein content of a 24-hour urine collection is 6 grams. Which is the most likely cause of this patient's renal disease?
A-Obstruction of urinary flow due to an enlarged prostate
B- Acute tubular necrosis due to hypotension
C- Acute interstitial nephritis
D- Myeloma
E- Diabetes Mellitus
d
A 30-year-old man with type I diabetes mellitus for 25 years developed proteinuria about 15 years ago; this reached the nephrotic range about 10 years ago, and despite treatment, he has continued to excrete > 5 grams of protein per day. His renal function was normal 15 years ago, but 10 years ago his creatinine level rose to 1.5 mg/dl, 7 years ago was 2.1 mg/dl, 5 years ago was 2.7 mg/dl, 3 years ago it was 4.1 mg/dl, and one year ago it was 5.9mg/dl. He presents now with weight loss, nausea and vomiting, itching and severe fatigue. His blood pressure is 170/100mmHg, he has neck vein distention, rales, an S3 gallop, and peripheral edema. His skin is excoriated, and he is pale. His BUN is 110 mg/dl and her creatinine level are 8.8 mg/dl. Which of the following is the best chronic therapy for this patient?
A- Transplantation
B- Continuous ambulatory peritoneal dialysis
C- Hemodialysis
D- Continuous hemofiltration
E-New treatment for his diabetes
a
A 57-year-old woman with a ten-year history of hypertension comes to the hospital with a headache. Her blood pressure is 250/120 mm Hg. Her urine analysis shows 2+ proteinuria and 2+ hematuria. His serum creatinine is 2.3mg/dL and the BUN is 30 mg/dl. Which of the following is the basic anatomic unit of the kidney responsible for this patient's renal disease?
A- The blood vessels
B- The glomerulus
C- The renal tubules
D- The renal interstitium
E- The collecting system
a
A 57-year-old woman with diabetes and diabetic nephropathy has chronic renal failure and is currently treated with hemodialysis, for 4 hours 3 times per week. On examination, you find her blood pressure to be 170/104mmHg. Her Na+ is 129mEq/L, K+ is 5.5 mEq/L, Cl- is 9'1 mEq/L, HC0 3- is19 mEq/L, BUN is 90 mg/dL, and creatinine is 8.6 mg/dL. The pH is 7.33. Which factor is most important in explaining her hypertension?
A-Decreased glomerular filtration of sodium
B-Glycosylation of her vascular smooth muscle cells increased renin and aldosterone levels
C-Anxiety related to his chronic illness
D-Osmotic shifts of fluid due to high BUN levels
a
Which of the following causes systolic hypertension?
A. acromegaly
B. thyrotoxicosis
C. renal artery stenosis
D. increased intracranial pressure
E. chronic renal failure
b
A 45-year-old woman has had increasing malaise for the past year. On physical examination her blood pressure is 265/150 mm Hg. Laboratory studies show a plasma renin activity of 9ng/mL/hr. She then suffers a 'stroke' with a right basal ganglia hemorrhage and dies. At autopsy the kidneys are bilaterally small with granular surfaces. Microscopically they show hyperplastic arteriolosclerosis with fibrinoid necrosis, petechial hemorrhages, and microinfarcts in the cortices. Which of the following conditions is most likely to be her underlying cause of death?
A-Diabetes mellitus, type II
B-Fibromuscular dysplasia
C-Factor V Leiden mutation
D-Analgesic abuse
E-Systemic sclerosis
b
Which of the following statements about angiotensin II is false?
A-It causes vasoconstriction of the efferent arteriole
B- It increases the amount of albumin filtered by the glomeruli
C- It is increased in renal acidosis
D- It increases aldosterone production
E-It is reduced in people with diabetes
b
__________ failure is caused by obstruction of urine flow. (urethral obstruction by enlarged prostate or tumor; ureteral or kidney pelvis obstruction by calculi)
A. Prerenal
B. Intrarenal
C. Postrenal
D. Perirenal
c
Agents that damage the kidney tissue are called:
A. Nephrons
B. Nephrotoxins
C. Antibodies
D. Enterotoxins
b
Acute renal failure is generally identified by oliguria (urine output <_____ mL/day).
400mL/day
4. The risk for __________________ is particularly high when ischemia and exposure to a nephrotoxin occur at the same time.
Acute tubular necrosis
6. The cause of ___________ failure is impaired blood supply to the kidney (Fluid Volume
Deficit, hemorrhage, heart failure, shock)
A. Prerenal
B. Intrarenal
C. Postrenal
D. Perirenal
a
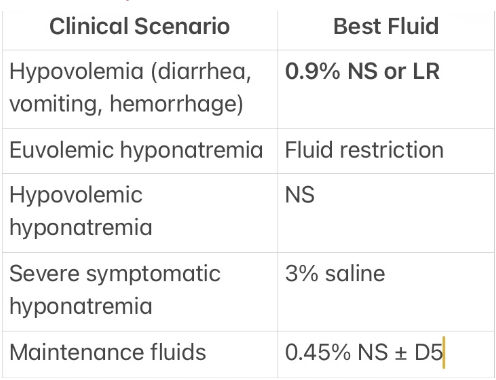
A 19-year-old man presents to the ED today after 3 days of severe diarrhea. His blood pressure in the supine position i s 100/60 and his heart rate is 90 beats per minute. His upright blood pressure drops to 80/50, and his heart rate increases to 110 beats per minute, and he complains of feeling dizzy and nauseous. His serum sodium i s 138 mEq/L. (NV Nat 135-145mEq/l.)
Which of the following is the most appropriate replacement fluid?
A . IV 0.9% saline
B . IV 0.45% saline
C . IV 5% dextrose
D. IV 3% saline
E. Chicken soup
a. IV 0.9% saline
Why?:
- isotonic → stays in the Extracellular space
Expands intravascular volume
first-line for hypovolemic shock or orthostasis
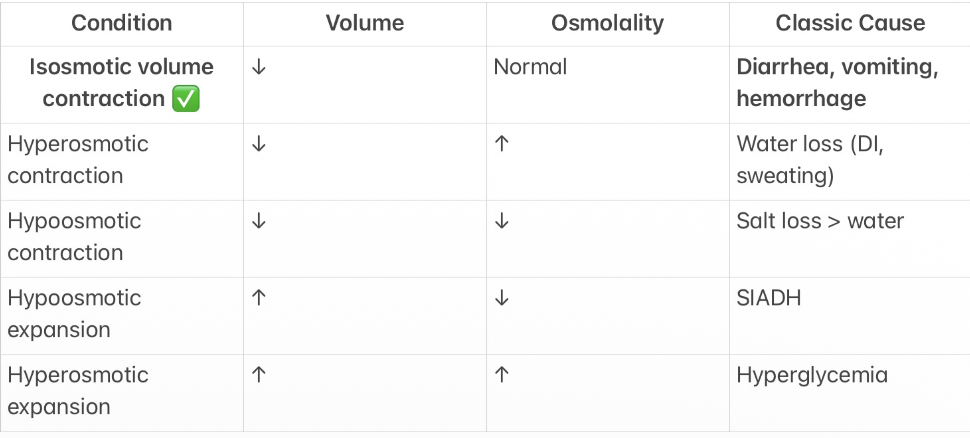
A n 8-year-old boy is bringing to Emergency Room because two days o f diarrhea.
Which of the following is his fluid and electrolytes condition?
A- Isosmotic volume contraction
B- Hyperosmotic volume contraction
C- Hypoosmotic volume expansion
D- Osmotic volume expansion A
A- Isosmotic volume contraction
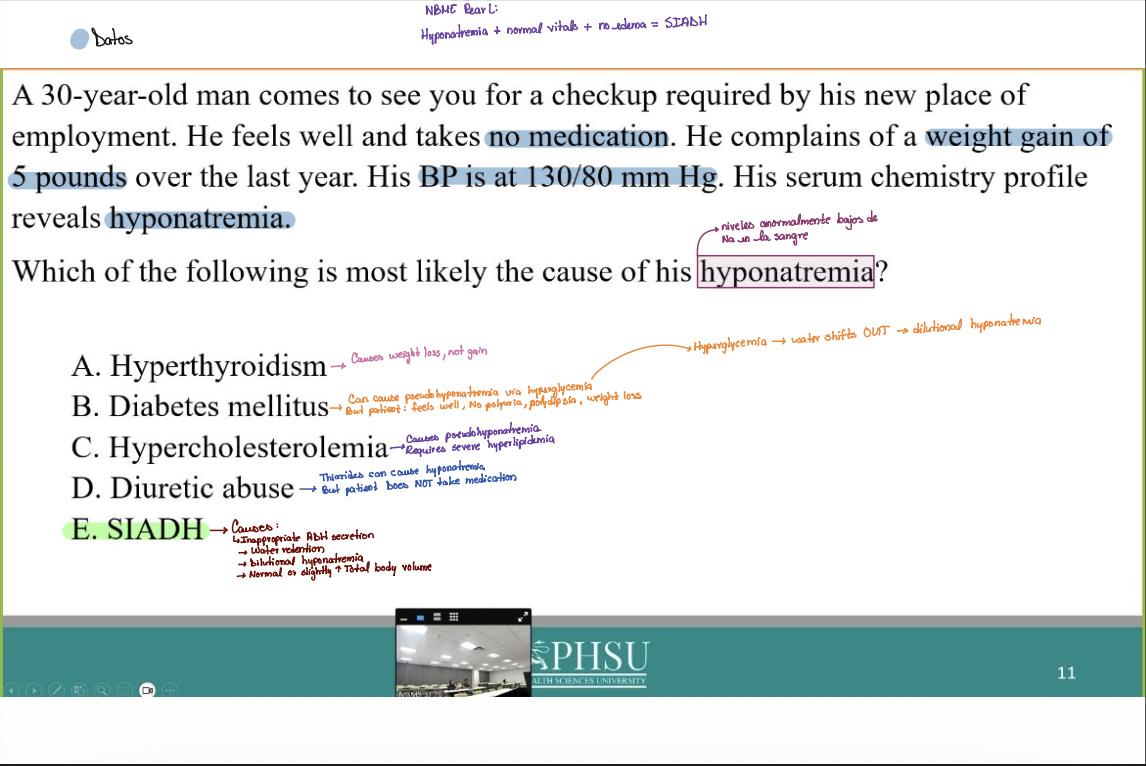
A 30-year-old man comes to see you for a checkup required by his new place of employment. H e feels well and takes no medication. He complains of a weight gain of 5 pounds over the last year. His BP is at 130/80 mm Hg. His serum chemistry profile reveals hyponatremia.
Which of the following is most likely the cause of his hyponatremia?
A . Hyperthyroidism
B. Diabetes mellitus
C . Hypercholesterolemia
D. Diuretic abuse
E. SIADH
E. SIADH
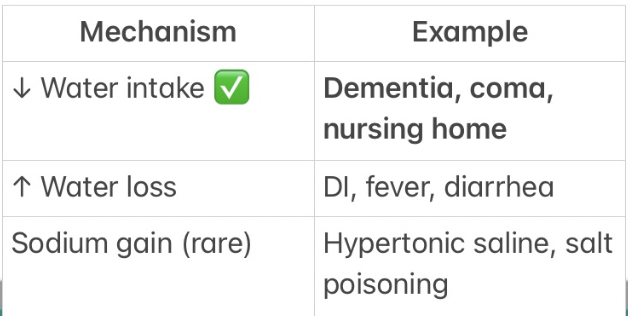
An 87-year-old woman with Alzheimer disease is referred to ED from his nursing home with a urinary tract infection. She has profound dementia, is nonverbal and makes no purposeful movements. She has a temperature of 98° F, a BP of 148/90mm/Hg, a RR of 12/minute, and a HR of 88/minute. She is emaciated and cachectic. Cloudy urine, which seems grossly infected, drains from an indwelling urinary catheter. A serum sodium is drawn and is 154 mE/L.
The single most important contributor to her high serum sodium level is:
A- Water loss from insensible losses
B - An inability to excrete sodium from his urine due to urinary obstruction
C - Decreased water intake
D- Shift of sodium into the extracellular space
E - Increased dietary intake of sodium
C - Decreased water intake
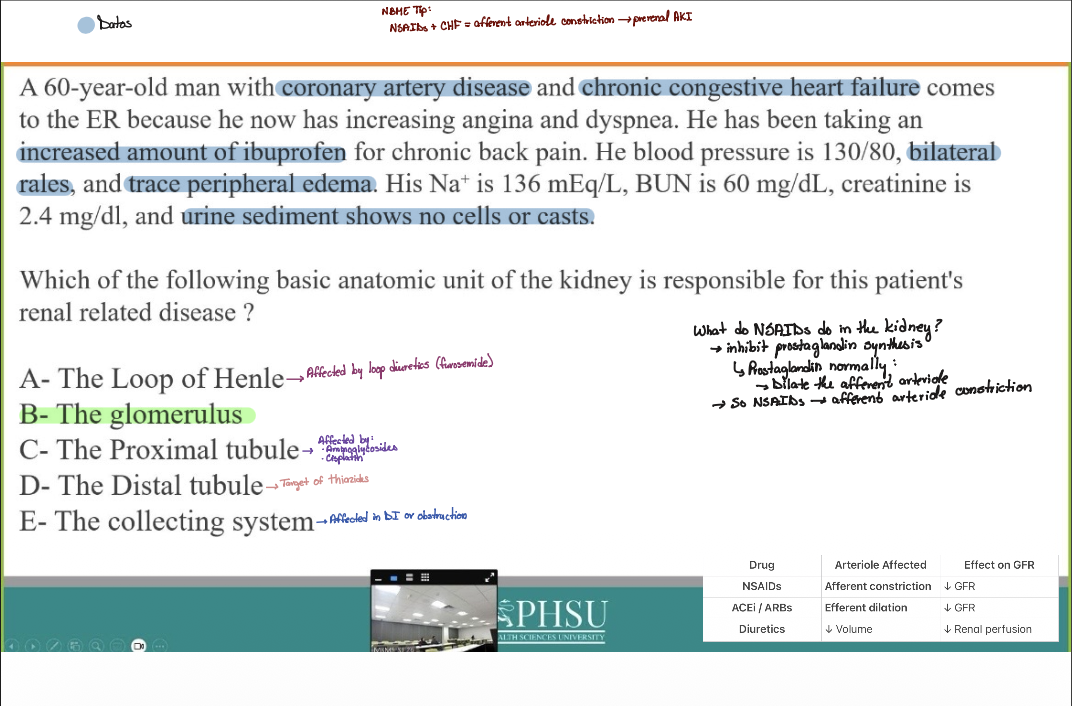
A 60-year-old man with coronary artery disease and chronic congestive heart failure comes to the ER because he now has increasing angina and dyspnea. H e has been taking an increased amount of ibuprofen for chronic back pain. He blood pressure is 130/80, bilateral rales, and trace peripheral edema. His Na+ is 136 mEq/L, BUN is 60 mg/dL, creatinine is 2.4 mg/dl, and urine sediment shows no cells or casts.
Which of the following basic anatomic unit of the kidney is responsible for this patient's renal related disease?
A- The Loop of Henle
B- The glomerulus
C- The Proximal tubule
D - The Distal tubule
E- The collecting system
B- The glomerulus
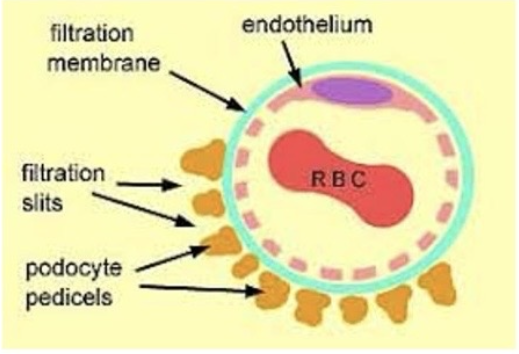
What structure in the figure is the most important in the regulation of the
passage of proteins from the vascular space to the urinary space?
Glomerular filtration membrane
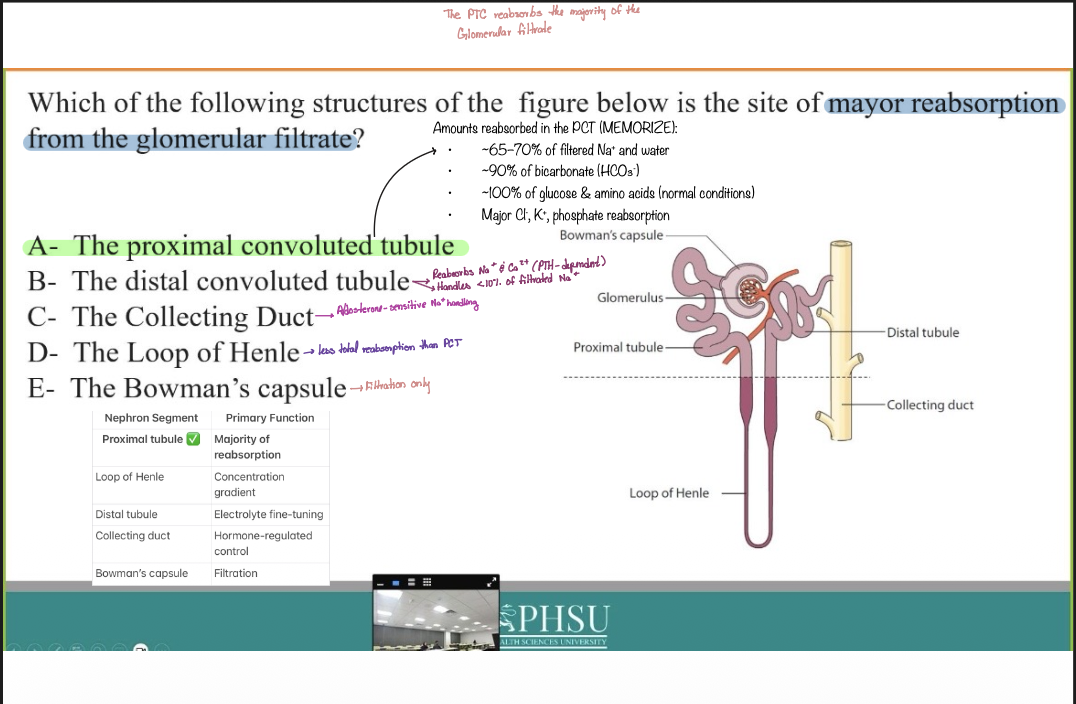
Which of the following structures of the figure below is the site of mayor reabsorption from the glomerular filtrate?
A- The proximal convoluted tubule
B- The distal convoluted tubule
C- The Collecting Duct
D- The Loop of Henle
E - The Bowman's capsule
A- The proximal convoluted tubule
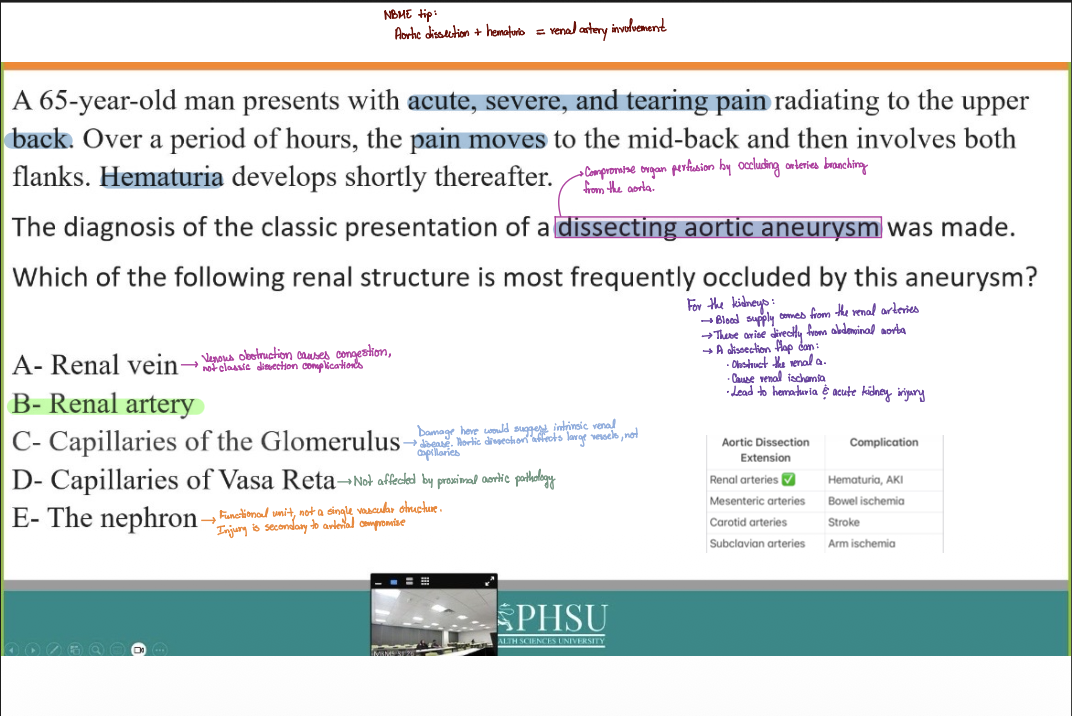
A 65-year-old man presents with acute, severe, and tearing pain radiating to the upper back. Over a period of hours, the pain moves to the mid-back and then involves both flanks. Hematuria develops shortly thereafter. The diagnosis of the classic presentation of a dissecting aortic aneurysm was made.
Which of the following renal structure is most frequently occluded by this aneurysm?
A- Renal vein
B- Renal artery
C - Capillaries of the Glomerulus
D - Capillaries of Vasa Reta
E - The nephron
B- Renal artery
A researcher observes a consistent 75% decrease in renal blood flow in subjects performing maximal exercise.
Which of the following best accounts for the decreased flow?
A . Decrease in mean arterial pressure
B . Decrease in renal arterial pressure
C. Sweat-induced hypovolemia
D . Increased renal sympathetic nerve activity
E. Antidiuretic hormone release
D . Increased renal sympathetic nerve activity
A 36-year-old woman comes to your office with a 1-day history of burning sensation during urination and foul-smelling urine. She is sexually active with 1 partner, her husband, and he uses a condom for contraception. Fluid intake and blood glucose are normal. BP 135/95 mmHg. Leukocyte esterase dipstick test is positive, and urinalysis reveals 10 WBC/ml and bacteria.
Which of the following is a risk factor for this patient's condition?
A- Length of the urethra
B- Renal disease
C- Condom use
D - Hypertension
E - Treatment with diuretics
A- Length of the urethra
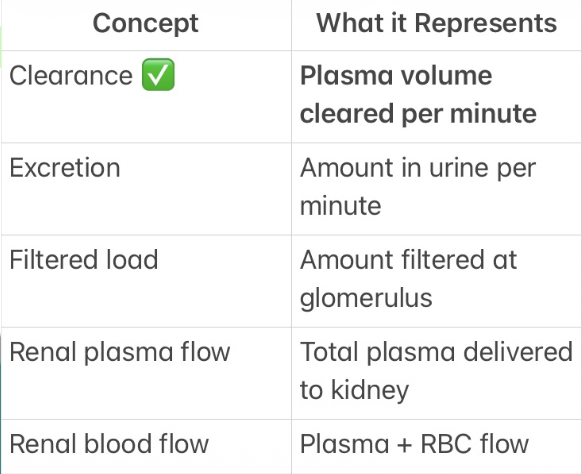
A 45-year-old man with a history of nephrolithiasis presents to ER with acute
right flank pain. A creatinine clearance assessment is performed.
Which of the following best equates with "Creatinine clearance"?
A. Renal blood flow
B. Renal plasma flow
C. Amount of creatinine traversing the glomerulus per minute
D. Amount of creatinine entering the urinary bladder per minute
E. Plasma volume completely cleared of creatinine per minute
E. Plasma volume completely cleared of creatinine per minute
Creatinine clearance = the volume of plasma that is completely cleared of creatine per unit time
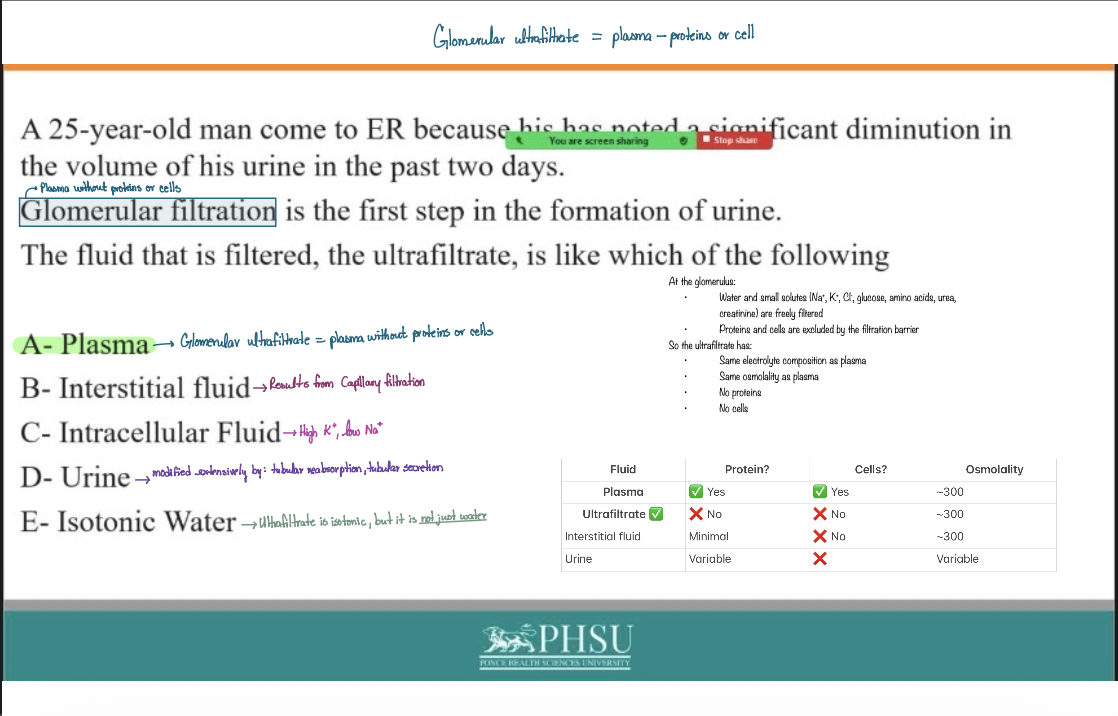
25-year-old man come to ER because his has noted, 2 significant diminution in the volume of his urine in the past two days. Glomerular filtration is the first step in the formation of urine.
The fluid that is filtered, the ultrafiltrate, is like which of the following
A- Plasma
B- Interstitial fluid
C- Intracellular Fluid
D - Urine
E- Isotonic Water
A- Plasma
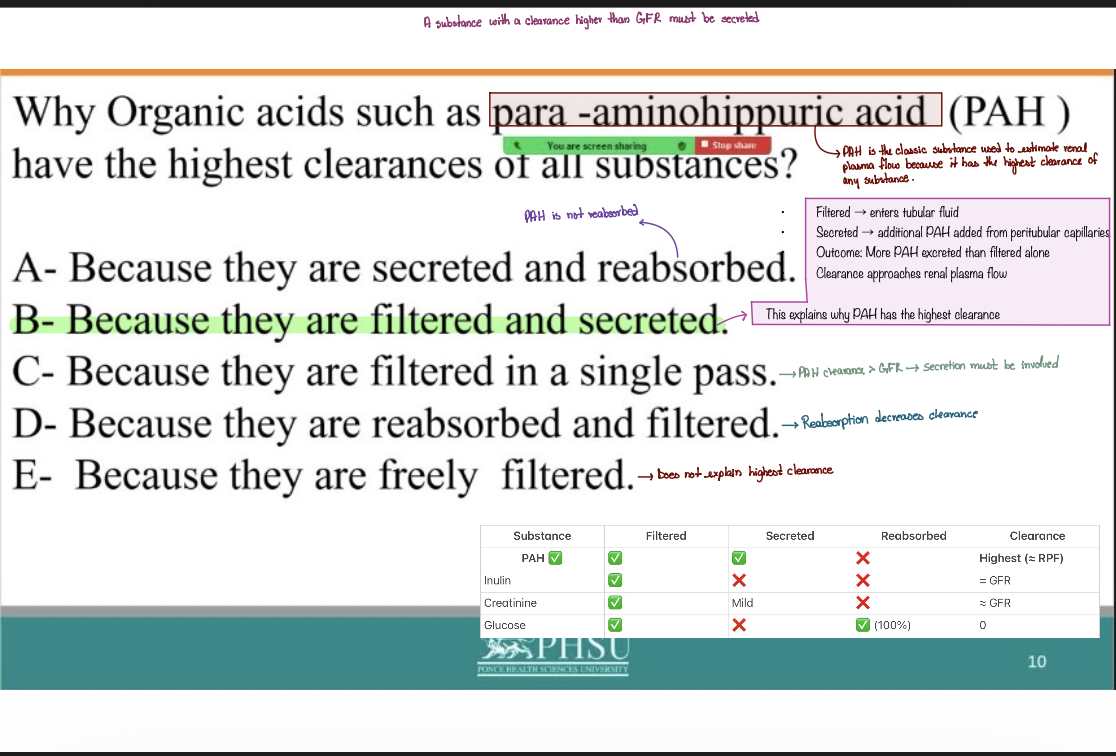
Why Organic acids such as para -aminohippuric acid (PAH) have the highest clearances of all substances?
A - Because they are secreted and reabsorbed.
B - Because they are filtered and secreted.
C - Because they are filtered in a single pass.
D- Because they are reabsorbed and filtered.
E - Because they are freely filtered.
B - Because they are filtered and secreted.
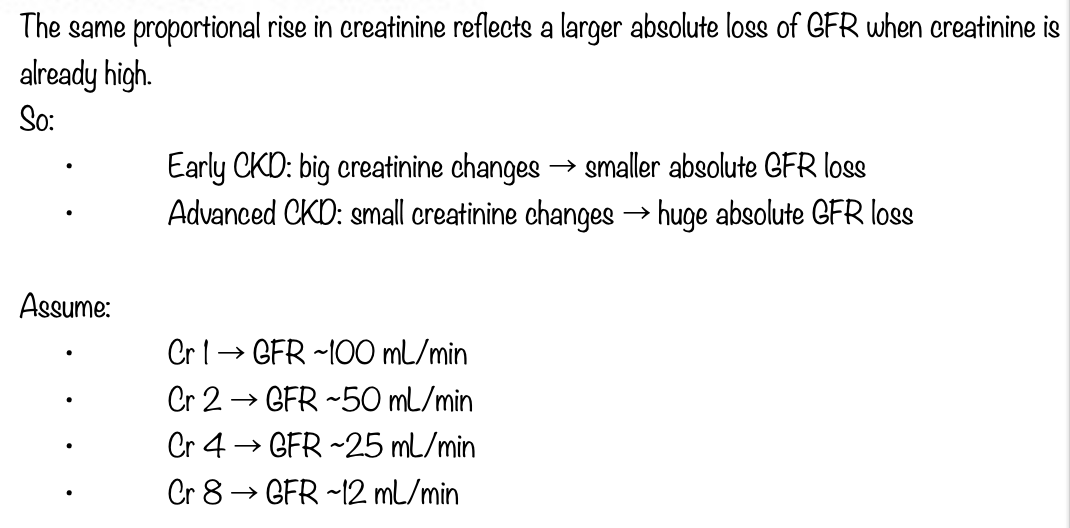
A 57-year-old woman come to your office for a follow up because you are treating her for a progressive, chronic kidney disease.
Which of the following indicates the greatest absolute decrease in GFR?
A . Fall in plasma creatinine from 4 to 2 mg/dL
B. Fall in plasma creatinine from 2 to 1 mg/dL
C. Rise i n plasma creatinine from 1 t o 2 mg/dL
D. Rise in plasma creatinine from 2 t o 4 mg/dL
E . Rise in plasma creatinine from 4 t o 8 mg/dL
E . Rise in plasma creatinine from 4 t o 8 mg/dL
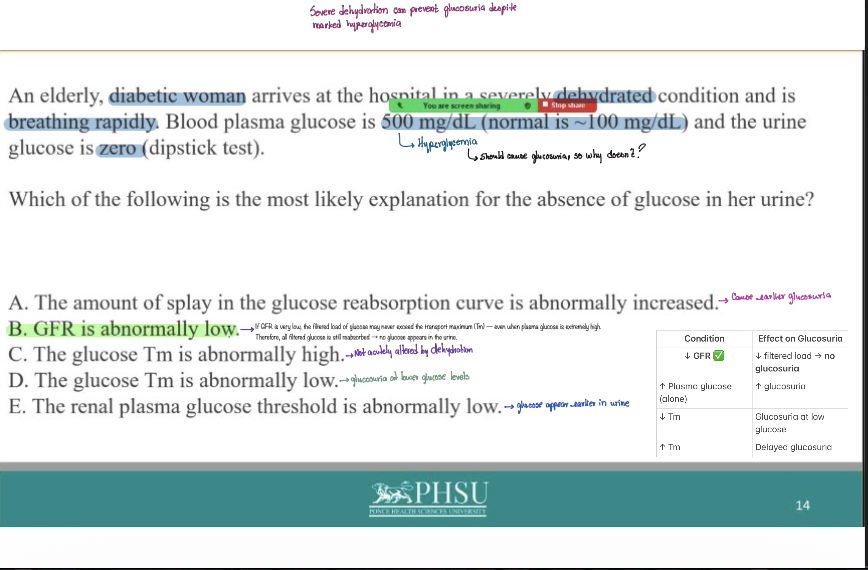
An elderly, diabetic woman arrives at the hospital in a severely dehydrated condition and is breathing rapidly. Blood plasma glucose is 500 mg/dL (normal is ~ 100 mg/dL) and the urine glucose is zero (dipstick test).
Which of the following is the most likely explanation for the absence of glucose in her urine?
A . The amount of splay in the glucose reabsorption curve is abnormally increased.
B. GFR is abnormally low.
C . The glucose Tm is abnormally high.
D . The glucose Tm is abnormally low.
E. The renal plasma glucose threshold is abnormally low.
B. GFR is abnormally low.
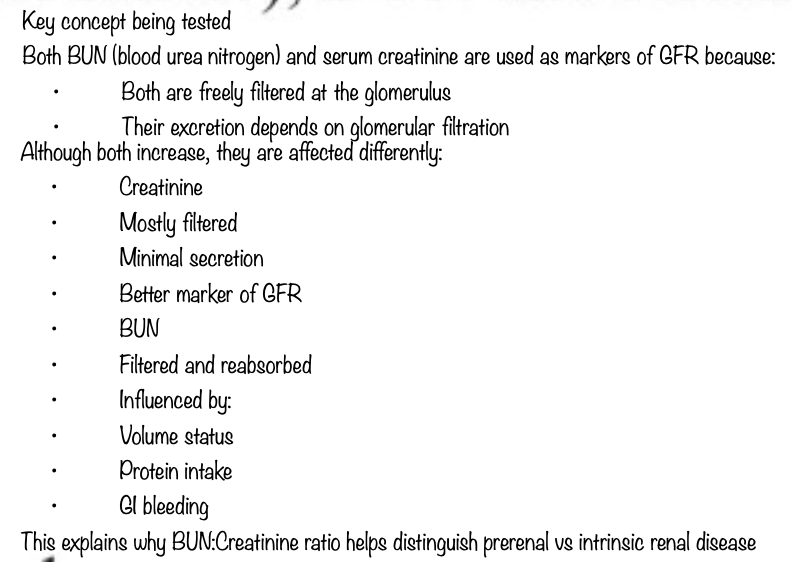
Both blood urea nitrogen (BUN) and serum creatinine concentration can be used to estimate GFR. They ? the glomerular capillaries and thus, each substance depends on the filtration step in order to be excreted in urine.
When there is a decrease in GFR (e.g., in renal failure), BUN and serum
creatinine
A- Both increase in serum.
B- Both decrease in serum.
C - BUN increase and Creatinine decrease.
D - Creatinine increase and BUN decrease.
E- They concentration in serum is not affected.
A- Both increase in serum.
A 7-year-old girl i s bringing b y her mother to the E R with sudden-onset lower extremity edema. The past 2 days, the patient's mother Said it began in the patient's feet and seems to be moving up his legs. She also reports that her daughter is urinating infrequently, but there is no gross blood in the urine. The patient is afebrile, and her vital signs are normal. Urinalysis and urine cytology reveal significant proteinuria (albumin only), with no red cells or casts.
Which of the following is most probably affected and is responsible for the renal problem in this patient?
A - The glomerular filtration apparatus.
B - The epithelial cell of the Proximal Tubule
C - The Collecting duct
D- The epithelial cell of the Distal Tubule
E - The long of the Hasa the Henle
A - The glomerular filtration apparatus.
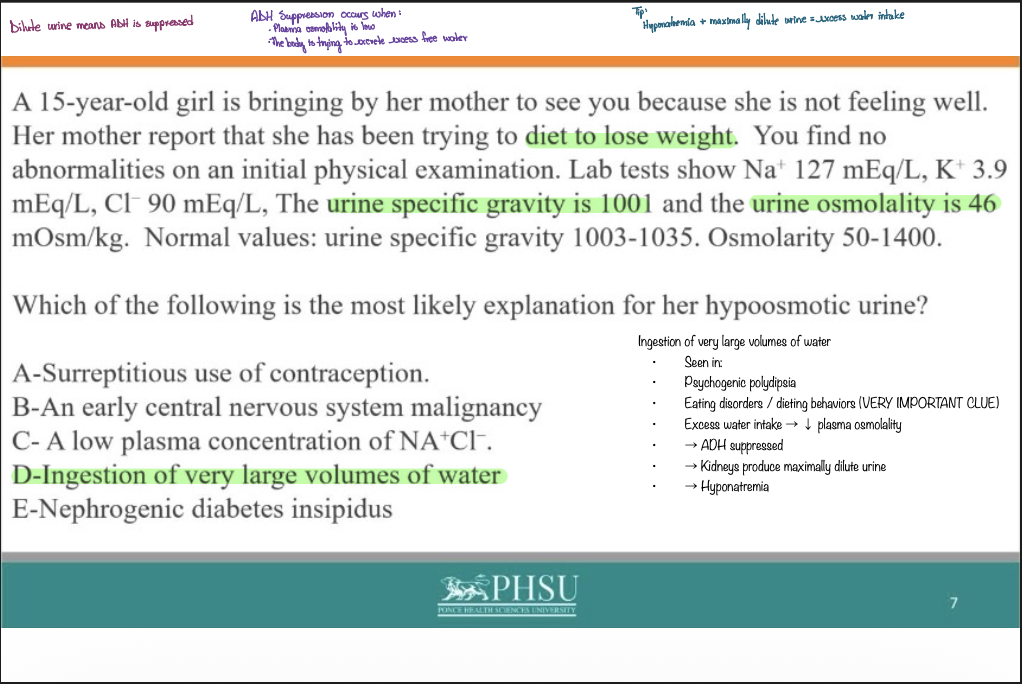
A 15-year-old girl is bringing by her mother to see you because she is not feeling well. Her mother report that she has been trying to diet to lose weight. You find no abnormalities on an initial physical examination. Lab tests show Na+ 127 mEq/L, K+ 3.9mEq/L, CI 90 mEq/L, The urine specific gravity is 1001 and the urine osmolality is 46 mOsm/kg. Normal values: urine specific gravity 1003-1035. Osmolarity 50-1400.
Which of the following is the most likely explanation for her hypoosmotic urine?
A - Surreptitious use of contraception.
B - An early central nervous system malignancy
C - A low plasma concentration of NA+CI.
D - Ingestion of very large volumes of water
E - Nephrogenic diabetes insipidus
D - Ingestion of very large volumes of water
Place the following in correct sequence from the following of a drop of urine to its elimination from the body: 1. major calyx, 2. minor calyx, 3. Glomerulus,
4. urethra, 5 . ureter, 6. collecting duct
A ) 3,1,2,6,5,4
B) 1,6,2,1,5,4
C) 2,1,3,6,5,4
D) 3,6,2,1,5,4
D) 3,6,2,1,5,4
The Vasa Recta participate in countercurrent exchange that helps maintain the cortico papillary osmotic gradient, and differs from countercurrent multiplication because countercurrent exchange is a purely
A - Active process
B - Passive process
C- ADH dependent process
D - Isosmotic process
E- Independent process
B - Passive process
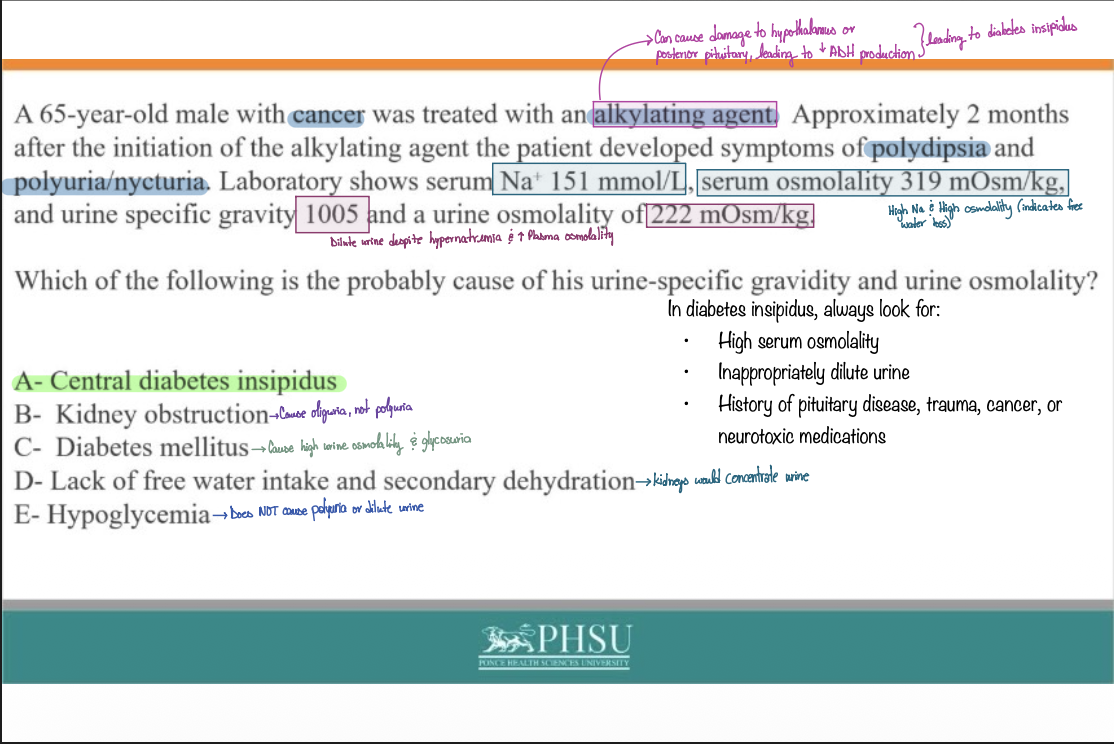
A 65-year-old male with cancer was treated with an alkylating agent. Approximately 2 months after the initiation of the alkylating agent the patient developed symptoms of polydipsia and polyuria/nycturia. Laboratory shows serum Na* 151 mmol/L, serum osmolality 319 mOsm/kg, and urine specific gravity 1005 and a urine osmolality of 222 mOsm/kg
Which of the following is the probably cause of his urine-specific gravidity and urine osmolality?
A - Central diabetes insipidus
B- Kidney obstruction
C - Diabetes mellitus
D - Lack of free water intake and secondary dehydration
E - Hypoglycemia
A - Central diabetes insipidus
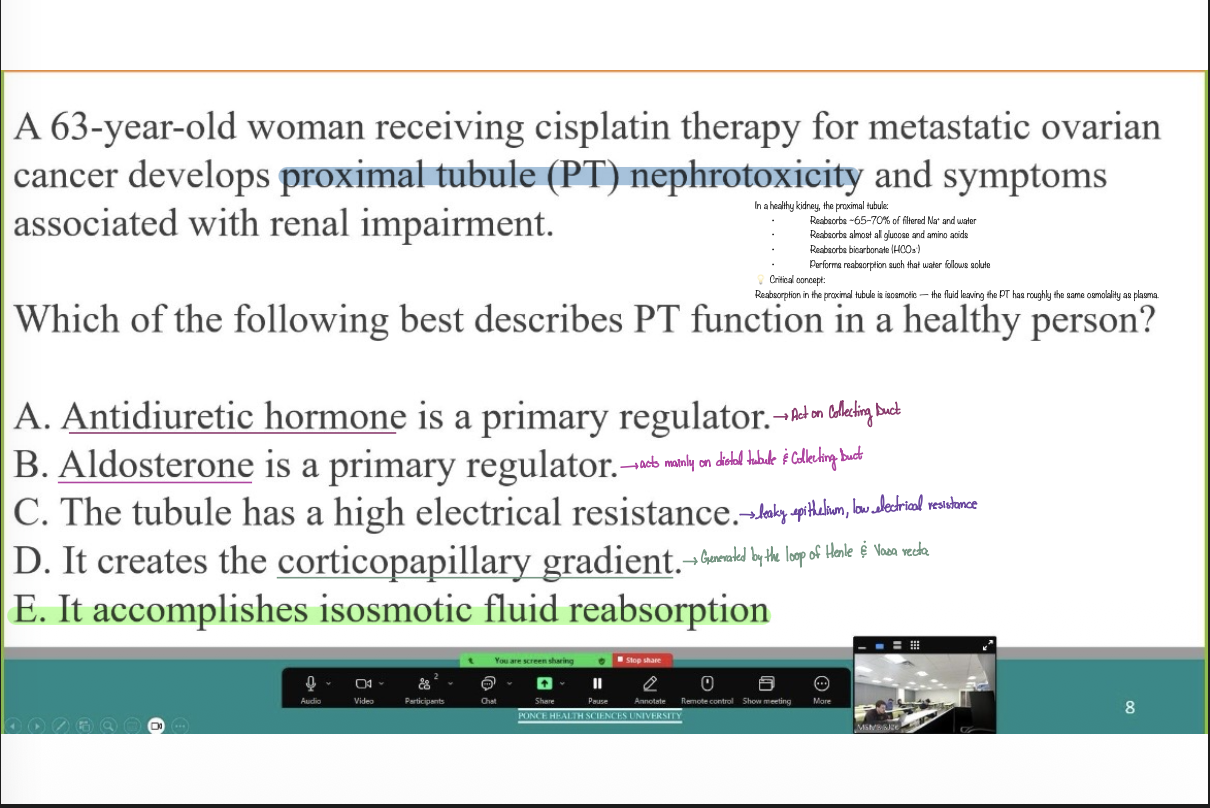
A 63-year-old woman receiving cisplatin therapy for metastatic ovarian cancer develops proximal tubule (PT) nephrotoxicity and symptoms associated with renal impairment.
Which of the following best describes PT function in a healthy person?
A . Antidiuretic hormone is a primary regulator.
B. Aldosterone is a primary regulator.
C. The tubule has a high electrical resistance.
D. It creates the corticopapillary gradient.
E. It accomplishes isosmotic fluid reabsorption
E. It accomplishes isosmotic fluid reabsorption
Na+ reabsorption by the proximal tubule is an example of the
transcellular pathway. It depends on the operation of the
A - Na+-Ca + -ATPase pump.
B - Nat- CI--ATPase pump.
C- Na+-K+-ATPase pump.
D- Kt- CI-ATPase pump.
E- Kt- Cat+- ATPase pump.
C- Na+-K+-ATPase pump.
A 19-year-old male college student decides to eat chile soup and chips for lunch. He is late for track practice, so he has no time to drink water and forgets to bring any with him. The weather is warm and dry. He doesn't sweat much but feels very thirsty.
Which of the following you expect most probably to occur?
A - Total urinary Nat excretion will fall because of his lack of water.
B - He has orthostatic hypotension, because of large insensible losses.
C - The level of ADH will be high.
D- The collecting tubules reabsorbs water to allow for concentration of urine.
E - The ascending loop of Henle will turn off allowing for dilution of urine.
C - The level of ADH will be high.
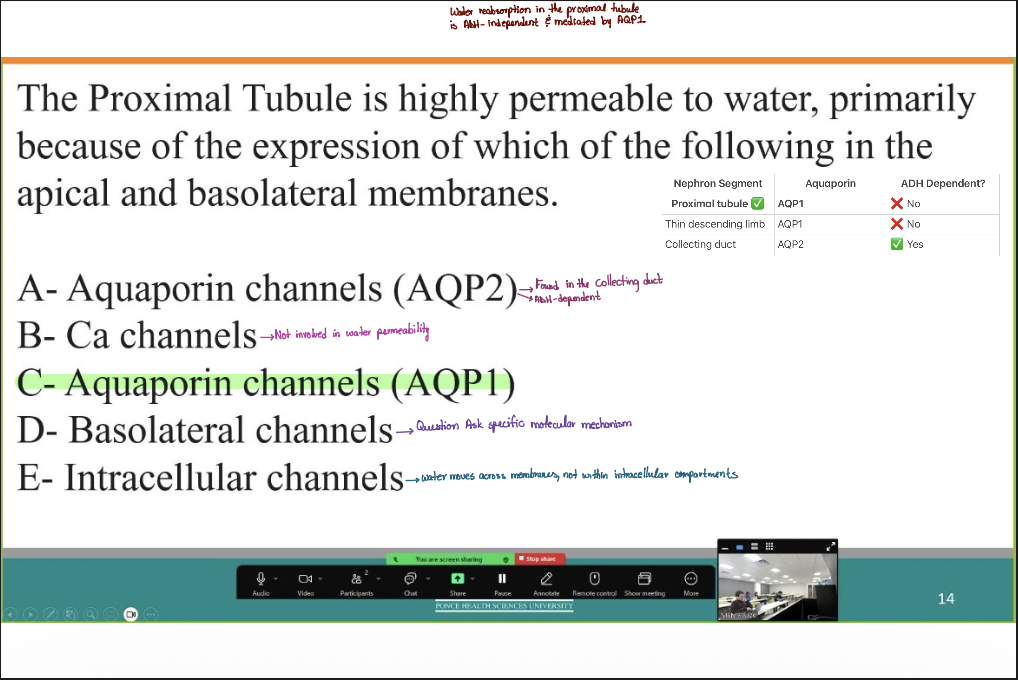
The Proximal Tubule is highly permeable to water, primarily because of the expression of which o f the following in the apical and basolateral membranes.
A- Aquaporin channels (AQP2)
B - C a channels
C- Aquaporin channels (AQP1)
D - Basolateral channels
E- Intracellular channels
C- Aquaporin channels (AQP1)
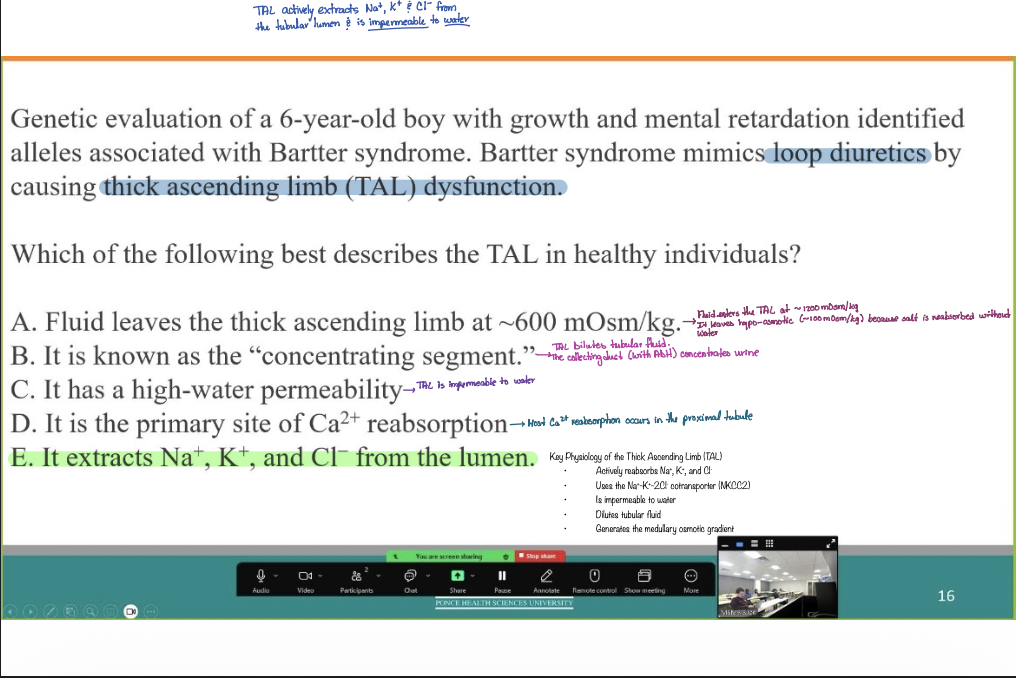
Genetic evaluation of a 6-year-old boy with growth and mental retardation identified alleles associated with Bartter syndrome. Bartter syndrome mimics loop diuretics by causing thick ascending limb (TAL) dysfunction.
Which of the following best describes the TAL in healthy individuals?
A. Fluid leaves the thick ascending limb at ~600 mOsm/kg.
B. It is known as the "concentrating segment."
C. It has a high-water permeability
D . It is the primary site of Ca+ reabsorption
E. It extracts Na+, K+, and CI from the lumen.
E. It extracts Na+, K+, and CI from the lumen.
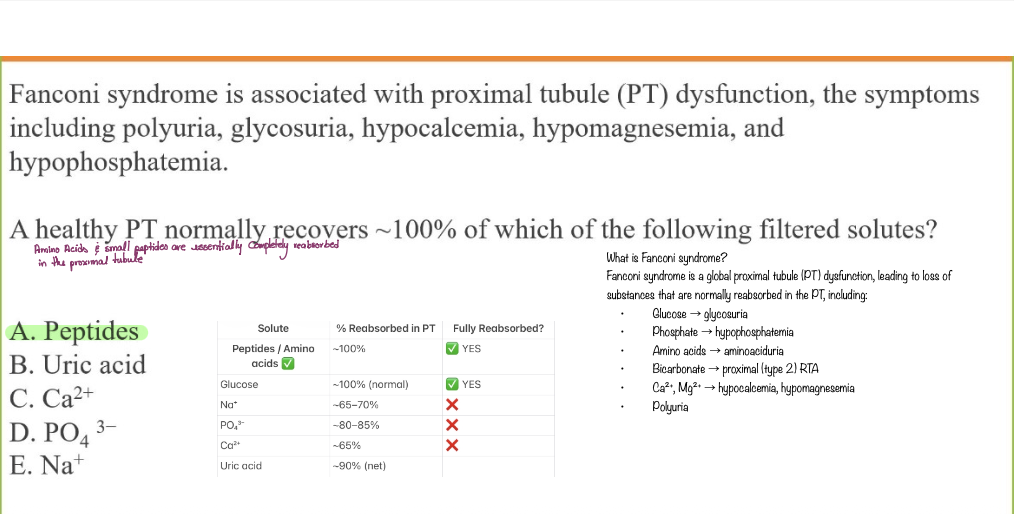
Fanconi syndrome is associated with proximal tubule (PT) dysfunction, the symptoms including polyuria, glycosuria, hypocalcemia, hypomagnesemia, and hypophosphatemia.
A healthy PT normally recovers ~100% of which of the following filtered solutes?
A. Peptides
B . Uric acid
C. Ca2+
D. PO4 3
E. Na+
A. Peptides
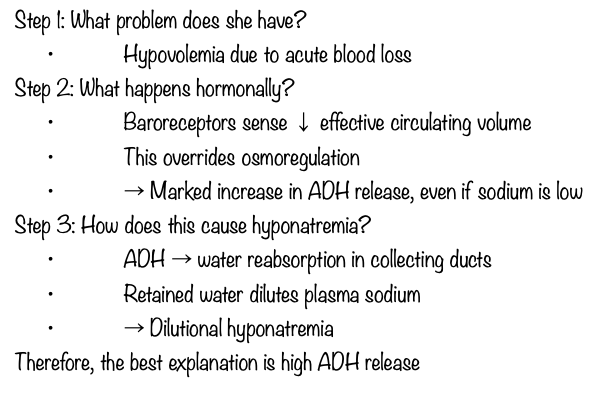
A 60-year-old woman with no medical history comes to see you complains of chronic joint aches and pains with gardening. She is prescribed ibuprofen 800 mg p/o which adequately controls her symptoms. One month later, she presents with multiple episodes of hematemesis. The patient Is thirsty and dizzy. Her HR 115/min, BP 96/64 mmHg.
Laboratory: Na* 130mEq/L
BUN 20 mg/dl
Creatinine 1.3 mg/dl
HCT 27%
Which of the following could best explain her hyponatremia?
A- High release of ADH
B - Low release of ADH
C- Hypovolemia due to blood loss with excessive water intake
D - NSAID induced inhibition of prostaglandin
E- Excess sodium loss with vomiting of blood
A- High release of ADH
A medical student gobbles a snack of bananas, potato chips, and a chocolate bar with nuts, and washes it down with orange juice.
Which of the following mechanisms is responsible to handle it.
A- Decrease of aldosterone secretion.
B - Decrease in proximal K+ reabsorption.
C - Increase of ADH.
D - Decrease of ADH.
E- Increase in insulin secretion.
E- Increase in insulin secretion.
To maintain K + balance, urinary excretion of K + must be equal to K + intake. The renal mechanisms that allow for this variability are called
A - External K+ balance
B- Internal K+ balance
C- Extracellular balance
D- Intracellular balance
E- External Na+- K+ balance
A - External K+ balance
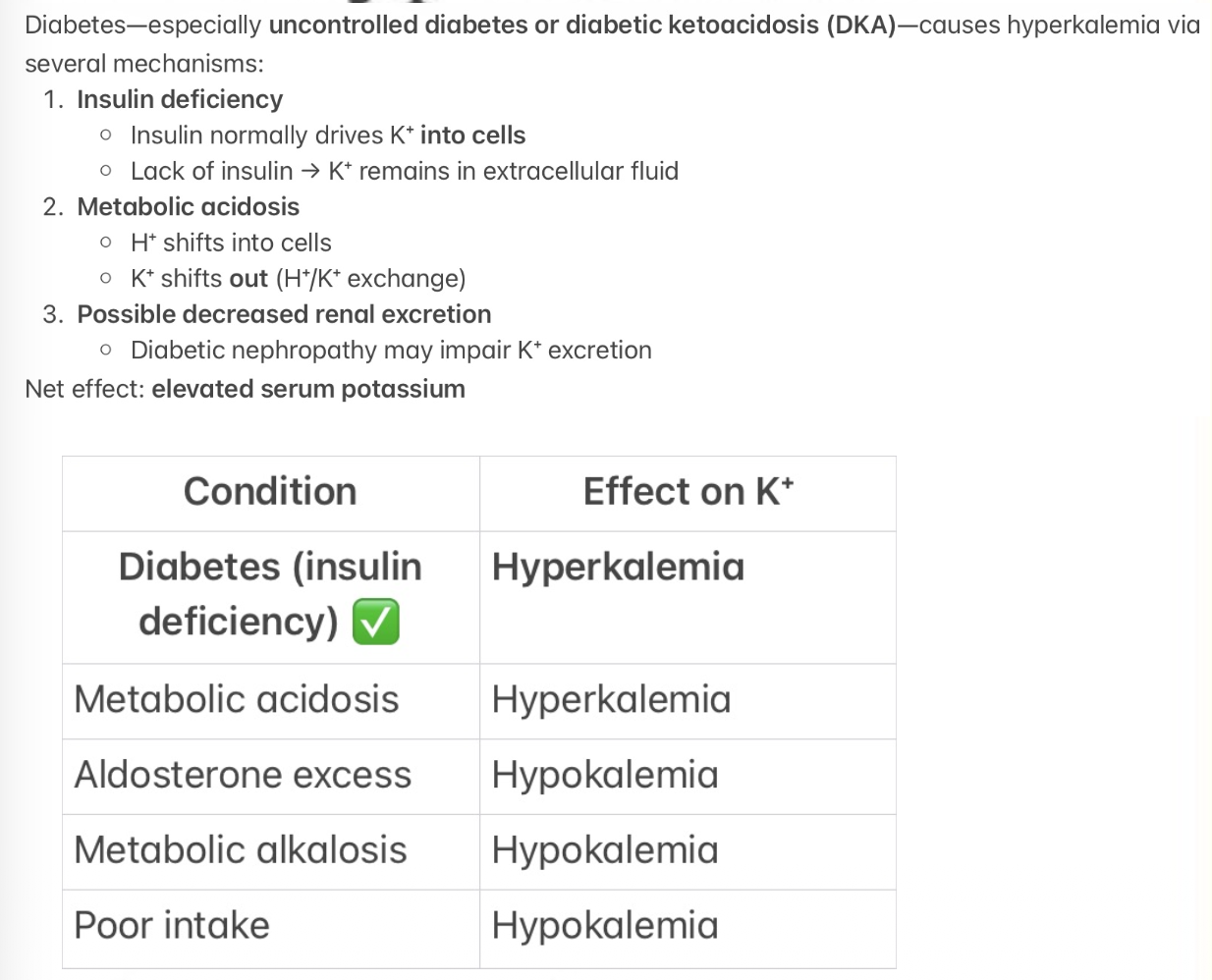
A 65-year-old woman presents to your office with nausea, vomit and a heart
rate of 138 beats per minute. Her chemistry panel is significant for a potassium of 5.7 mEq/L.
Which of the following conditions could be the cause of her hyperkalemia?
A-Dietary deficiency of potassium
B - Hyperthyroidism
C- Excess of Aldosterone
D - Diabetes
E - Metabolic alkalosis
D - Diabetes
A 24-year-old women come to your office because the last week she has
constipation, fatigue and palpitations.
Which of the following is the mayor responsible for K+ excretion?
A - Rate of tubular excretion o f Mg+
B - Amount of Na+ delivered to tubules
C- Rate of tubular secretion of H+
D - Aldosterone
E- Amount of Ca+ delivered to tubules
D - Aldosterone
To preserve electro neutrality, H + cannot enter o r leave cells by itself; it
must be accompanied by an anion or exchanged for another cation.
When H + is exchanged for another cation, which of the following is that
cation
A- Cat+
B- Mgt+
C- Na+
D-K +
E- NH4+
D-K +
Ca2+ reabsorption is tightly coupled to Na treabsorption, where is the
reabsorption of the two ions dissociated?
A- Proximal tubule
B - Loop of Henle
C - Distal tubule
D- Collecting Ducts
E - Thick ascending limb
C - Distal tubule
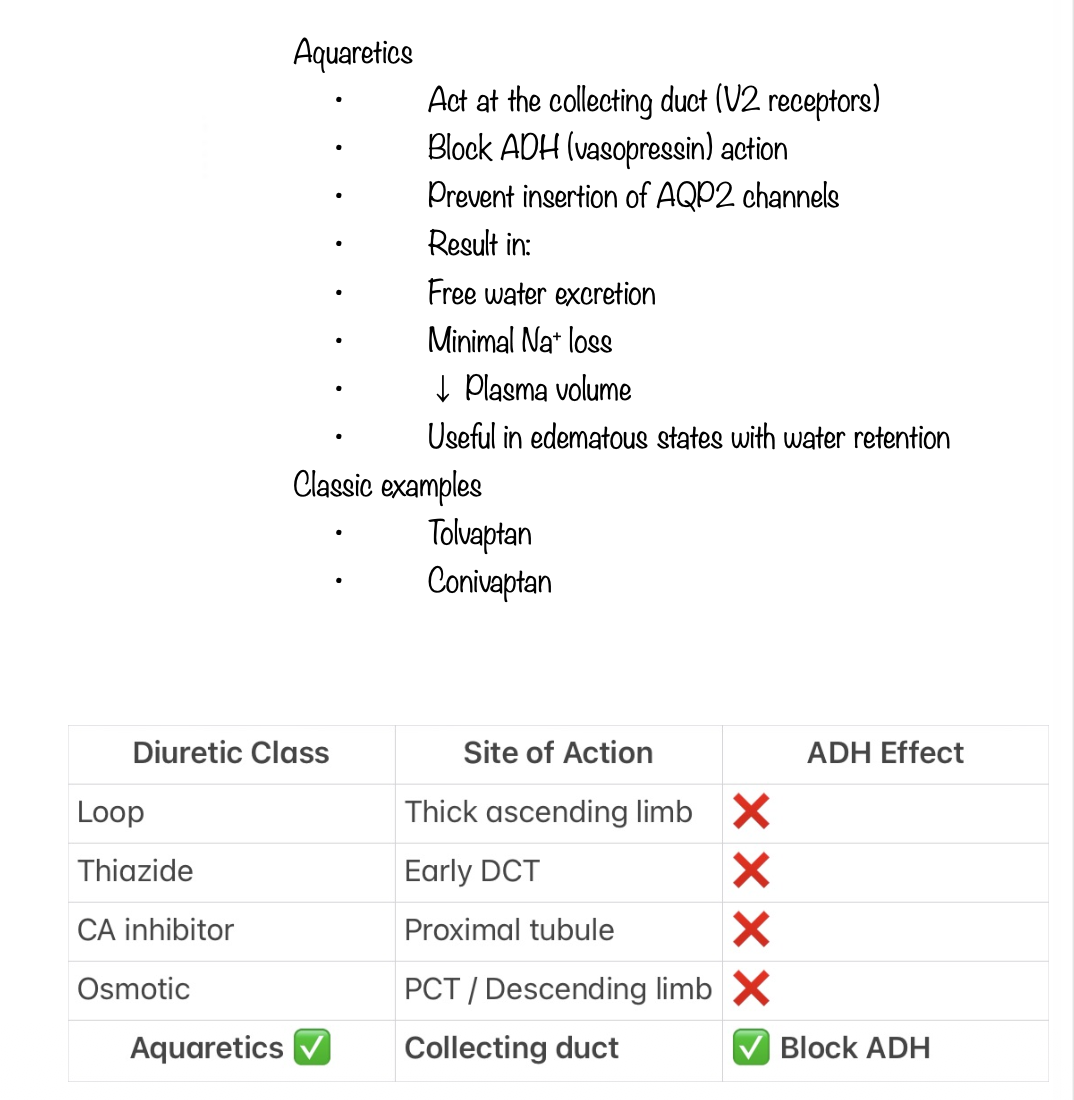
A patient with edema on the legs (++) by stasis is taking a diuretic that act on the late portion of the DT and the collecting duct to block the action of ADH.
Which of the following is the diuretic his is taking?
A-Thiazide Diuretics
B - Carbonic Anhydrase Inhibitors
C - Osmotic Diuretics
D - Aquaretics
E- Loop Diuretics
D - Aquaretics
Which of the following causes a decrease in renal Cat clearance?
A. Hypoparathyroidism
B. Treatment with chlorothiazide
C . Treatment with furosemide
D. Extracellular fluid (ECF) volume expansion
E . Hypermagnesemia
B. Treatment with chlorothiazide
A 64-year-old woman suffer from hypertension since 2005, now she is well controlled because her doctor prescribe to her the most potent diuretic available, that increase the excretion of Na+ to as much as 25% of the amount filtered.
Which of the following is the diuretic prescribed?
A-Thiazide Diuretics
B - Loop Diuretics
C - Osmotic Diuretics
D- Aquaretics
E- Carbonic Anhydrase Inhibitors
B - Loop Diuretics
A man who take for his hypertension a diuretic come to see you, complain of constipation, palpitations, fatigue and muscle weakness.
Which of the following is the medication implicated?
A- Osmotic Diuretics
B- Carbonic Anhydrase Inhibitors
C - Thiazide Diuretics
D - Aquaretics
E- Loop Diuretics
C - Thiazide Diuretics
A 60-year-old woman presents t o your office with weakness, constipation and a heart rate of 108 beats per minute. Her chemistry panel is significant for a potassium of 6.0 mEg/L.
Which of the following could be the cause of her hyperkalemia?
A. Hyperaldosteronism
B . Metabolic alkalosis
C. Spironolactone
D . Furosemide
E. Hyperthyroidism
C. Spironolactone
An 88-year-old patient is admitted t o your unit for CHF. The prescriber
orders IV furosemide. This patient has an increased risk for which of the
following furosemide's adverse effects?
a. Hyperuricemia
b. Vascular thrombosis
c . Headache
d . Photosensitivity
a. Hyperuricemia
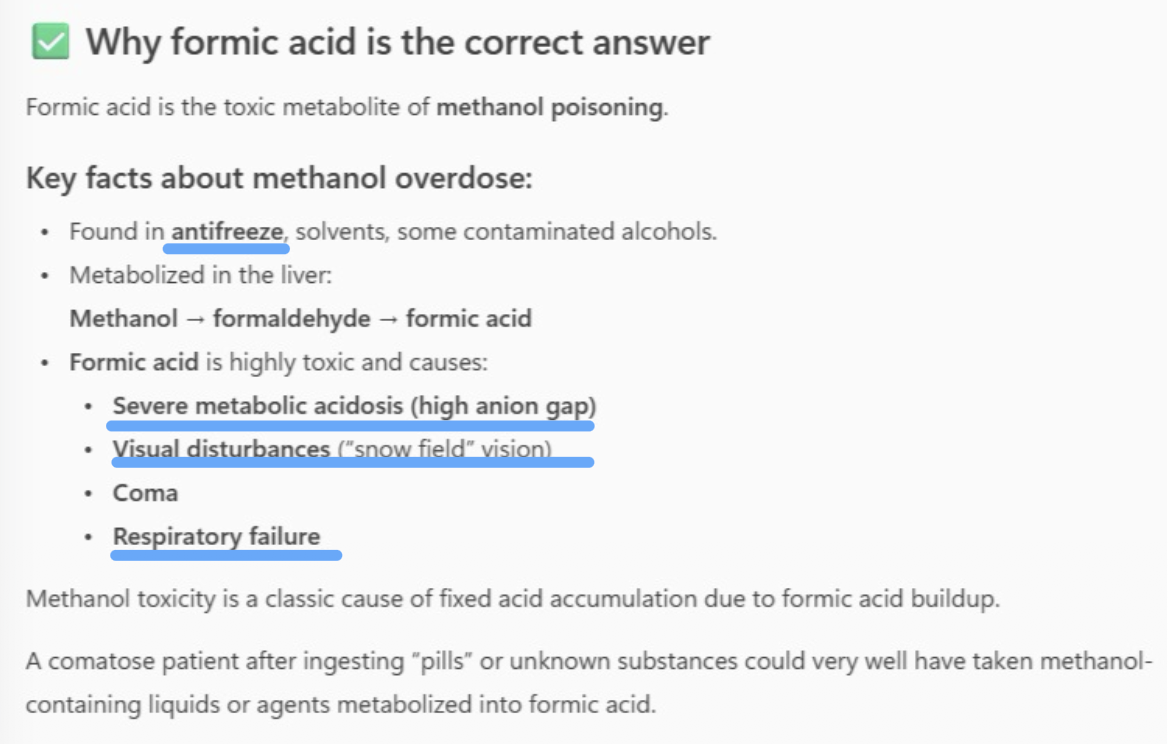
A young woman is found comatose, having taken an unknown number of
some pills two hours before. Which of the following fixed acids may be
implicated?
A- Lactic acid
B-B-hydroxybutyric acid
C- Acetoacetic acid
D - Salicylic acid
E- Formic acid
E- Formic acid
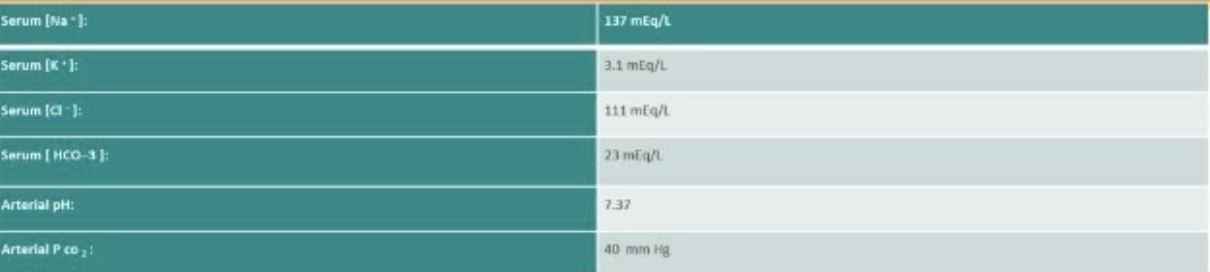
A previously healthy 28-year-old man with severe right flank pain is seen in the emergency department. Shortly after arrival, he passes a kidney stone. He reports that several people in his family also have had kidney stones.
The above laboratory data are obtained. Which of the following is the plasma anion gap?
A- 134
B- 3
C- 27
D - 3 6
E- 23
B- 3
Anion Gap=Na+−(Cl−+HCO3−)
Anion Gap=137−(111+23)
Anion Gap=137−134
Anion Gap=3
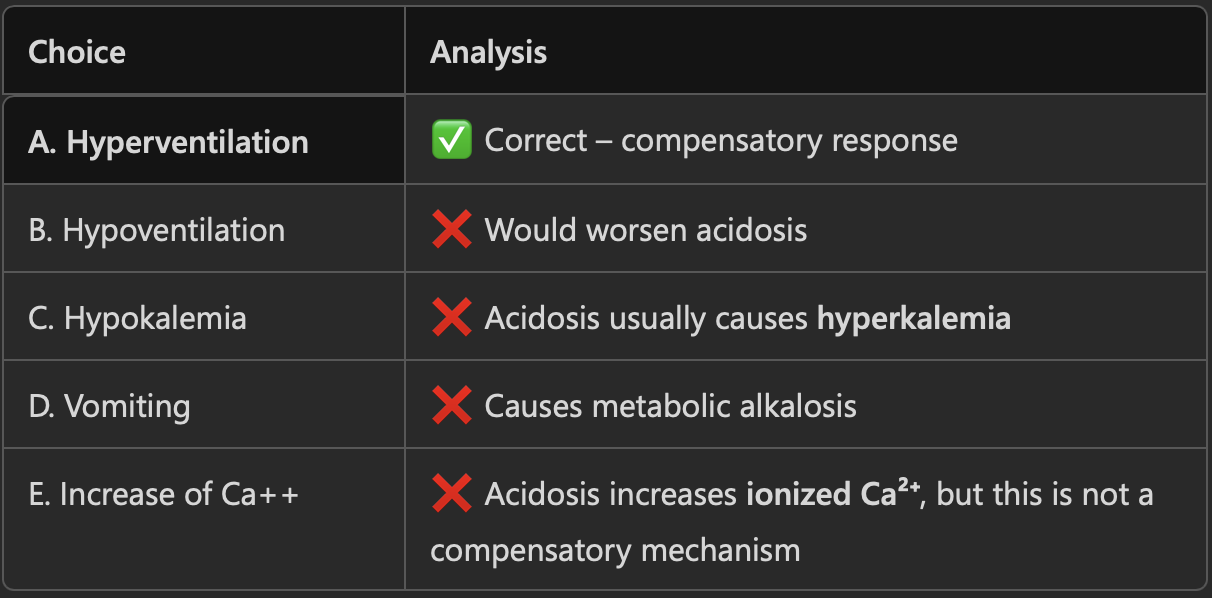
An elderly homeless woman is found unresponsive in the street, breathing rapidly. A blood gas analysis i s performed with these results: pH 7.29, pCO, 28 m m Hg, O2 saturation 96%, Nat 145 mEg/1, CI 90, HCO,- 12.
Which of the following is the appropriated response to her acidosis?
A . Hyperventilation
B . Hypoventilation
C . Hypokalemia
D. Vomiting
E . Increase of Ca++
A. Hyperventilation
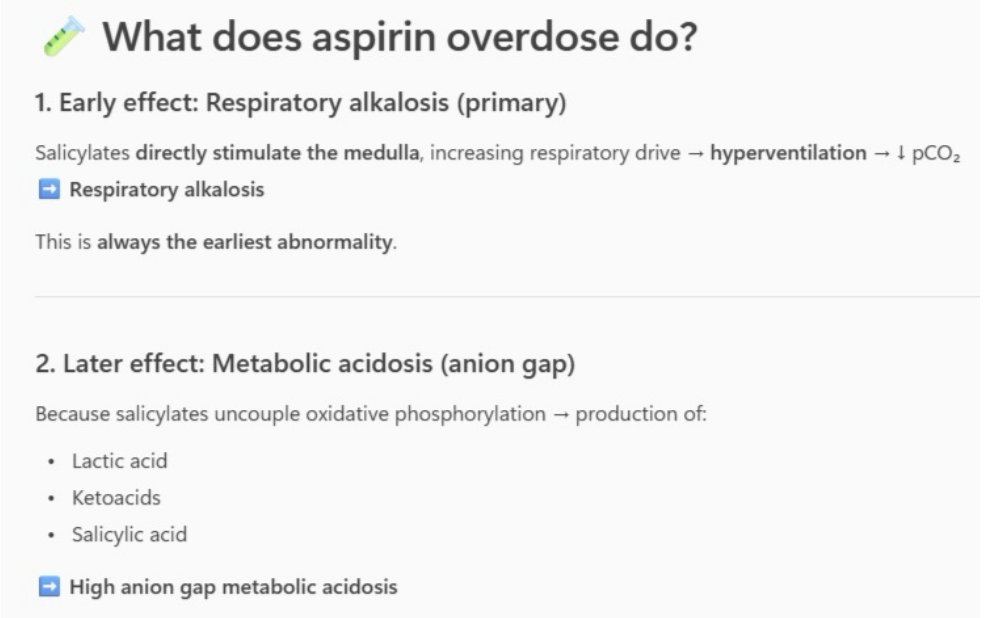
A young man is brought to ED by ambulance after attempting suicide.
He admits to being severely depressed and trying to end his own life by
taking a bottle of aspirin.
Which of the following abnormalities can we expect to see?
A . Respiratory acidosis
B. Respiratory alkalosis
C. Metabolic alkalosis
D. Hypercapnia and increase bicarbonate
E. Hypoxia and increased bicarbonate
B. Respiratory alkalosis
A 20-year-old woman is referred to you by the college health service because of abnormal blood tests, following her complaint of not feeling well. Her medical history is unremarkable, she takes no medications, and her examination is notable for a BP of 125/80, a HR o f 70/minute, clear lungs, a normal abdomen, and no edema. Arterial p H is 7.33, Na+ is 135 mEq/L, K* is 3.5 mEq/L, CI is 110 mEq/L, and HCO 3 is 16 mEq/L.
Which of the following is the most likely diagnosis?
A- Chronic renal failure
B- Aldosterone secreting tumor
C- Renal tubular acidosis
D- Early pregnancy
E- Excess ingestion of salicylates
C- Renal tubular acidosis
A 36-year-old man with a ten-year history of hypertension comes to the hospital with a headache. His blood pressure is 170/100 mm Hg. His urine analysis shows 2 + hematuria. His serum Cr i s 2.7 mg/dL, and the BUN is 3 4 mg/dl.
Which of the following abnormality would be expected to be present?
A . High serum K + level
B. Abnormal liver function tests
C. High level of ADH
D - High level of Proteinuria
E - High serum calcium level
D - High level of Proteinuria
Albuminuria marker for is one of the oldest and one of the most sensitive and widely used markers o f kidney dysfunction. Then, microalbuminuria is a
A- Malabsorption Syndrome
B - Diabetic nephropathy
C - Aldosteronism
D - Inappropriate secretion of ADH
E- Addison's disease
B - Diabetic nephropathy
A 35-year-old woman with type I diabetes mellitus for 25 years developed proteinuria. Her blood pressure i s 170/100, she has neck vein distention. rales, an S3 gallop, and peripheral edema. Lab: Nat 148mEq/l, K + 5mEq/1, CI 98mEq/l.
Which of the following could be the cause of her Hypernatremia?
A - Lesion of the Vasa Recta
B - Damage to collecting ducts
C- Changes in the countercurrent exchange
D- Damage of glomerulus
E- Destruction of the macula densa
A - Lesion of the Vasa Recta
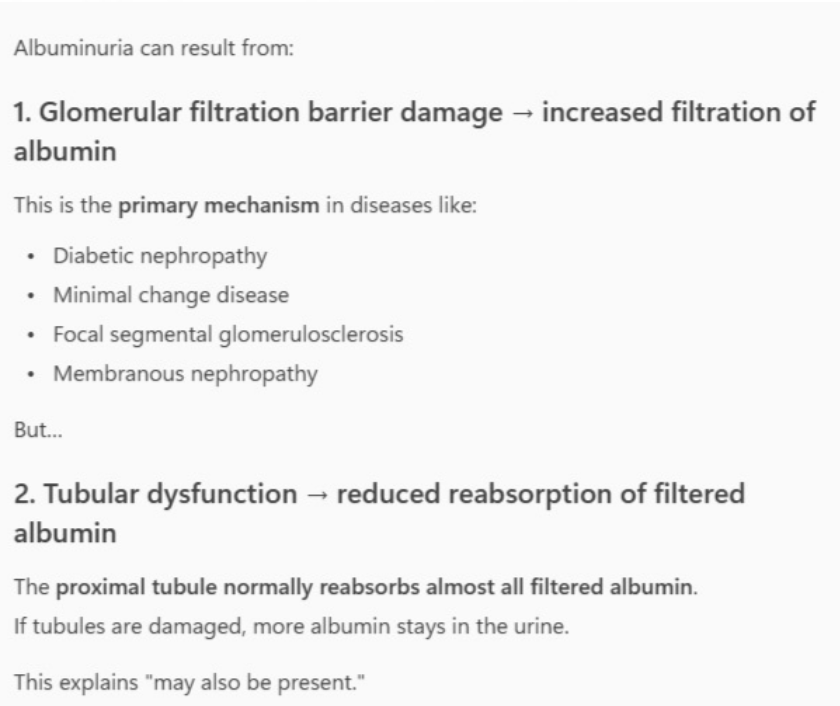
Most primary renal diseases with significant albuminuria are associated with structural changes in the glomeruli signifying that changes in glomerular function are the major contributor to the albuminuria but may also be present.
A - Functional changes at the nephron
B- Structural changes at the nephron
C- Distal tubule changes
D - Tubular dysfunction
E- Loop of Henle disfunction
D - Tubular dysfunction