Psych 257 - Lecture 4 : Clinical Assessment and Diagnosis
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
14 Terms
Clinical assessment vs. Diagnosis
Clinical assessment is the systematic evaluation and measurement of psychological, biological, and social factors in an individual presenting with a possible psychological disorder.
Diagnosis is the process of determining whether the particular problem affecting the individual meets the criteria for a psychological disorder, as set forth in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, text revision, or DSM-5-TR
Classification of Psychological Disorders + Pros and Cons
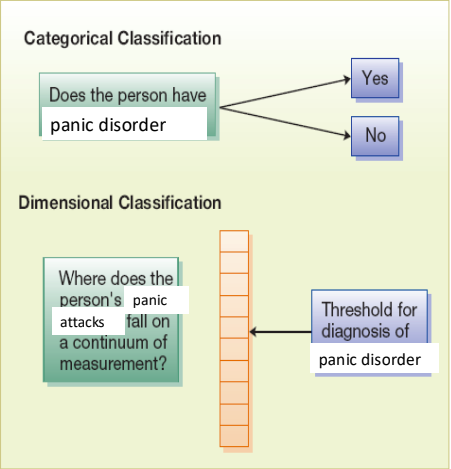
a) Categorical Approaches
b) Dimensional Approaches
Classification - Pros:
◦ Taxonomy : construct groups or categories and to assign objects or people to these categories on the basis of their shared attributes or relations
◦ Nomenclature : The naming system used to label and communicate about disorders clearly.
◦ Treatment and insurance : Classification helps determine appropriate care and ensures coverage for treatment.
◦ Research and grants : Provides standardized categories that make studying and funding mental disorders easier.
◦ Social/political : Supports awareness, advocacy, and policy development for mental health issues.
Classification - Cons:
Labeling: Assigning a diagnostic name that may define or limit how a person is seen.
Stereotyping: Assuming traits or behaviours about someone based on their label.
Stigma: A negative social judgment or discrimination toward people with mental illness.
Categorical Approaches - Pros and Cons
Pros:
Ease of communication (universal)
Vivid & succinct (conveys it quick)
Clinical decisions are often categorical (can access the treatment plans/programs) → can join treatment/ medicate
Easy research participant classification → easy to classify who to include/ exclude
Fits with medical model approach
(i.e., ease of administration, insurance coding, etc.)
Cons:
Unique pathological causes?
Shared case that leads to different outcomes
Heterogeneity issues
different manifestation but diff sympotms
Loss of important clinical information
People with 1 less symptoms as bad as no symptom, “it’s not bad enough”
Implications for prevalence rates
Hides or makes a problem if criteria changes
Boundary disputes
Co-occuring issues; cannot have them be put into multiple boxes
Not otherwise specified (lots of people diagnosed with this since they don’t fit)
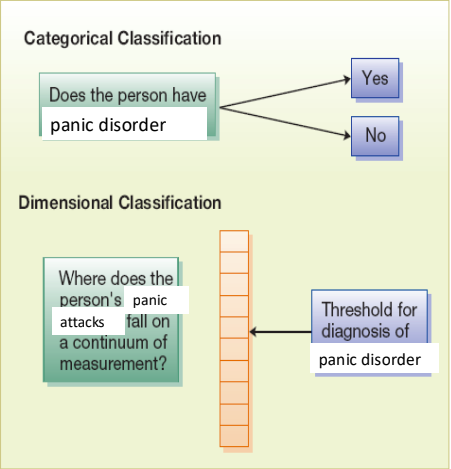
Dimensional Approach - Pros and Cons
Pros:
Diagnostic reliability & stability over time
Eliminate boundary disputes & comorbidity
Gather more patient information
May benefit therapy (e.g., less specialized - instead of things that only work for one thing)
Could be helpful for research
better for it to be on a continuum rather than binary
Cons:
Still requires cut-off points → mild, moderate, severe; still in box
Lack of agreement on dimensions (standardization)
◦ Which ones?
◦ How many?
Re-training clinicians, disrupting research
More time/effort/cost ?? - we want quick and easy labels
About the DSM
Prototypical approach - Essential characteristics and non-essential variations
Main classification system of adult and child mental illness
Also International Classification of Diseases (ICD)
Broad categories w/ specific disorders
Symptom descriptions
Differential diagnosis
Non-theoretical
Statistics
Professionals who can diagnose
Strengths and Criticism of DSM-5
Strengths
Best reflects our current knowledge of psychopathology
• User-friendly
• Not biased toward one theory
Criticism
Too many people that were “normal” the day before have disorders now
2 week framework - too short
DSM - Unresolved Issues Classifications
Appropriateness of medical model
◦ Surface phenomena?
◦ Individual experiences and social context?
Dimensions vs. categories
Validity and reliability of categories
◦ No natural boundaries
Why assess
Clinical treatment reasons
◦ Formulate diagnosis
◦ Understand individual
◦ Predict behaviour
◦ Plan and narrow treatment
◦ Evaluate treatment outcome
◦ Help client understand, feel less ashamed
Research reasons
Characteristics of Strong Assessment Tools
1. Reliability – measurement consistency (The degree to which a measurement is consistent)
Inter-rater (The degree of agreement between different observers or clinicians using the same tool); test-retest (The stability of results when the same test is given to the same person at different times.)
2. Validity – measurement accuracy (The degree to which a technique measures what it is designed to measure)
Concurrent validity: comparing the results of a new assessment measure with the results of others that are better established allows you to begin to determine the validity of the first measure.
Predictive validity is how well your assessment tells you what will happen in the future.
3. Standardization – measurement, implementation, scoring, interpretation (Application of certain standards to ensure consistency)
Assessment Tools
1. Physical Exams
2. Psychological Tests
3. Behavioural Assessment - direct observation to formally assess an individual’s thoughts, feelings, and behaviour in specific situations or contexts;
4. Psychophysiological Assessment
5. Neuropsychological Testing
6. Neuroimaging
7. Clinical Interviews (patient, family)
Clinical Interviews
• Face-to-face assessment
Unstructured - follow no systematic format
Structured
The Mental Status Exam
Semi-structured - made up of questions that have been carefully phrased and tested to elicit useful information in a consistent manner, so clinicians can be sure they have inquired about the most important aspects of particular disorders.
• Context relevant
• Gather detailed client information
Content
Process
The Mental Status Exam
Exam covers five categories:
appearance and behaviour
thought processes - fast, slow, continuity of speech
Evidence of delusions: delusions of persecution, ideas of reference, hallucinations
mood and affect - the predominant feeling state of the individual
refers to the feeling state that accompanies what we say at a given time; appropriate or inappropriate
intellectual functioning - vocab, memory, above or below average intelligence
sensorium - general awareness of our surroundings.
The ABCs of Observation
Antecedents - (what happened just before the behaviour)
Behaviour
Consequences - (what happened afterward)
Observational assessment
Observational assessment is usually focused on the here and now. Therefore, the clinician’s attention is usually focused on the immediate behaviour, its antecedents (what happened just before the behaviour), and its consequences (what happened afterward)
Formal observation involves identifying specific behaviours that are observable and measurable
informal observation spontaneous or unstructured observation where behavior is not measured systematically, but rather noted in a general or subjective way based on overall impressions.
Self Monitoring