Anatomy Lecture Block 3
1/236
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
237 Terms
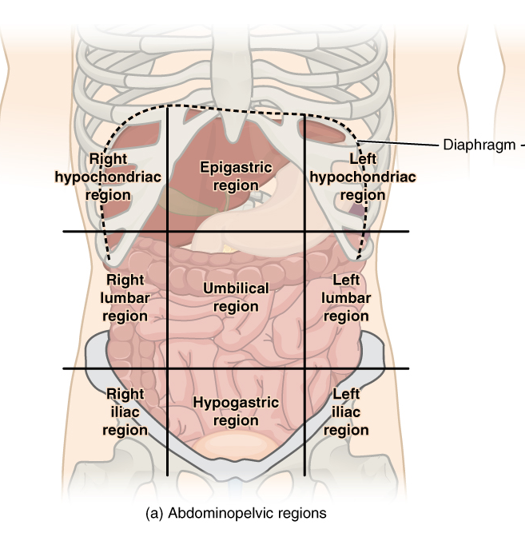
9 regions of the abdomen
right/left hypochondriac
right/left lumbar
right/left iliac
epigastric
umbilical
hypogastric
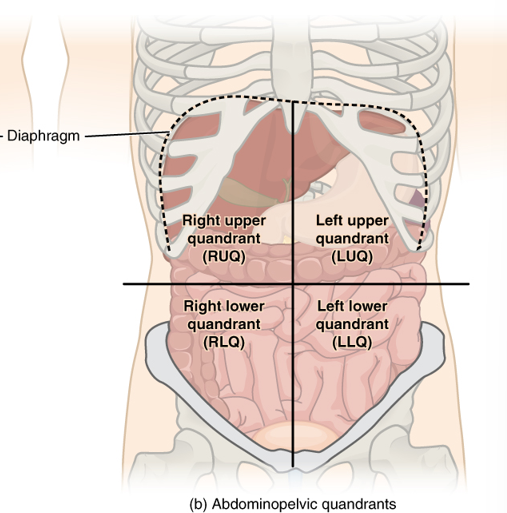
4 quadrants of the abdomen
right/left upper quandrant RUQ/LUQ
right/left lower quandrant RLQ/LLQ
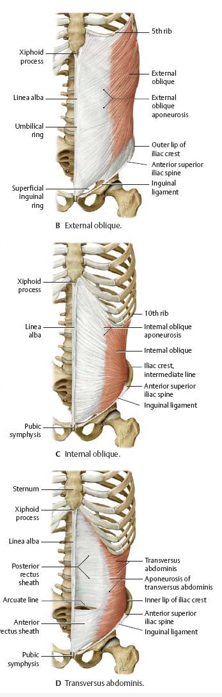
lateral group muscles and their innervation
external abdominal oblique
internal abdominal oblique
transverse abdominis
INNERVATED BY 6 LOWER INTERCOSTAL NERVES AND L1
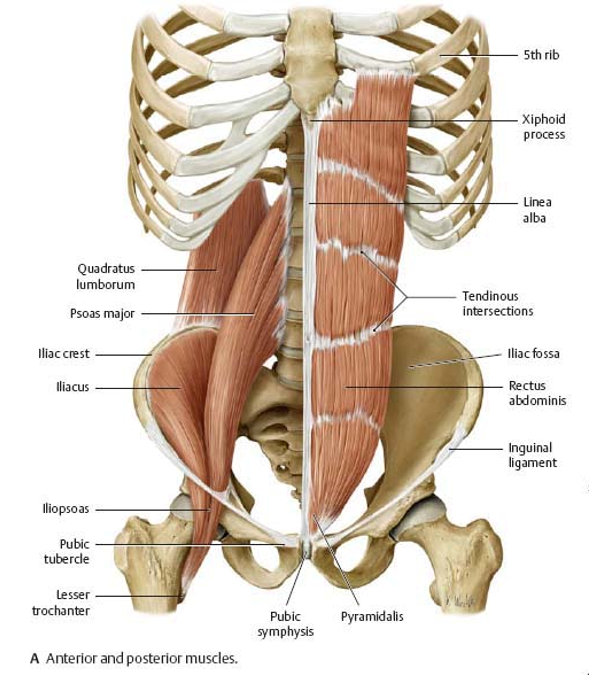
medial group muscles and their innervation
rectus abdominis
pyramidalis
INNERVATED BY 6 LOWER INTERCOSTAL NERVES AND L1
function of the lateral and medial group muscles
compress abdominal viscera
flex and rotate the trunk (via thoracic/flexion/extension via lumbar)
expiratory muscles
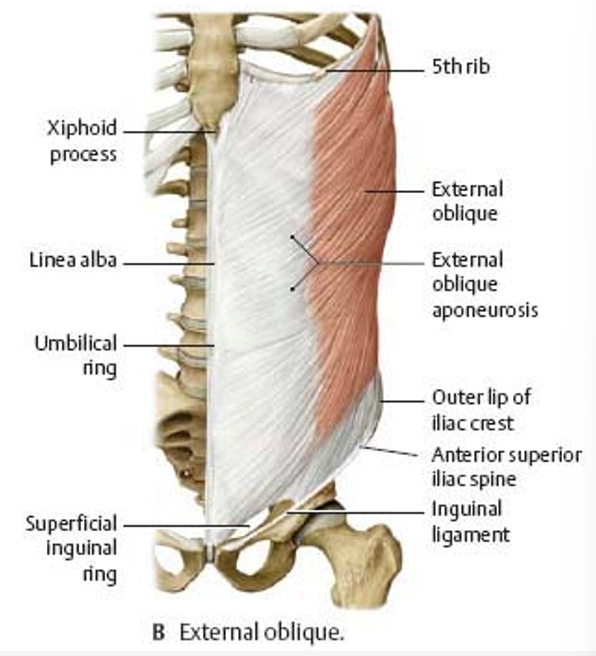
external abdominal oblique characteristics
lowest part of the aponeurosis
origin of the inguinal ligament
continuous w/ the inguinal ligament
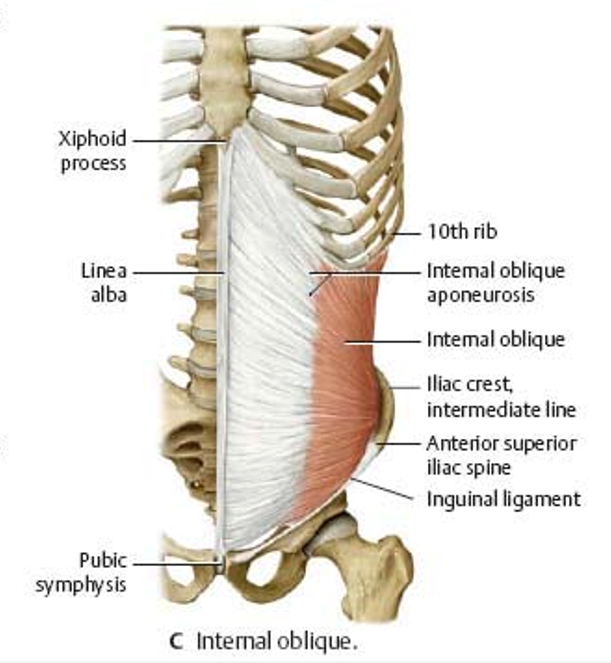
internal abdominal oblique
cranial part
middle part - aponeurosis helps make rectus sheath as 2 layers (anterior and posterior rectus abdominis)
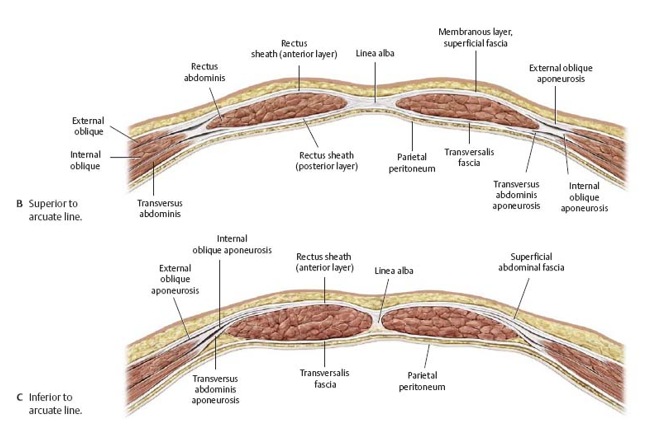
inferior layer terminated 5cm below navel (at arcuate line)
caudal part - continues in male into the spermatic cord as the cremaster muscle and its thin fibers reach around the round ligament in females
innervation of cremaster muscle
genital branch of genitofemoral nerve
cremastic reflexes
afferent limb (sensory input)- femoral branch of genitofemoral
efferent limb (motor output)- genital branch of genitofemoral
cremsasteric reflex origin, innervation, and clinical significance
origin: caudal part of internal abdominal oblique mucsle
wraps around spermatic cord in males
consists of thin fibers that make up round ligament of uterus in females
innervation: genital branch of genitofemoral nerve(sensory and motor)
clinical significance:
twisted testes/mass in testes, we can palpate the upper thigh to see if we have contraction of the cremaster muscle (if we do, then both sensory/motor work properly)
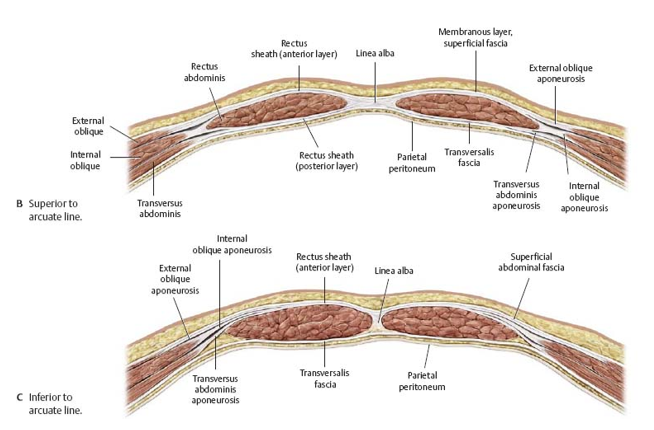
rectus sheath
aponeurosis of lateral group adbominal muscles that surround the rectus abdominis anteriorly and posteriorly
location of the rectus sheath:
anterior
middle …encircles
internal…posteriorly beneath
location of the rectus sheath:
aponeurosis of external oblique is on the __ side of the rectus abdominis
aponeurosis of internal oblique in the ___ splits into 2 layers and ___ the rectus abdominis (one part is posterior and the other, anterior)
transverse abdominal muscle is ___ and continues ___
the transversalis facia is ___ the transverse abdominal muscle
what is the origin of the inguinal ligament
the lowest (inferior part) aponeurosis of the external oblique muscle
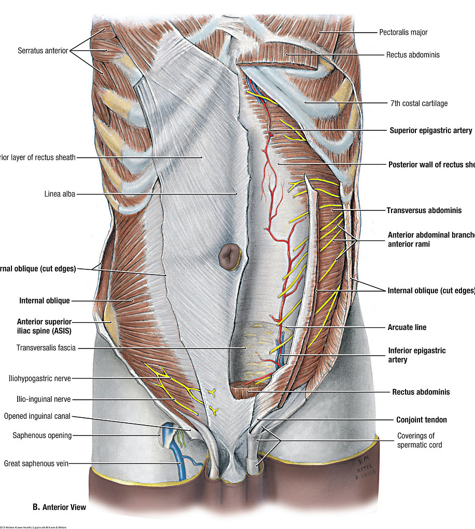
contents of the rectus sheath
rectus abdominal muscle
inferior/superior epigastric vessels
5 lower intercostal nerves (including subcostal nerve)
location of the inguinal canal and its deep and superficial rings
parallel to the inguinal ligament and its opening
deep inguinal ring - internal opening and a gap in the fascia transversalis
superficial inguinal ring - gap in aponeurosis of the external abdominal oblique muscle
contents of the inguinal canal in men and females
male - spermatic cord
female - round ligament of the uterus and lymphatics
descent of the testis:
spermatic cord
scrotum … inguinal canal
processus vaginalis … scrotum … tunica vaginalis
descent of the testis:
testis are connected to the ______
testis descend from the abdominal cavity into the ___ via the _____ during intrauterine life
b4 descension of testis, part of the _______ (peritneum abdominal lining) travels through the canal to line the developing ___ and create space for the testis to sit and follow, ultimately becoming the ___ around the testis
cryptorchidism clinical significance and treatment
when the testis fails to descend into scrotum
immediate fix eneded bc pendulous testes are temperature sensitive (5-7 than rest of the body); if stuck inside the body → cant become cool
treatment:
normally developed testis - pass them through the inguinal canal into the scrotum
underdeveloped testis - get rid of it
hydrocele of the cord
proccesus vaginalis doesnt close after descent of testis → fluid buildup around spermatic cord
treatment - remove fluid and suture
contents of the spermatic cord
ductus (vas) defrens
testicular artery
ductus deferens artery cremaster artery
pampiniform plexus
autonomic nerve fibers
genital branch of the genitofemoral nerve
lymphatics
cremaster muscle
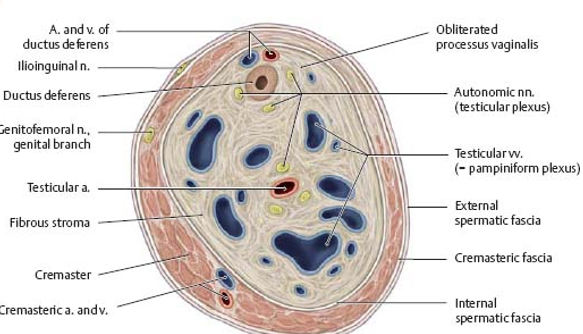
pampiniform plexus
net-like blood vessels in the fibrous stroma that surround the testicular arteries
blood flow of testis:
blood flow of testis:
artery goes into the testis and carries warm (98.6 farenheit) blood from the abdomen
testis venous blood is cool and travels back to the heart
as blood comes across each other, warm blood coold down b4 it enters the testis via counter current exchange
ONE ARTERY AND A VENOUS NETWORK AROUND IT
cremaster muscle
Helps cool/heat the testes via contraction/relxation ultimatley manipulating blood flow through pampiniform plexus
Relaxed -> testes falls further from body
Contracted -> testes pulled closer to the body
direct/indirect inguinal hernias
both occur superior to the inguinal ligament
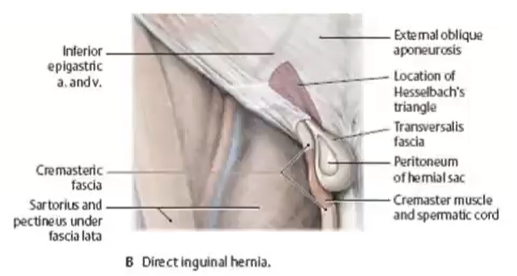
direct inguinal hernia
abdominal wall split in the Hesselbrach’s triangle → instestine loop comes out
medial to epigastric vessels
doesnt pass through the inguinal canal (parallels the spermatic cord)
smaller in size
low risk of strangulation/infarction (softer/malleable)
acquired
happens in Hesselbrach’s triangle (superficial opening location)
risk factors and treatment for direct inguinal hernias
middle age men (40+ yrs old)
smaller in size
treatment:
doesn’t always require surgery
binding/brace then bedrest
laparoscopic cord and suture
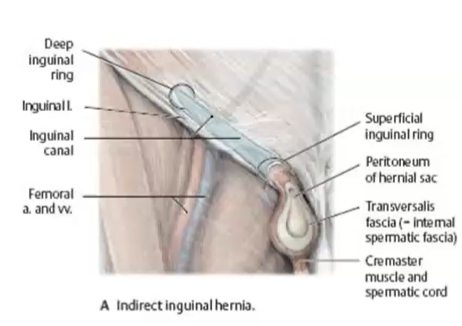
indirect inguinal hernias
happens underneath the fascia of spermatic cord → pushed length of spermatic cord → compromised blood flow
lateral to epigastric vessels
passes through inguinal canal (inside the spermatic cord)
high risk of strangulation/infarction
congenital and also can be acquired
risk factors and treatment for indirect inguinal hernias
younger ppl
bigger in size
treatment: requires surgery to pull loop of intestine back out into the abdominal cavity
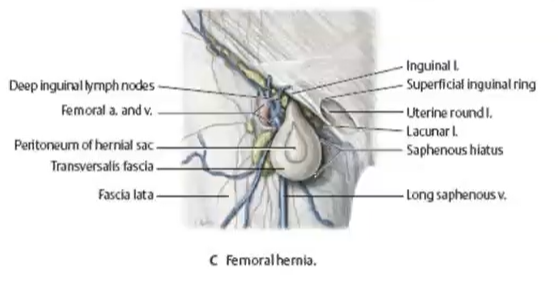
femoral hernias
inferior to the inguinal ligament
more common in females
very painful
peritoneum
serous membrane lining the abdominal and pelvic cavities
has greater and lesser sac
greater sac
main part of the peritoneal cavity
lesser sac (omental bursa)
diverticulum of the peritoneal cavity
on the left side
posterior to the stomach
mesentary
double layer of the visceral peritoneum that has vessels, nerves, and fat
connects intestines to the posterior abdominal wall
mesenteric border
fixed, more vascular
anti-messenteric border
free border, less vascular
where surgery is done
innervation of the peritoneum
somatic nerves - parietal layer
autonomic nerves - visceral layer (including mesentary)
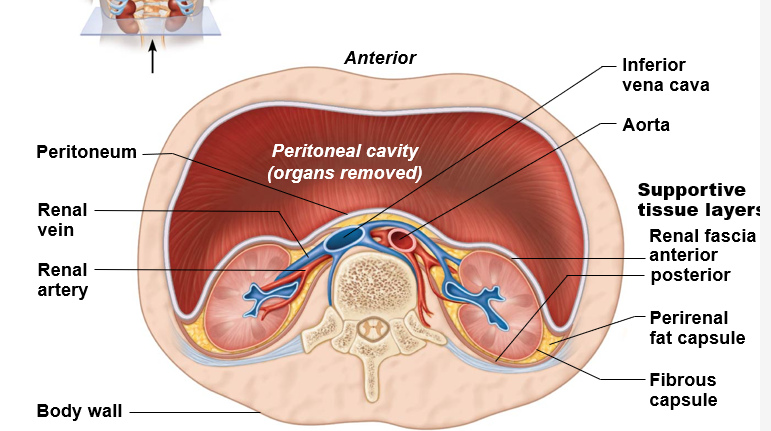
what are retroperitoneal organs?
organs that are NOT covered by visceral peritoneum and are BEHIND the peritoneal cavity
retroperitoneal organs
kidneys
suprarenal glands
uterine cervix
descending, horizontal, and ascending duodenum
pancreas
ascending & descending colon
upper 2/3 of rectum
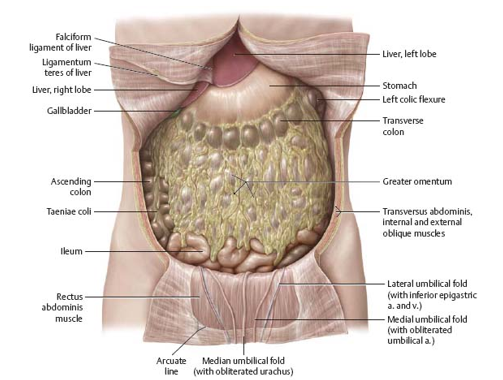
what are intraperitoneal organs
organs that has a mesentery and are covered by the peritoneum
intraperitoneal organs
stomach
small intestine (jejunum, ileum, some superior duodenum)
spleen
liver
gallbladder
cecum w/ vermiform appendix (varies)
large intestine (transverse and sigmoid colons)
peritoneum pathway:
anterior
inferior
flaciform ligament
anterior & inferior
anterior
peritoneum pathway:
it lines the ____ abdominal wall
reflects upward to cover ____ surface of diaphragm
reflects onto the liver → making the _______
covers the ___ and ____ inferior surfaces of the liver
continues downwards as the ___ layer of the lesser omentum (liver →stomach)
peritoneum over the stomach:
anterior
greater omentum
peritoneum over the stomach:
covers the ____ surface of the stomach
descends as the ______
lesser sac
behind the stomach
superior and inferior recess (pocket)
has an opening, Epiploic foramen, which is beneath the portal triad
epiploic foramen (foramen of winslow) and its clinical signficance
opening to the lesser sac
beneath the portal triad
clinical significance: increase in abdominal fat/pressure → causes intestines to be pushed → upwards displacement of small intestines → small intestines loop pushed through the epiploic foramen and into the lesser sac → internal hernia and strangulation
epiploic foramen and surgical importance
srugery done from greater sac
right next to the porta hepatis
structures reachable through the epiploic foramen
posterior liver surface
cystic artery of gallbladder via lesser sac
portal triad which is anterior to the foramen
importance of mesentary
prevents adhesion of visceral and parietal peritoneum
good amount of mobility → moves by peristaltic movement of viscera
has fat, lymphocytes, and immune cells to protect against infection/inflammation in abdominal cavity (abdominal policeman)
protects abdominal organs against injury and acts as insulator against loss of body heat
anterio, posteriorm superior, and inferior bounderies of epiploic foramen
anterior - porta hepatis (portal triad): hepatic artery, common bile duct, and portal vein
posterior - IVC and right crus of diaphragm
superior - caudate lobe of liver
inferior - first part of duodenum
abdominal policeman
immune cells that protect against infection/inflammatory conditions in abdominal cavity by wrapping around , separating the inflamed/healing parts and releasing inflammatory mediators to get helpuful immune cells
move towards inflamed/infected area (o.e Appendicitis)
why its important to move after abdominal surgery → otherwise adhesions of greater momentum → tears
collects … localized
because of the arrangement of the peritoneum, fluid in the abdominal cavity ___ and becomes ___ in certain regions
subphrenic spaces
between the diaphragm and the liver on both sides of the falsiform ligament
inhaled anesthetic → increased serous fluid production that sits in subphrenic space → diaphragm irritation → respiratory problems (another reason for the importance of movement post-surgery)
paracolic gutters
besides the ascending/descending colon
right subhepatic space (pouch of morison)
between the liver and the right kidney
lowest part of the abdominal cavity when lying flat (supine position)
another site of fluid accumulation postoperative from lack of movement
left subhepatic space
equal to lesser sac
fluid can become trapped behind the stomach
right and left infracolic spaces
below transverse mesocolon
divided by the mesentery of the small intestine
fluid can track into pelvis
rectouterine (douglas) pouch
possible fluid accumulation site w/ pelvic inflammatory disease
in females
pelvic cavity
rectovesical pouch
fluid accumlation site in the pelvic cavity of males
peritonitis
inflammation along w/ pain of the peritoneum a4 an abdominal injury → can cause fluid from parietal peritneum to go into abdomen
i.e stab wound or perforated appendicitis (fecal material/ e coli spills out into abdonimal cavity)
can be acquired secondarily
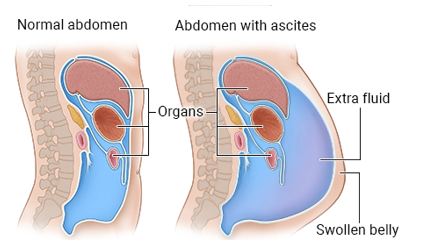
ascites
abnormal accumlation of fluid in the abdominal cavity
often seen in liver cirrhosis (end-stage liver cirrhosis) which compromises blood flow in liver
more common
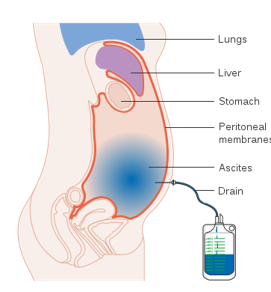
paracentesis
puncturing the peritoneal cavity to get rid of excess buildup fluid
done via a catheter and massage done a4 to keep fluid from getting trapped in the compartments
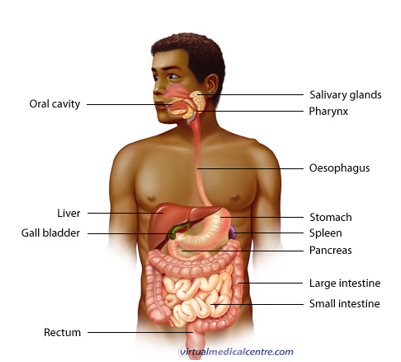
anatomy of digestion tract
made of the esophagus, stomach, and intestine which come from the primordial foregut, midgut, and hindgut
foregut
esophagus
stomach to the 2nd part of duodenum
liver
billiary system
gall bladder
pancreas
midgut
lower half of 2nd part of duodenum
jejunum
ileum
colom (cecum, ascending and right 2/3 of transverse colon)
hindgut
left 1/3 of transverse colon
descending colon
sigmoid colon
rectum
upper part of anal canal
blood supply of foregut, midgut, and hindgut
foregut - celiac trunk
midgut - superior mesenteric artery
hindgut - inferior mesenteric artery
parasympathetic innervation of forgut and midgut (rest & digest)
vagus nerve (CN X) - esophagus to 2/3 right of transverse colon
pelvic sphlanchnic nerves (S2-S4) - 1/3 left of transverse colon down to the anal canal
sympathetic innervation of the hindgut (flight or fight)
spinal segments (T5-L2) - from the lower esophagus to anus
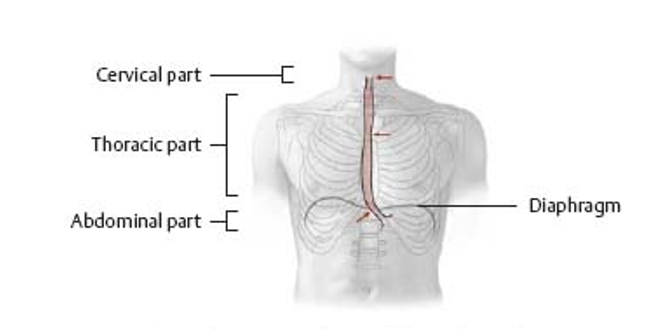
esophagus characteristics
25-30cm long
starts at C6 vertebra (cricoid cartilage)
ends below the diaphragm at T10-T12
enters the stomach at the cardia
function and innervation (sympathetic/parasympathetic) of the esophagus
function: conveys bolus of food to the stomach
innervation:
sympathetic - T5-L2 spinal segments
parasympathetic - vagus nerve
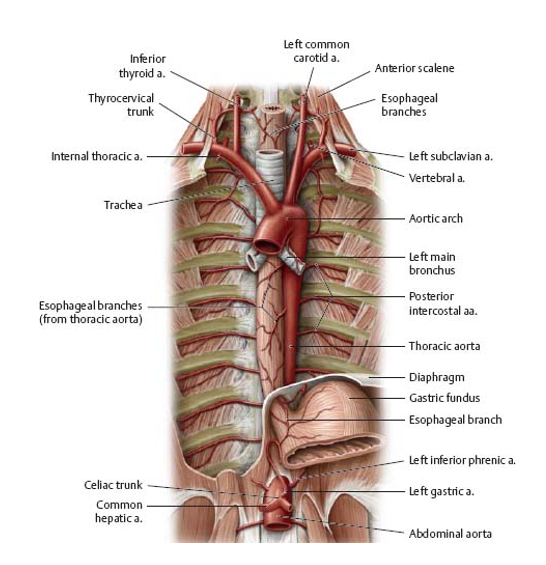
blood supply of the upper, middle, and lower parts of the esophagus
upper(cervical): inferior thyroid artery
middle (thoracic): 4-5 arteries from the thoracic aorta and bronchial arteries
lower/adominal portion: left gastric artery (from celiac artery) and inferior phrenic artery (from abdominal aorta)
venous drainage of the upper, middle, and lower parts of the esophagus
upper: inferior thyroid vein → brachiocephalic → SVC (SYSTEMIC CIRCULATION)
middle: azygous vein → hemiazygos vein → SVC (SYSTEMIC CIRCULATION)
lower: left gastric vein → portal vein (PORTAL CIRCULATION)
lower esophageal connection plays role in esophageal varices in liver cirrhosis
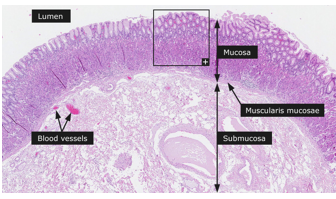
layers of the esophagus innermost → outermost
mucosa
submucosa
tunica muscularis/muscularis externa
adventitia/serosa
mucosa of the alimentary canal/esophagus
stratified non-keratinized squamous epithelium that transitions to simple columnar in cardia)
muscularis mucosa - thin layer of smooth muscle
lamina propria - connective tissue
submucosa of the alimentary canal/esophagus
connective tissue that has blood vessels, lymphatics, and nerve fibers
muscularis externa/ tunica muscularis of alimentary canal/esophagus
2 layers of smooth muscle
inner circular muscular layer that squeezes the tube
outer longitudinal muscular layer that shorts it
serosa/adventitia of alimentary canal/esophagus
connective tissue that binds strcture to surroudning structures
hiatal hernias, its types, and treatment
hernias where part of the stomach herniates into the mediastinum through the esophageal hiatus of the diaphragm → pain w/ chest pains and cardiac ichemia
types:
sliding hiatal hernia
para-esophageal hiatal hernia
treatment: both fixed via surgery (fundoplication) to reinforce LES barrier
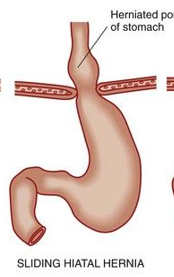
sliding hiatal hernia
when abdominal part of esophagus, cardia and fundus slide up through the esophageal hiatus → pressure on LES → LES pushes open → regurgitation and heart burn

para-esophageal hiatal hernia
part of the fundus and peritoneum passes through the esophageal hiatus into thoracic cavity
no regurgitation
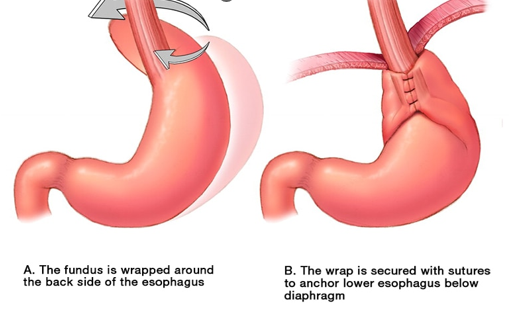
fundoplication
operation to correct gastroesophageal reflux, reinforce barrier to reflux LES
upper portion of stomach (fundus) wrapped (plicated) around lower portion of esophagus and anchored securely below the diaphragm
radiofrequency treatment
radiofrequency energy causes tiny burns at G-E junction that heal and form scar tissues which tightens the weaken valve or LES
endoscope supplied by electrodes are used

esophageal atresia
distal end of esophagus is closed
esophagus is supposed to be continuous
we just need to close the tubes together
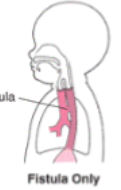
tracheoesophageal fistula
abnormal connection between the esophagus and traches w/ epithelial cells
milk from nerborn esophagus goes into respiratory track → severe problems
we need to sever the connection
malignancy
frequency at transition between epithelia types
esophageal cancers
low in north america
higher in iran and china bc of irritation of mucosa from hot tea and opium use
diverticulum
where all 3 wall layers (mucosa, submucosa, and tunica muscularis) protrude to form little pouches
most common in large intestines
zenker’s diverticulum
upper esophagus, dysphagia (difficulty swallowing), and halitosis (bad breath), regurgitation → food gets trapped
complications - ulceration, bleeding, and inflammation
treatment - surgery in the esophagus, diet changes for large intestine
achalasia (cardiospasm)
neuromotor disorder of the LES that causes retrosternal pain
LES cant open/relax to let food pass into stomach bc of weakness of secretomotor function/peristaltic movement→ food cant be swallowed into esophagus → increased LES pressure
loss of ganglion cells in myenteric plexus (analogus to Hirschsprung’s disease)
dysphagia for both solids and liquids
dilated proximal esophagus
aperistalsis
risk factors and treatment of achalasia (cardiospasm)
risk factors: congenital (not all fibers show up in submucosa) or developmental (from trauma/stroke)
treatment:
drinking cold/warm thing can stimulate LES to open up
often need mechanical assistance at the hospital
if patient cant swallow → feeding tube via stomach
columnar … metaplasia
barret’s esophagus is the damage to ___ cell metaplasia of the ___ epithelium
cause and effect of barret’s esophagus
result of acid injury/chemical burn
LES doesnt close proplerly → gastric secretion regigurgitation (hydrochloric acid)
GI tracts’ innnvervation system
GI tract has built-in nervous system w/ two plexuses called the submucosal plexus of meissner and myenteric plexus of auerbach
submucosal plexus of Meissner:
secretomotor function of mucus for lubrication and facilitation of molecule movement (feces and foods) and absorption
myenteric plexus Auerbach:
muscle fibers that cause peristaltic movement of smooth muscle
a branch talks to each muscler fiber
autonomic innervation of digestive tract
parasympathetic - stimulates/increases
via vagus CN X and pelvic splanchnics S2-S4
sympathetic - inhibits/decreases
via T5-L2
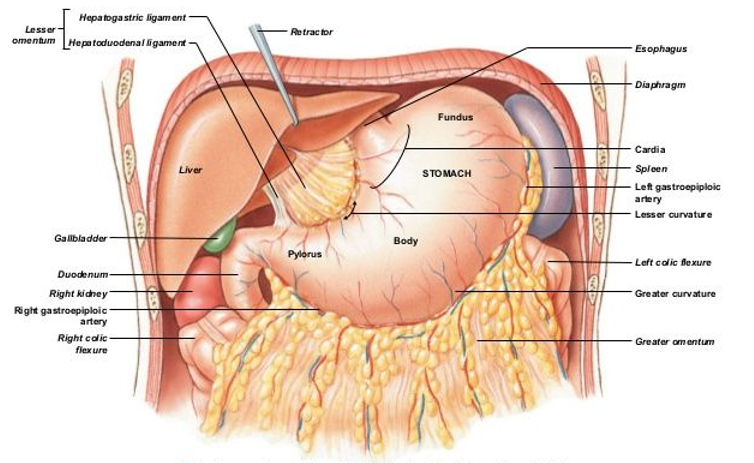
stomach
most dilated part of alimentary tract in upper left quadrant of the abdomen
between the esophagus and lesser intestine
functions as food reservoir and involved in enzymatic digestion
stomach charasterics
has longitudinal smooth layer and oblique smooth muscle layer (which helps w/ mechanical digestion/physically breaks things up)
has rugae which helps expand surface area in the stomach other than in lesser curvature
has cells that specialize in secreting hydochloric acid and enzymes that weaken bonds within protein molecules for further digestion in small intestine
hypertrophic pylroic stenosis
progressive hypertrophy of circular muscles in pyloric sphincter → narrow pyloric lumen → obstruction of food passage
seen in male infants (first child) and they have:
nonbilious vomiting after feeding
small olive sized knot in right costal margin seen via palpation
what does nonbilious vomiting tell us?
it tells us we cant move smth out of stomach and into the duodenum or that bile cant move from the duodenum and upwards → ULTIMATELY THERES A BLOCKAGE
longitudinal pyloromyotomy
hypertrophic pyloric stenosis treatment where we take the longitudinal smooth muscle out of the pyloric sphincter and leave the mucosa intact