UCF Anatomy Block 4 lecture (good 0ne)
1/194
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
195 Terms
Fracture of the surgical neck of the humerus
Injury to axillary nerve.
Fracture of the middle of the shaft of the humerus
may cause injury to the radial nerve = wrist drop
Fracture of the distal end of the humerus
Injury to the Median nerve.
Fracture of the medial epicondyle of the humerus
Injury to the ulnar nerve.
Radial Nerve
Travels posteriorly and innervates the muscles of the arm and forearm.
Median Nerve innervation
all but 2 muscles of the forearm
Ulnar Nerve
Innervates Flexor Carpi Ulnaris and Flexor Digitorum Profundus (hybrid, innervated by the median and ulnar nerve).
Fracture of different areas of the humerus
Depending on the area, it causes damage to different nerves, including the nerve functionality, and the muscles that the nerves innervate.
The Proximal Epiphysis
In pre-pubertal individuals, both proximal and distal pivotal plates continue to add cartilage, which ossifies during growth once the individual undergoes puberty. Once the individual goes through puberty, steroids trigger the closure by preventing any more cartilage from being put into the plates. Once cartilage is replaced with bone cells, the closure and fusion are complete. Their name changes from plates to epithelial cells.
Traumatic Separation of the Proximal Epiphysis
The proximal end of the humerus is held in place by tendons, joint cavities, and ligaments. Separation can occur, and when it happens in individuals under 18-20 years, it can cause premature closure of the epiphyseal plates, causing abnormal growth and shoulder dislocation.
Joints of the shoulders
1. Acromioclavicular joint.
2. Glenohumeral joint.
3. Scapulothoracic joint (formed by region of the scapula with ribs 3 and 4, 3 mainly).
4. Sternoclavicular joint
Vein utilized for venipuncture
Median cubital vein because it is easy to see, by putting something like an elastic band in order to restrict blood flow, blood backs up into this vein, it becomes engorged and it can be palpated easily, meaning easy access.
Anterior Compartment of the Forearm (superficial group)
1. Pronator teres
2. Flexor Carpi Radialis
3. Palmaris Longus
4. Flexor Carpi Ulnaris
Anterior Compartment of the Forearm (intermediate group)
Flexor Digitorum Superficialis.
Anterior Compartment of the Forearm (deep group)
1. Flexor Digitorum Profundis
2. Flexor Pollicis Longus.
3. Pronator Quadratus.
Colles' Fracture
Fracture of the radial styloid process; posterior displacement forces the process into the shaft. It may be accompanied by an avulsion of the ulnar styloid process due to also breaking the ulnar styloid process. When both processes break.
The radius is much larger when compared to the ulna in terms of the distal end. When people fall with their arm extended.
Treatment: requires surgery to retrieve the radial styloid process that was misplaced in the shaft, and then it is reattached to its original place.
The head of the of the radius is
Proximal
3 multiple choice options
The head of the ulna is
Distal
3 multiple choice options
Brachial Plexus Nerves
1. Musculocutaneous Nerve.
2. Axillary Nerve.
3. Median Nerve.
4. Radial Nerve.
5. Ulnar Nerve.
Musculocutaneous nerve roots
Roots C5-C7; flexion at both the shoulder and elbow.
Median Nerve roots
Roots C6-T1; movement in the forearm and the parts of the hand.
Axillary Nerve roots
Roots C5 and C6; helps with shoulder rotation and enables the arm abduction.
Radial Nerve roots
Roots C5-T1; movement in the arm, elbow, forearm, and hands.
Ulnar nerve roots
Roots C8-T1; fine motor control of the fingers.
Pronator Teres Origin
The medial epicondyle of the humerus and the coronoid process of the ulnar head.
Pronator Teres Insertion
Lateral radius (distal to supinator insertion).
Pronator Teres Innervation
Median nerve. (C6-C7).
Flexor Carpi Radialis Origin
Medial epicondyle of the humerus
Flexor Carpi Radialis Insertion
Base of 2nd and 3rd metacarpal
Flexor Carpi Radialis Innervation
Median nerve (C6, C7)
Palmar Longus Origin
Medial epicondyle of humerus
Palmar Longus Insertion
Palmar aponeurosis
Palmar Longus Innervation
Median nerve (C7, C8)
Flexor Carpi Ulnaris Origin
Medial epicondyle of humerus and olecranon process of ulna.
Flexor Carpi Ulnaris Insertion
Pisiform, hook of hamate, base of 5th metacarpal
Flexor Carpi Ulnaris Innervation
Ulnar nerve (C7-T1)
Flexor Digitorum Superficialis Origin
Medial epicondyle of humerus and coronoid process of ulnar head.
Flexor Digitorum Superficialis Insertion
Sides of the middle phalanges of 2nd and 5th digits.
Flexor Digitorum Superficialis Innervation
Median nerve (C8, T1).
flexor digitorum profundis origin
Ulna two third of flexor muscle and interosseous membrane
flexor digitorum profundis insertion
Distal phalanges 2nd to 5th digits (palmar region)
flexor digitorum profundis innervation
Median and Ulnar nerve (C8, T1)
Flexor pollicis longus origin
Radius (midanterior surface) and adjacent interosseous membrane.
Flexus Pollicis Longus Insertion
Distal phalanx of thumb (palmar surface)
Flexus Pollicis Longus Innervation
Median nerve (C7,C8)
Pronator Quadratus Origin
Distal quarter of ulna (anterior surface)
Pronator Quadratus Insertion
Distal quarter of radius (anterior surface).
Pronator Quadratus Innervation
Median nerve (C7,C8).
Lymph Nodes Groups
Pectoral, Lateral, Central, Apical, and Posterior
Lymph Nodes Drainage
Subclavian lymphatic trunk to right lymphatic duct to right venous angle. 75% of breast's lymphatics drain here.
Lymphangitis
Swelling of the upper limb, lymphatic fluid building up in that area, is debilitating and compromises quality of life because individuals are not capable of using their upper limb.
Usually, after a mastectomy, the removal of the breast compromises lymphatic flow due to not having a way of emptying the lymphatic fluids of the upper limb.
Mastectomy was done due to Breast Cancer, transporting metastasis to the axillary lymph node.
Wing Scapula muscles involved
Due to a lack or loss of innervation. Three muscles involved: rhomboid minor, rhomboid major (both innervated by the dorsal scapular nerve), and serratus anterior (innervated by the long thoracic nerve).
How to determine which muscles are compromised in the Wing Scapula?
-Patient can lift their arms: rhomboids issue.
- Patient not capable of lifting their arms: serratus anterior issue
Two ways Wing Scapula can happen:
-Radial Mastectomy: a third of the breast tissue is situated anterior to the serratus anterior, removal of tissue leads to damaging the long thoracic nerve, which leads to Wing Scapula.
- Traumatic Injury: tearing/ rupture of rhomboid muscles, which can also be due to overuse.
Posterior Compartment Muscles of the Forearm
1. Extensor digitorum. (superficial)
2. Extensor Digiti Minimi.(superficial)
3. Extensor Carpi Ulnaris. (superficial)
4.Supinator (deep).
5. Abductor Pollicis Longus (deep).
6. Extensor Pollicis Brevis (deep)
7. Extensor Pollicis Longus.(deep)
8. Extensor Indicis (deep).
Extensor Digitorum Origin
Lateral epicondyle of humerus (common head).
Extensor Digitorum Insertion
Dorsal digital expansion of 2nd and 5th digits.
Extensor Digitorum Innervation
Radial Nerve (C7, C8).
Extensor Digiti Minimi Origin
lateral epicondyle of humerus (common head)
Extensor Digit Minimi Insertion
dorsal digital expansion of 5th digit
Extensor Digiti Minimi Innervation
Radial nerve (C7,C8).
Extensor Carpi Ulnaris Origin
Lateral epicondyle of humerus (common head); and dorsal surface (ulnar head).
Extensor Carpi Ulnaris Insertion
Base of 5th metacarpal
Extensor Carpi Ulnaris Innervation
Radial nerve (C7, C8).
Supinator Origin
Olecranon, lateral epicondyle of humerus, radial collateral ligament, and annular ligament of the radius.
Supinator Insertion
Radius (between radial tuberosity and insertion of pronator teres).
Supinator Innervation
Radial nerve (C6,C7)
Abductor Pollicis Longus Origin
Radius and Ulna (dorsal surfaces, interosseous membrane).
Abductor Pollicis Longus Insertion
Base of 1st metacarpal
Abductor Pollicis Longus Innervation
Radial nerve (C7,C8)
Extensor Pollicis Brevis Origin
Radius (posterior surface) and interosseous membrane.
Extensor Pollicis Brevis Insertion
Base of proximal phalanx thumb.
Extensor Pollicis Brevis Innervation
Radial Nerve (C7,C8)
Extensor Pollicis Longus Origin
Ulna (posterior surface) and interosseous membrane.
Extensor Pollicis Longus Insertion
Base of distal phalanx of thumb.
Extensor Pollicis Longus Innervation
Radial Nerve (C7,C8)
Extensor indicis Origin
Ulna (posterior surface) and interosseous membrane.
Extensor Indicis Insertion
Posterior digital extension of 2nd digit
Extensor Indicis Innervation
Radial Nerve (C7, C8)
Radial Group Muscles
1. Brachioradialis.
2. Extensor Carpi Radialis Longus.
3. Extensor Carpi Radialis Brevis..
Brachioradialis Origin
Distal humerus
Brachioradialis Insertion
Radial Styloid Process
Brachioradialis Innervation
Radial nerve.
Extensor Carpi Radialis Longus Origin
Lateral supracondylar ridge of distal humerus
Extensor Carpi Radialis Longus Insertion
2nd metacarpal base.
Extensor Carpi Radialis Longus Innervation
Radial nerve.
Extensor Carpi Radialis Brevis Origin
Lateral epicondyle of humerus
Extensor Carpi Radialis Brevis Insertion
3rd metacarpal base.
Extensor Carpi Radialis Brevis Innervation
Radial nerve.
Brachial Plexus Neuropraxia (stretch)
-Roots compression usually by rotation of the head; commonly seen in older individuals.
-Nerve traction is a result of a downward pull; common among adolescents and young adults.
-Both characterized as "burners" or "stringers" depending on the sensation felt with each injury.
Brachial Plexus Rupture: stretch and rupture/partial tear.
- A forceful stretch resulting in the partial or complete tear of the nerve.
-Associated with muscle weakness and pain; severity depends on location and extent of injury.
-Often requires surgery to repair. If not repare, the patient can develop brachial plexus neuroma.
Brachial Plexus Neuroma
- Commonly occurs when a nerve is cut during surgery.
- Scar tissue forms a painful knot on the nerve, preventing it from healing itself in the actual attempt of healing itself.
-The scar tissue formation triggers sensory innervation, causing pain.
- Surgery is often required to remove scar tissue. Removal of neuroma.
Brachial Plexus Avulsion: most severe of all
-Nerve root completely separated from spinal cord (inside vertebral foramen).
-Common injury during childbirth (2/1000 births), among athletes, rock climbers, and blunt trauma.
-When an obstetrician is not experienced enough and tries to pull the arm of the baby as leverage, the shoulder is the most challenging part to get out.
-Two types depending on which nerves are involved: Upper Brachial Plexus and Lower Brachial Plexus
-Treatment depends on severity.
Upper Brachial Plexus (C5-C6)
- Most common type of avulsion.
-Erb- Duchenne paralysis.
Upper Brachial Plexus (C5-C6) Signs
-Numbness and loss of motion around the shoulder, inability to flex elbow.
-Deltoid and supraspinatus are paralyzed (no arm abduction).
-Infraspinatus paralysis leads to medial rotation of the arm.
-Biceps and Brachialis are also paralyzed, no elbow flexion.
-Loss of biceps and supinator, weak supination.
-Adductors of the shoulder are mildly affected (pectoralis major and latissimus dorsi).
Lower Brachial Plexus (C8-T1)
-Not as common as upper plexus injuries.
-Klumpke's paralysis.
Lower Brachial Plexus sign
-Loss of movement and/or sensation of the wrist and hand.
-Paralysis of the intrinsic muscle of the hand (small muscles) compromises finger movement.
-Atrophic paralysis of the forearm and small muscles of the hand (claw hand).
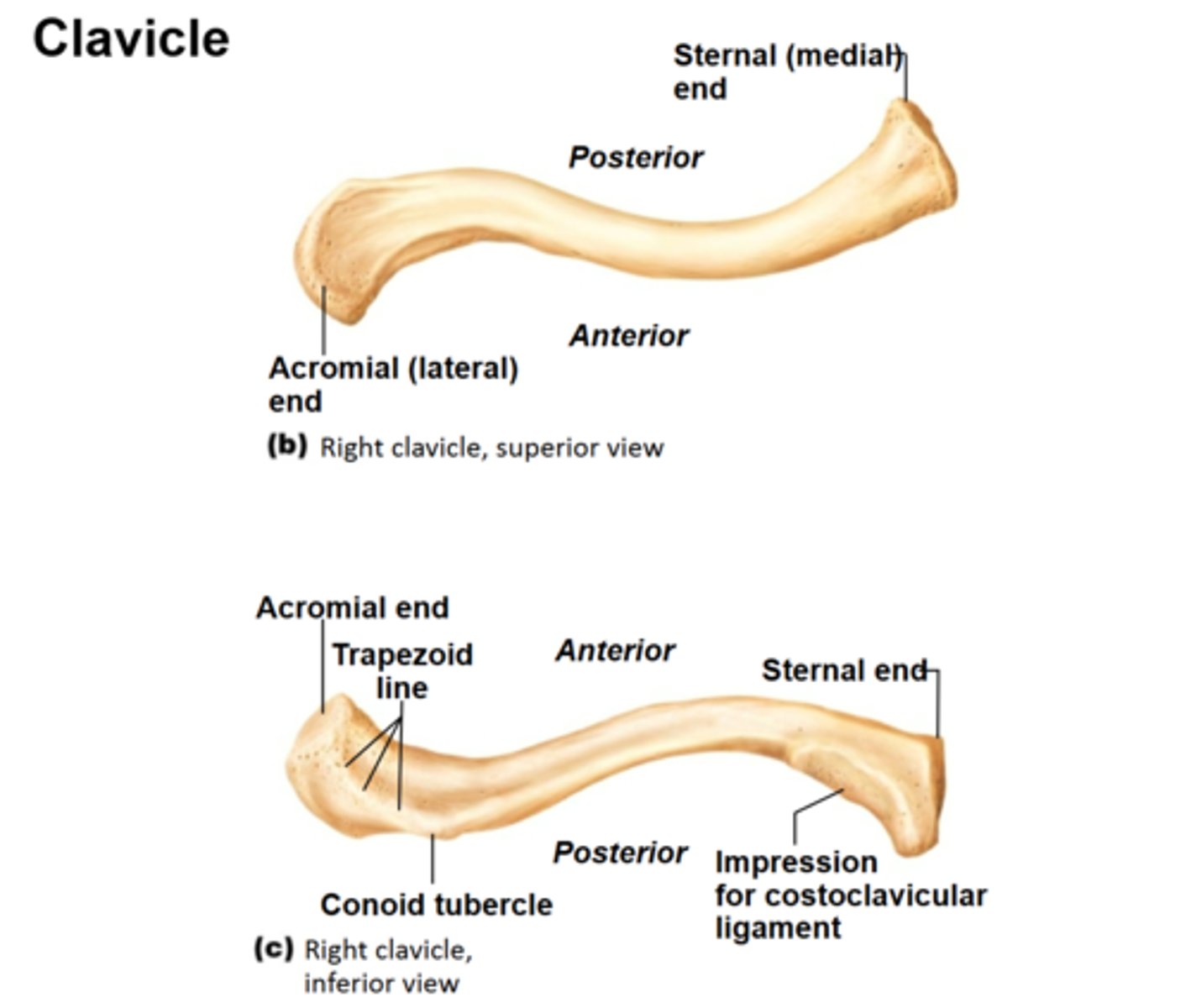
Clavicle
-The upper limb is attached to the clavicle and the scapula.
-The two ends of the clavicle: the sternal/medial end and the acromial/lateral end. The acromial end articulates with the scapula.
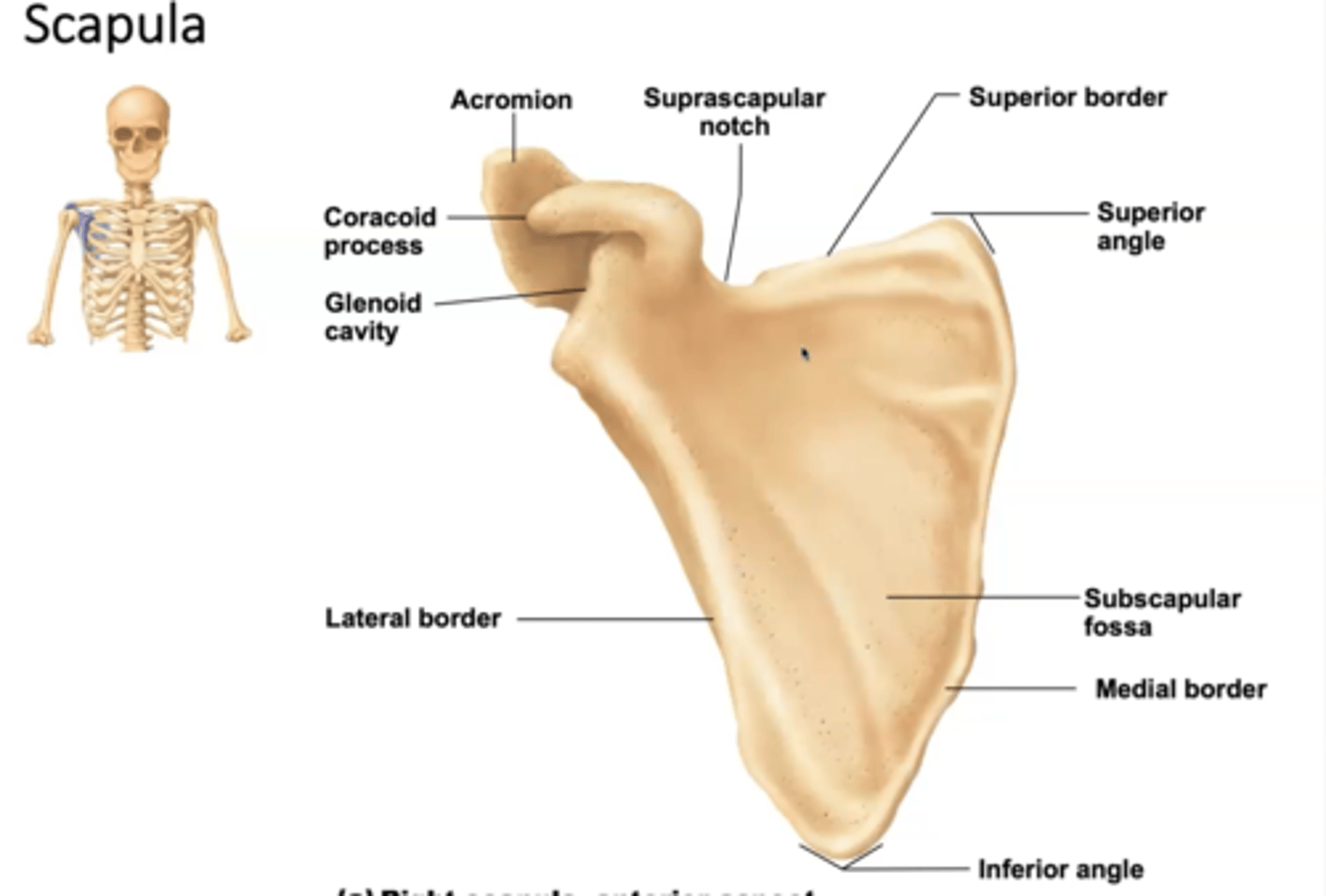
Scapula
-Irregularly shaped bone that has a smooth side for the ribs in the posterior aspect, and the other side for the spine.
-The scapula is home to the rotator cuff muscles. In the subscapular fossa the first of the four rotator cuff muscles is present, known as the subscapularis. These rotator cuff muscles are named after the fossa they lean on.
-Coracoid process: ligament and tendons attachment (unique).
-Glenoid cavity: where the head of the humerus articulates.
-Acromion: posterior-facing structure. Articulates with the clavicle, with the acromial/lateral end. First of the shoulder joints: Acromion clavicular joint.
Spine: landmark structure, that helps with orientation, it is located posteriorly, and at the very end of it, the acromion is present.
-Everything above the spine is the supraspinous fossa.
-Below the infraspinatus fossa, where the infraspinatus is located.
Rotator Cuff Muscles
-Supraspinatus
-Infraspinatus.
-Teres Minor.
-Subscapularis.