Neuro E2- Movement disorders
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
What does damage to the basal ganglia cause?
movement disorders (does NOT cause weakness)
What does damage to the substantia nigra result in?
less dopamine, imbalance between GABA & Ach (like in PD)
What is a rhythmic oscillatory movement, enhanced. by emotional stress and disappears during sleep?
tremor
What kind of tremor is present during sustained posture?
postural / action tremor
What kind of tremor is associated with/ fear or fatigue?
physiologic tremor
What kind of tremor is present during planned voluntary movement but NOT present at rest, and may be associated with a cerebellar lesion?
intentional tremor
What tremor occurs when limb is at rest?
resting tremor
What is rapid irregular muscle jerks that occur involuntarily & unpredictably, involving only one body part at a time but “skips” from 1 part to another randomly?
chorea
What is a milkmaid grasp?
hand grip relaxes intermittently (seen with chorea)
What do patients with chorea have difficulty with?
maintaining muscular contraction for strength testing, also milkmaids grasp, irregular & unsteady gait, and speech irregular in volume/temp (explosive)
What is a violent, unilateral chorea involving sudden, wild, flail like movements of proximal muscle groups, and is most often due to vascular disease in the contralateral sub thalamic nucleus?
hemiballismus
What kind of movement is this?
slow, sinuous, writhing in characteri
flow to different parts of body (rather than skip)
flex, extension, pronation, supination of fingers & hands (proximal limbs)
not present during sleep, may be caused by brain lesion
athetosis
When athetosis is held as a prolonged posture, what is this considered as?
Dystonia
What kind of movement?
sustained muscle contractions causes twisting & repetitive movements or abnormal postures
not present during sleep
enhanced by voluntary activity
dystonia
What is abnormal neck and head posturing?
spasmodic torticollis (cervical dystonia)
What is a blepharospasm?
involuntary B/L contraction of peri-ocular muscles
What condition is generalized dystonia seen in?
cerebral palsy
What are treatment options for dystonia?
anticholinergics (benztropine), dopamine, Backofen, benzodiazepines, botox
What kind of movement?
difficulty/slowness in performing voluntary movements
MC involve repetitive loos perioral and lingual muscles
can be caused by long term medication use (antipsychotics, DA receptor blockers, metoclopramide)
tardive dyskinesia
What kind of movement?/
sudden, rapid, very brief twitch ike muscle contractions
spontaneous or brought on by stimulation/initiation of movement
generalized or focal
myoclonus
What are treatment options for myoclonus?
anticonvulsants (VPA) & benzodiazepines (clonazepam)
What kind of myoclonus involve twitches that may awaken patient from sleep, including hiccups?
physiologic / nocturnal myoclonus
What is a form of myoclonus associated with hepatic encephalopathy (liver flap)?
asterixis (negative myoclonus)
If you ask a patient to extend their wrists like their stopping traffic and it causes rhythmic hand flapping, what should you think of?
liver issues (asterixis)
What kind of movement?
sudden, recurrent, quick, jerky, coordinated movements of smaller muscle groups; recur in a pattern
suppressing movement can cause anxiety
worse with stress & disappear with sleep
associated with Tourette’s syndrome (chronic)
tics
Transient simple tics that terminate spontaneously usually occur in what population?
children
When do chronic simple tics develop?
any age, usually childhood
When do persistent simple or multiple tics develop?
before age 15, resolution by end of adolescence
If abnormal movements are present since infancy, what is the likely cause?
Cerebral palsy
If abnormal movements begin in early adult life, what is the likely cause?
benign essential tremor or huntington’s
What meds resort tardive dyskinesia or extrapyramidal sx as an ADR?
Metoclopramide, Promethazine, Haloperidol
Abnormal movements in a patient with a history of rheumatic fever is likely what condition?
syndenham’s chorea
What body part do tremors usually spare?
legs
What condition?
unknown cause or autosomal dominant
begins at any age
enhanced by emotional stress, improved by small amounts of ETOH
interferes w/ delicate manual skills, writing, drinking, speaking (one or both hands MC)
benign essential / familial tremor
What is the treatment for benign essential tremors?
propranolol or nadolol, primidone, clonazepam, carbamazepine
surgery: stereotactic thalamotomy, deep brain stimulator
What condition?
reversible, extrapyramidal, spasmodic or sustained involuntary contractions of muscles
arise from a drug induced alteration of dopaminergic cholinergic balance in the nigrostriatum (basal ganglia)
acute dystonic reactions
What drugs can cause acute dystonic reactions?
DA receptor antagonists: neuroleptic/antipsychotics (haldol), phenothiazine anti-emetics
cocaine, street valium, LSD, amitriptyline, lithium, anticonvulsants (phenytoin, carbamazepine)
What occurs with drug induced laryngeal dystonia?
dysphagia & stridor
What occurs with drug induced oculogyric crisis?
involuntary deviation of eyes due to contraction of extraocular muscles
What occurs with drug induced buccolingual crisis?
forced spasms of face, jaw, tongue
What occurs with drug induced opisthotonus?
forced spasm of paravertebral muscles, forcing trunk & neck into hyperextension
What is the treatment for acute dystonia?
emergency - diphenhydramine or benzotropine, discontinue offending drug, admit to ICU if airway involvement
What does failure to respond to repeated doses of an anticholinergic drug suggest?
non-drug induced dystonia
What condition?
adult (elderly) onset neurodegenerative disorder of extrapyramidal system
motor sx usually unilateral
the only neurodegenerative disease that is treatable long-term (but no cure)
parkinson’s disease (PD)
Who is Parkinsons more common in?
onset at 60, M > F
What are the 4 cardinal signs of parkinson’s?
Tremor- resting, “pill rolling”
Rigidity- difficulty moving stiff limbs, inc muscle tone hypertonia
Akinesia- difficulty initiating movement, bradykinesia
Postural instability- flexed stooped posture
What is primary parkinson’s disease?
lost dopaminergic cells in nigrostriatal system causing imbalance b/t dopamine & Ach in corpus striatum
5 stages of disability
What following symptoms are seen with what condition?
difficulty w/ initiation of walking
shuffling gait
monotonous, stuttering, poorly enunciated dysarthria
Dementia & depression common
lead pipe rigidity (continuous inc muscle resistant felt on passive movement)
cogwheel rigidity (ratchet-like fluctuate of muscle resistance felt on passive movement)
ocular- dec blink reflex, dry eyes, apraxia, etc
Parkinsons
What is the name one the scale used to stage PD?
Hoehn & Yahr scale of disability
What is the first line & most effective treatment for PD?
dopaminergics: l-dopa/carbidopa (sinemet)
What are possible SEs of Ldopa/carbidopa (Sinemet)?
N/V, hypotension, arrhythmias
What drugs can be used in addition to levodopa/carbidopa in PD?
COMT inhibitors: Entacapone, Tolcapone
DA agonists: Pramipexole, Ropinirole, Bromocriptine
MAO-B inhibitors: Selegiline, Rasagiline
What SE is seen with Bromocriptine (Parlodel)?
fibrosis of lung, heart, & kidney
What should be avoided with MAO-B inhibitors?
tyramine rich foods like aged cheese or wines (hypertensive effect)
What is the second line treatment for PD?
anticholinergics: Benzotropine (Congentin), Amantadine (Symetrel)
*helo more with tremor & rigidity than bradykinesia
What classic adverse effect is seen with Amantadine (Symmetrel)?
livedo reticularis- vasculitis causing red-blue fishnet mottling
What is important to do with PD patients?
keep as physically active as possible
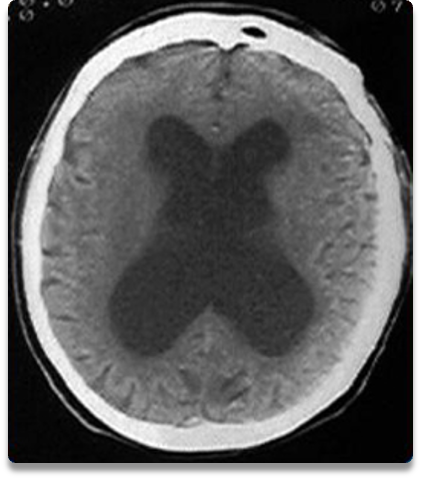
What condition?
pathologically enlarged ventricular size w/ normal opening pressure on LP
reversible w/ ventriculoperitoneal (VP) shunt - important to dx
mimics PD- get CT to differentiate
Normal pressure hydrocephalus (NPH)
What is the classic triad of NPH?
dementia. gait disturbance, urinary incontinence
What condition?
genetic, chronic, degenerative d/o of CNS
chromosome 4- caudate nucleus atrophy, dec in GABA & sub P, inc dopamine
3 manifestations: psychiatric sx, progressive cognitive deterioration, chorea (may manifest last)
Huntington’s disease
What population do you see Huntingon’s disease?
insidious onset after age 30 (lifespan 15 years after), M=F
Early or late ssx of Huntingtons?
anxiety
emotional lability
impaired problem solving
depression
hypotonia
abnormal eye movements
early
Early or late ssx of Huntingtons?
chorea
dementia
dysphagia, dysarthria
incontinence
gait disturbance, postural instability
rigidity, clonus
late
What is the treatment for Huntington’s?
genetic counseling, no known cure, symptomatic tx only
dyskinesia: haldol, tetrabenazine
behavior: clozapine
chorea: clonazepam
rigidity: baclofen
depression: fluoxetine
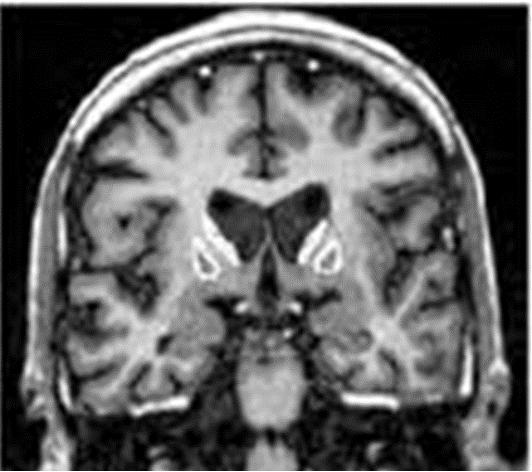
How would Huntington’s disease appear on imaging?
atrophy of cerebral cortex & caudate nucleus
What condition?
acute or insidious onset 2-3 mos after rheumatic fever (GAS infx)
usually subsides in 4-6 mos
abnormal choreiform movements mistaken for fidgetiness, behavior changes (irritable, obsessive-compulsive, emotional labile)
Sydenham’s chorea
What is the tx for Sydenham’s chorea?
eliminate strep infx; consider PCN IM/PO daily until age 20
What condition?
neurological movement disorder associated w/ a sleep complaint
not a true disorder of basal ganglia
“creeping and crawling” usually worse at night
unknown cause; idiopathic or secondary to medications, iron def, lesions, PD, pregnancy, or uremia
Restless leg syndrome (RLS)
What is the diagnostic criteria for RLS?
irresistible urge to move legs ± uncomfortable sensations
urge to move is worse during periods of inactivity, evening or night, & relieved by movement,
What is the treatment for RLS?
non pharm: stretching mental alerting activities, avoid aggravating factors
pharm: Pramipexole, Gabapentin, Benzodiazepines (Clonazepam), opioids