Psych 3501 Exam 3: Cognitive Therapy
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
Philosophical Origins
Stoicism: emphasis on developing self-control as a way to overcome destructive emotions
Goal: to become an unbiased thinker
“Men are disturbed not by things but by the view which they take of them”
Taoism, Buddhism: emphasize that human emotions are based on ideas
Control of intense feelings can be achieved by changing ideas
Phenomenological movement: Heidegger, Kant
We interpret our activities by contextual relations to the world
Alfred Adler: emphasize that it’s important to understand the client from their own conscious experiences to see how they are perceiving the world
We are self-determined by the meaning we give to our experiences
Overall: How we interpret events and experiences will drive our feelings and reactions
Assumptions of cognitive therapy
Cognition represents a synthesis of internal and external stimuli
Appraisal of a situation is evident in cognition
Cognitions constitute a "phenomenal field" which is made up of one's view of self, world, past, and future
Content of cognition affect emotion and behavior
Cognitive theory of depression
Cognitive therapy is developed in the context of depression
Built on four components:
1. The cognitive triad
2. Schemas
3. Automatic negative thoughts
4. Negative attributional style
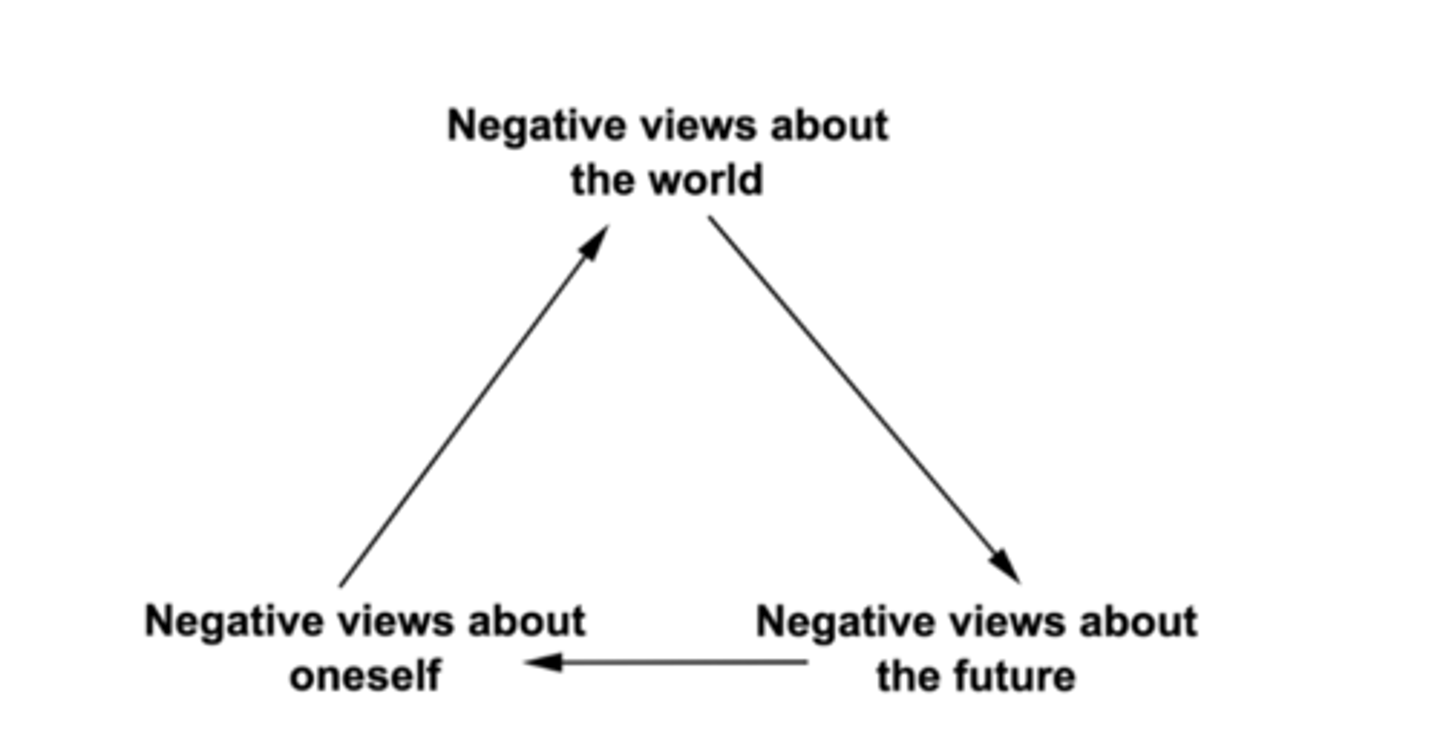
The cognitive triad
Depressed patients tend to have negative views about the world, oneself, and the future
Self: attributing negative events to own defects
World: viewed as hostile, unfair, prevent me from achieving my goals
Future: current difficulties is going to go on forever; expectation of failure
Schemas
Cognitive shortcuts to make navigation quicker, more efficient
Cognitive structure of stored information and memories that forms basis of core beliefs
Constitute basis for screening, differentiating, coding stimuli experienced in a given situation
Determines experience of and response to a situation
Adaptive for efficient information processing
Problematic if negatively biased, rigid, self-perpetuating
Automatic thoughts
Stream of positive and negative thoughts that runs through our minds independent of direct or conscious effort
Automatic, fast, out of voluntary control
Output of negative schemas
event/situation -> schema -> automatic negative thought
Similar to psychoanalysis: events happening without conscious awareness; but not deeply buried
Cognitive biases/distortions
Magnification and minimization
Emotional reasoning
Overgeneralization
Magical thinking
Disqualifying the positive
All-or-nothing thinking
Magnification and minimization
exaggerating or minimizing the importance of events
E.g., believe that own achievements are unimportant or mistakes are excessively important
Emotional reasoning
the assumption that emotions reflect the way things really are
E.g., I feel like a bad friend, therefore I must be a bad friend
Overgeneralization
making broad interpretations from a single or few events
E.g., I felt awkward during my job interview. I'm always so awkward.
Magical thinking
the belief that thoughts, actions, or emotions influence unrelated situations
E.g., Ig I hadn't hoped something bad would happen to him, he wouldn't have gotten into an accident
Common for anxiety disorders (OCD: If I don't washing my hands 7 times, my dog will die)
Disqualifying the positive
recognizing only the negative aspects of a situation while ignoring the positive
E.g., you might receive many compliments on an evaluation, but focus on the single piece of negative feedback
All-or-nothing thinking
thinking in absolutes such as "always", "never", or "every"
E.g., I never do a good enough job on anything
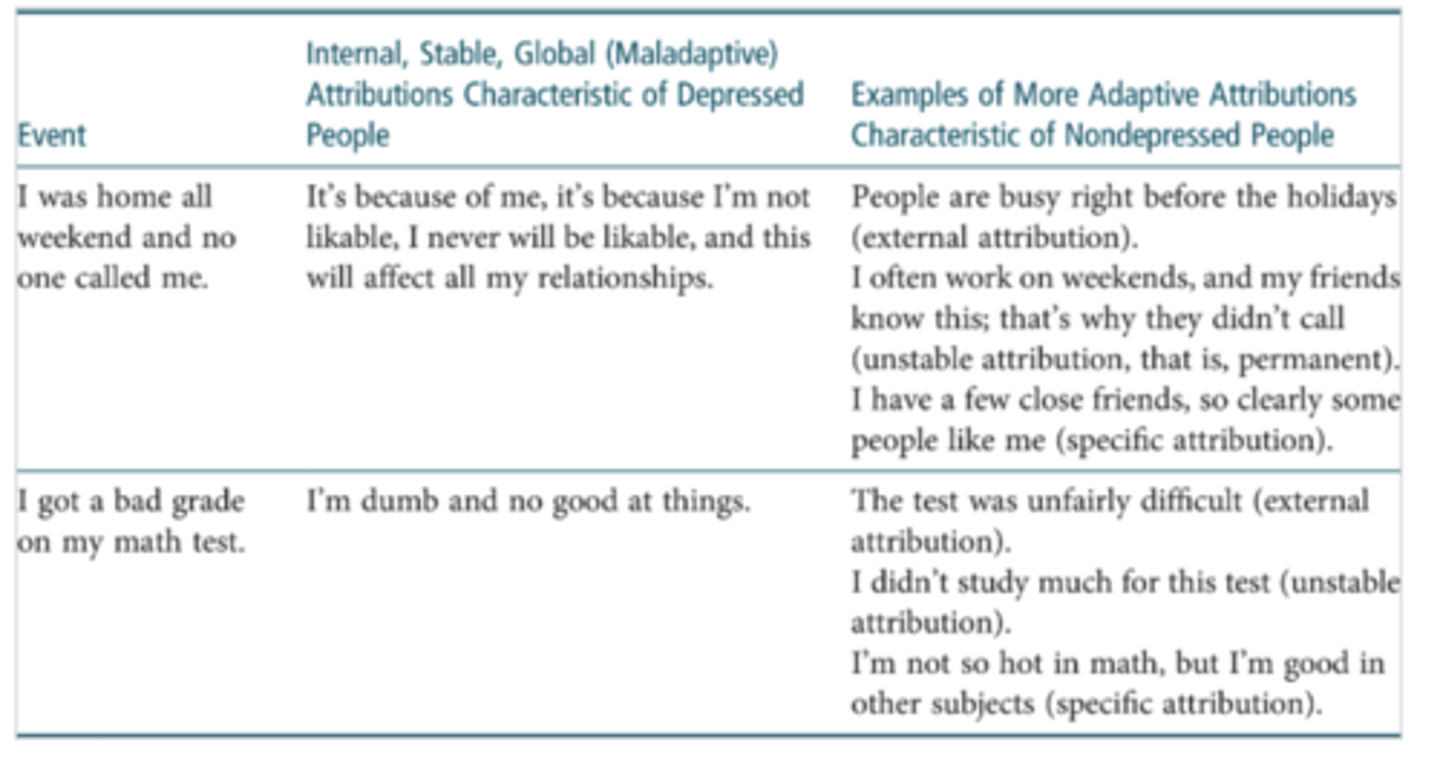
Negative attributional style
Tendency to explain events in way that perpetuates depression
Internal: myself caused the situation
Stable: something that is permanently true, fixed, unchangeable
Global: spread, far-reaching effects
More adaptive attributions: external, unstable, specific
Goals of cognitive therapy
Reduce symptoms by identifying, evaluating, and changing client’s maladaptive cognitions
3 hypotheses:
1. Access hypothesis: client can become aware of their thoughts with training and motivation
2. Mediation hypothesis: thoughts influence emotion and behavior
3. Change hypothesis: thoughts can be modified to improve function
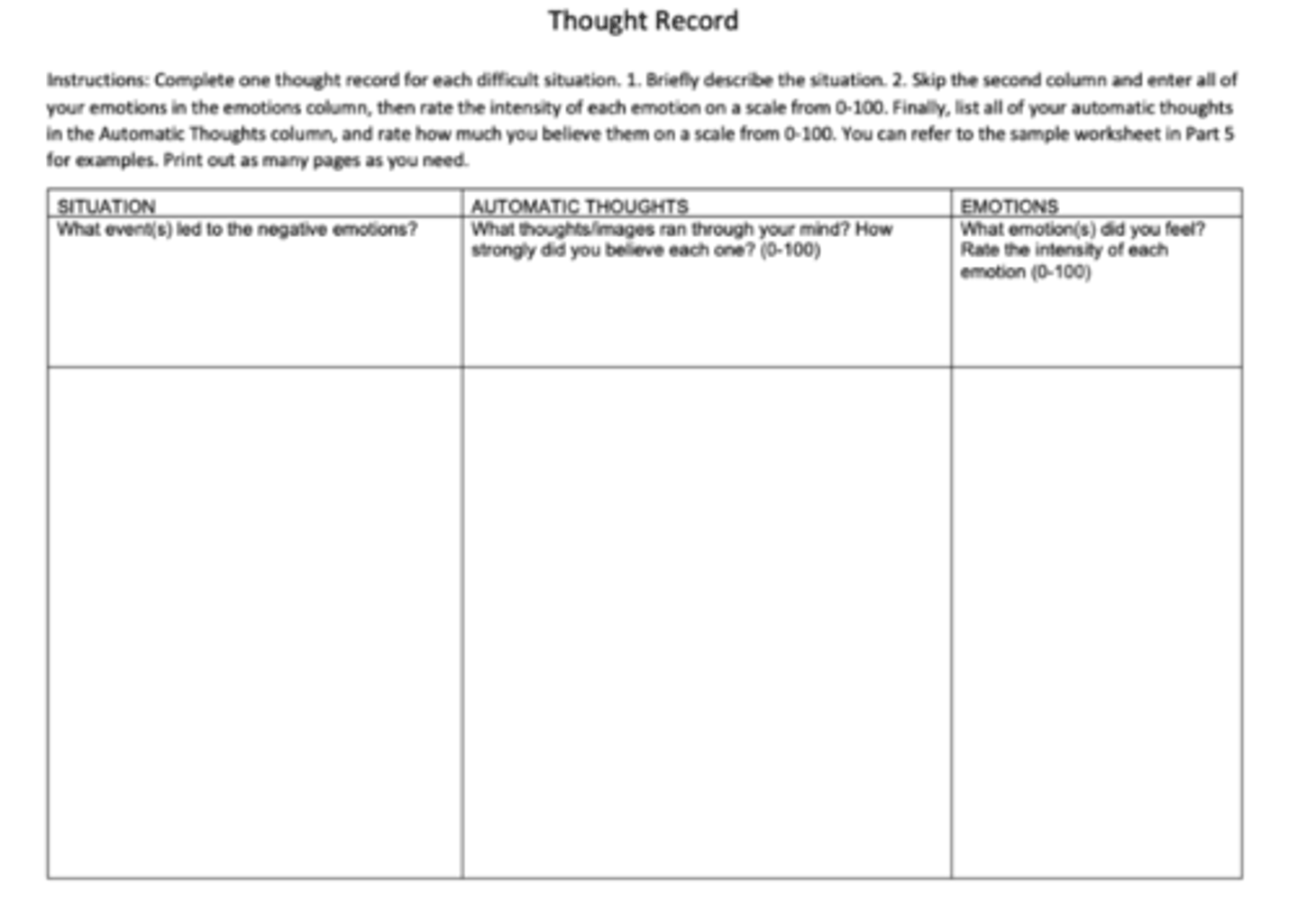
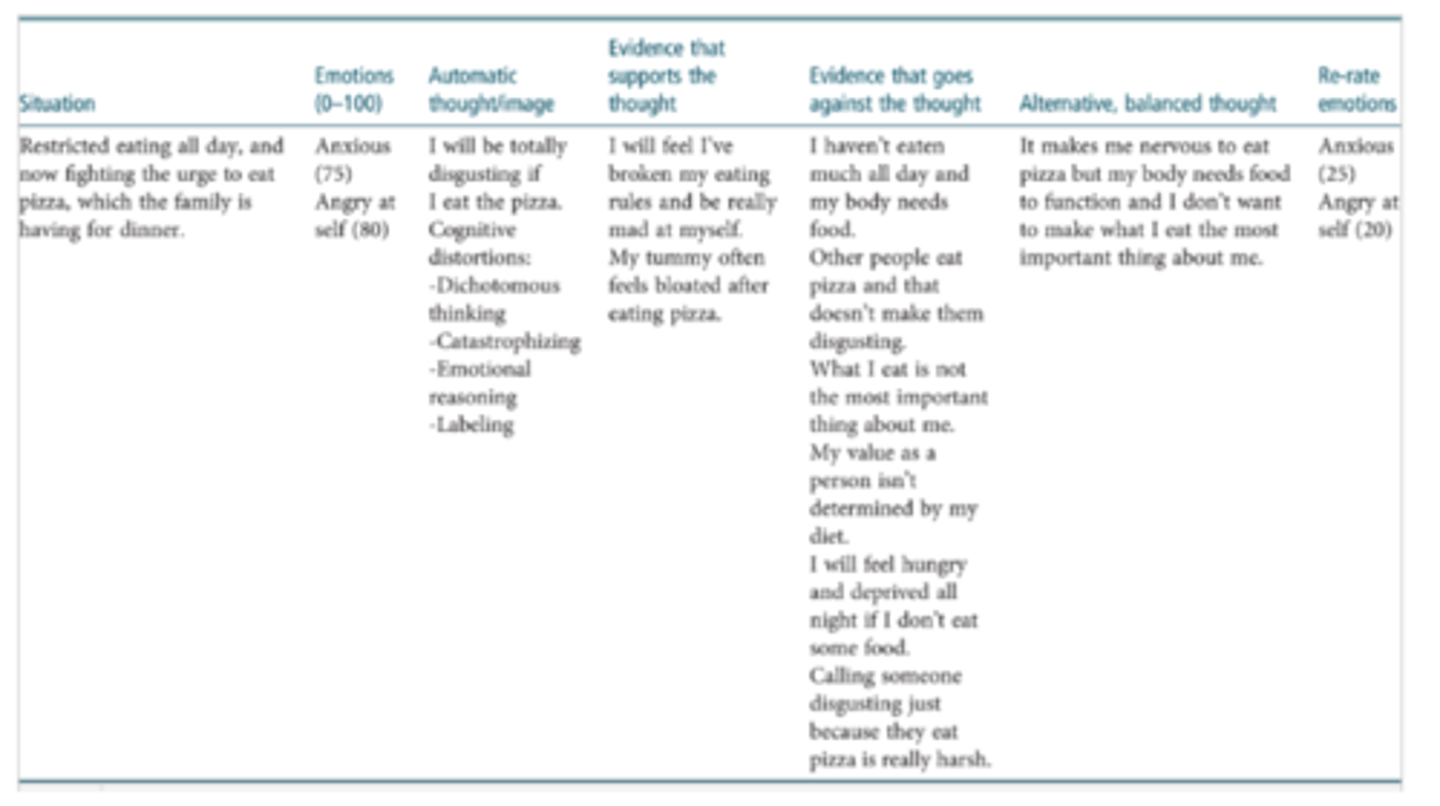
Step 1: help clients develop more awareness of their thoughts - Thought record
Instruct the client to identify the situation, notice emotions, and then identifying thoughts
The columns are structured under the assumptions that thoughts influence emotions
Step 2: Cognitive restructuring: changing thoughts
Once clients are aware of their thoughts, then try to change their thoughts
Process of generating more balanced and adaptive alternative ways of thinking
Four techniques:
- Downward arrow
- Socratic questioning
- Thought records
- Continuum technique
Downward arrow
Technique to identify core beliefs
Core beliefs: underlying negative, broad beliefs that generate specific thoughts
E.g., I’m worthless
Asking about the meaning of an automatic thought until a core belief is discovered
- If that’s true, so what?
- What’s so bad about…?
- What’s the worst part about…?
- What does that mean about you?
Socratic questioning
Asking questions to help reveal patterns in client’s thinking that are maintaining symptoms
Draw attention to information that they filtered out/ignored
Ask with open, genuine curiosity; not arguing with the client/telling them they are wrong/giving advices
- What is the evidence? What is the evidence on the other side?
- Is there an alternative way of viewing the situation?
- What is the worst that could happen? How could you cope with it if it did happen? What is the best outcome? What is the most realistic outcome?
- What is the effect of believing the automatic thought? What could be the effect of changing your thinking?
- What advice would you give if a friend were in the same situation and had the same automatic thought?
Thought records
Structured way for clients to identify automatic thoughts and generate more balanced alternative thoughts and their effect on emotions
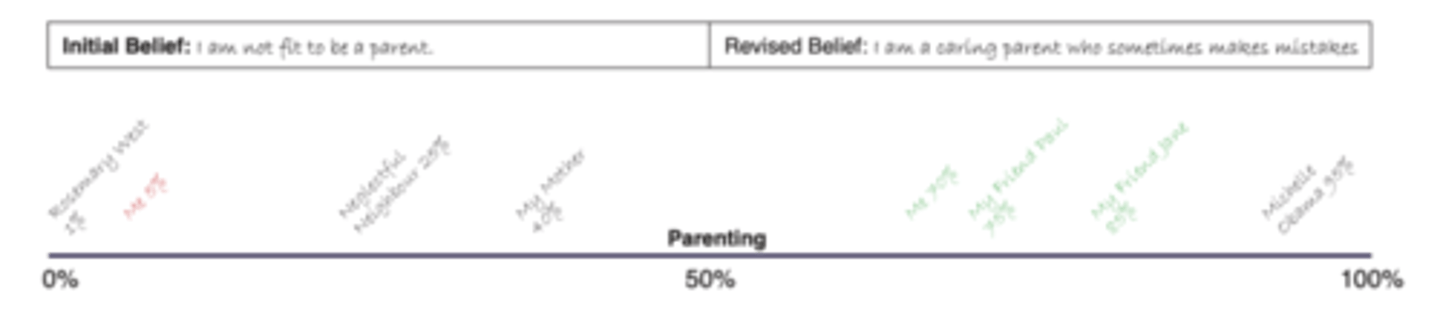
Continuum technique
Help clients recognize extreme thinking and generate a new, more balanced thought or belief
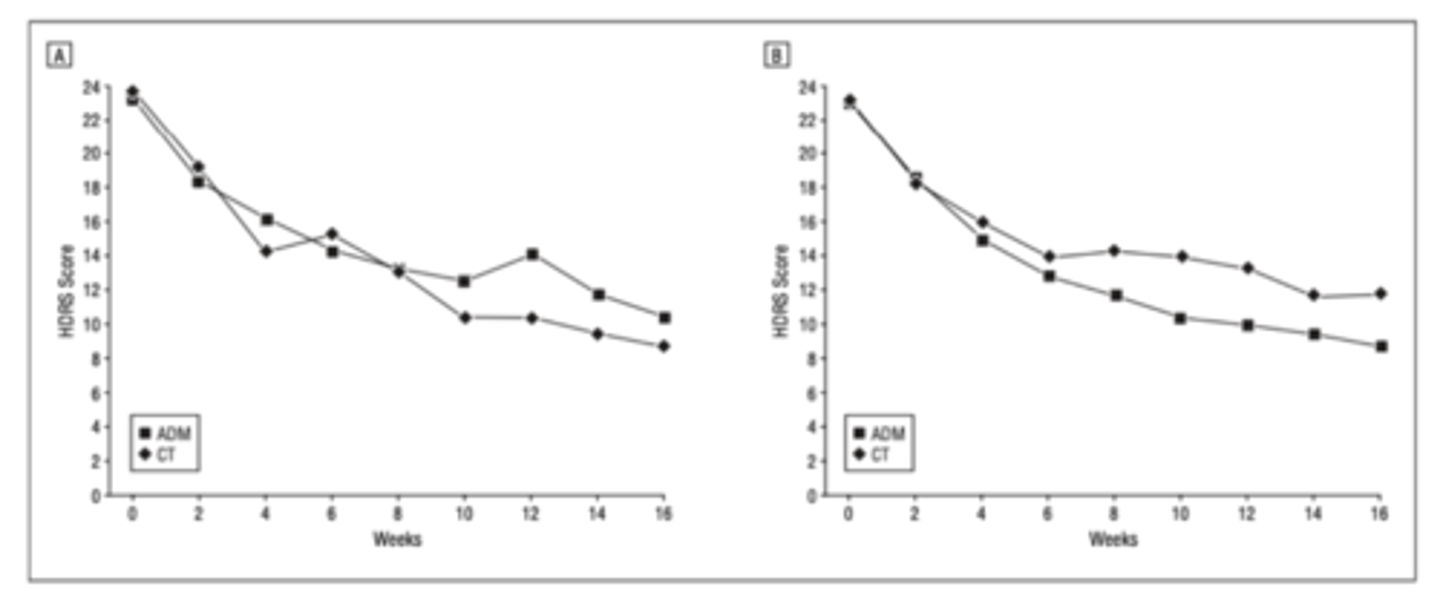
Efficacy of cognitive therapy for depression vs. medication
Antidepressant medication vs. cognitive therapy
Panel A: data from UPenn; Panel B: data from Vanderbilt
Y axis: Hamilton Depression Rating Scale: depression severity
Result: patients who receive antidepressants & cognitive therapy both have significant decreases in depression symptoms pre- to post-treatment, and there is no significant differences
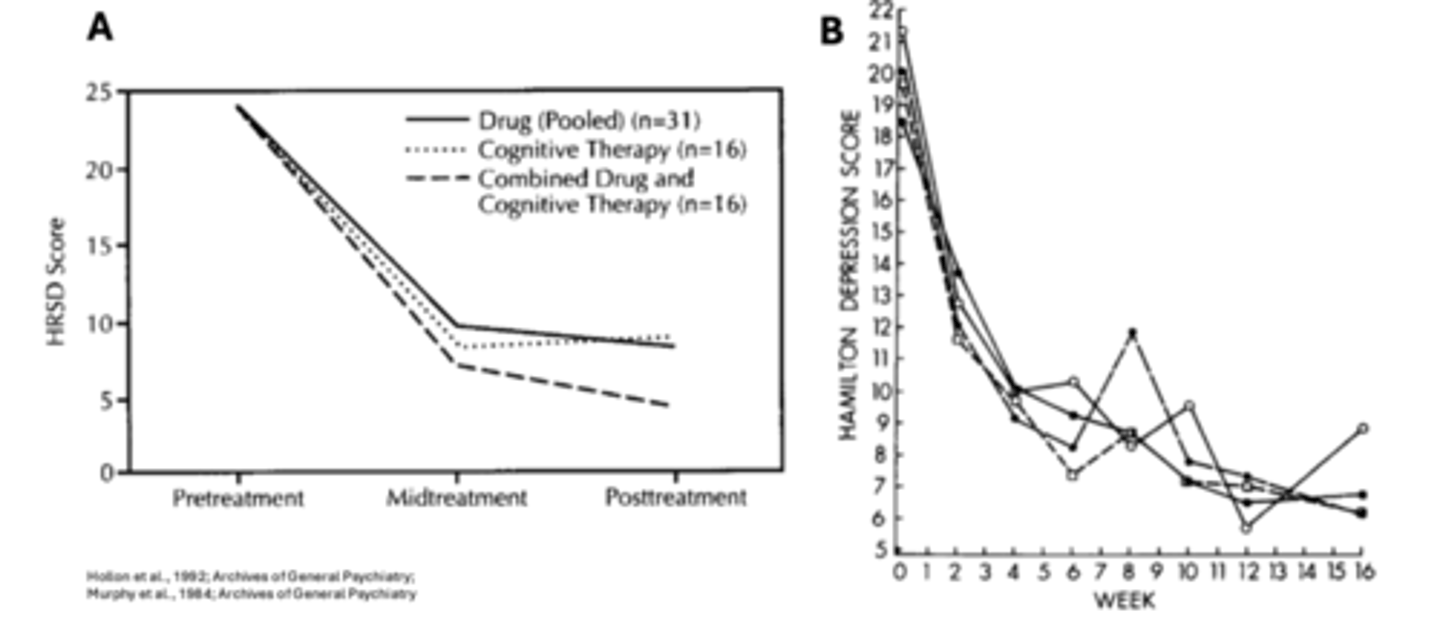
Efficacy of cognitive therapy for depression if combine antidepressant medication and cognitive therapy
Panel A: All three group significantly improved, and there is no significant differences between groups
Panel B: no differences between treatment groups
No benefits from combining antidepressant medication and cognitive therapy
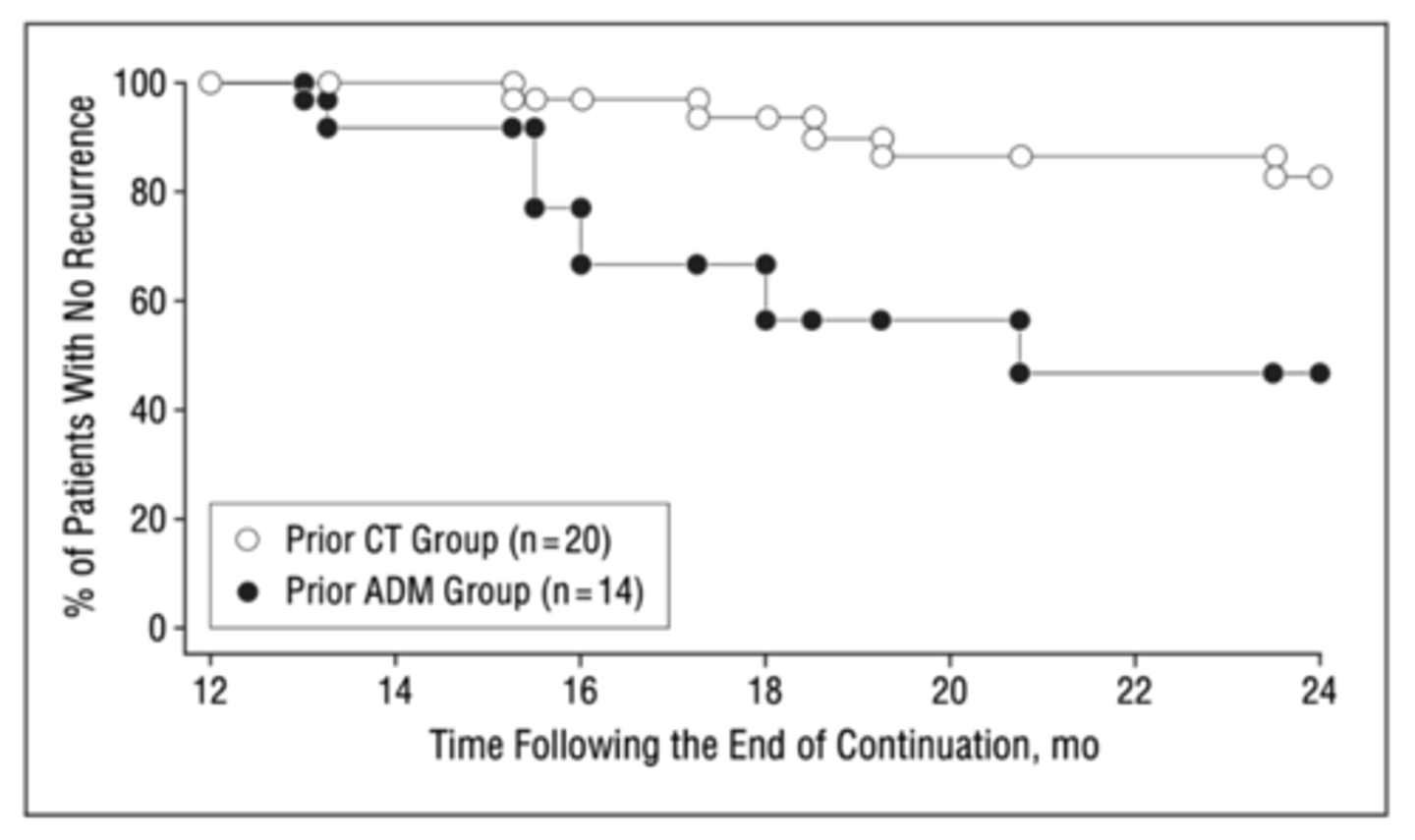
Enduring effects of cognitive therapy for depression
16 weeks of cognitive therapy/antidepressant medication
1 year after treatment termination, followed for another 12 months
Result: those received cognitive therapy previous are less likely to experience depression again over time
Better enduring effects of cognitive therapy compared to antidepressants
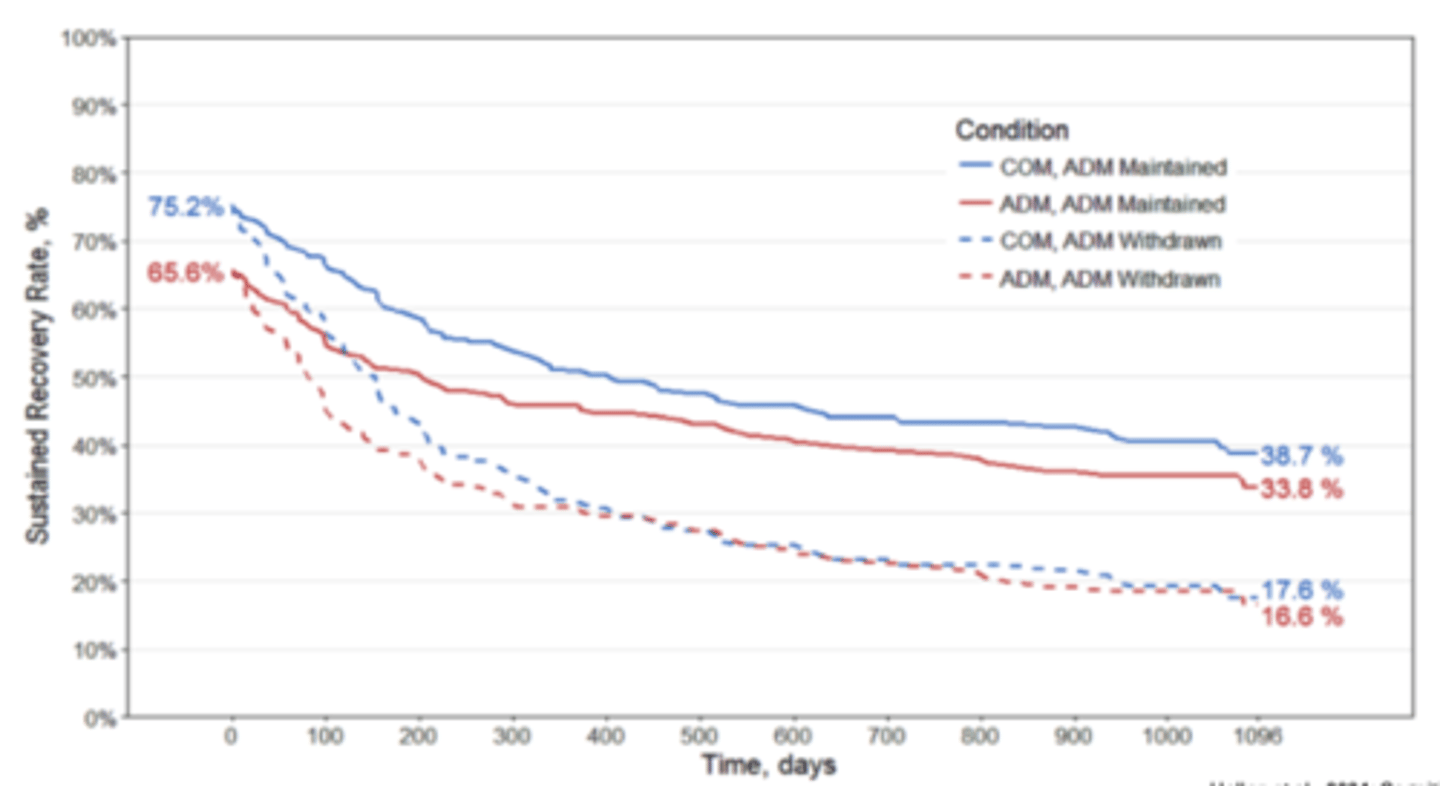
Concerns about combined treatment
Blue line: combined cognitive therapy + antidepressant medication
Red line: antidepressant alone
Result: for those who received combined treatment, the gains from the treatment tend to be lost once the medication is drawn
If you add medication to cognitive therapy, it might limit the enduring effects
No additional efficacy, and may reduce enduring effects over time
Criticisms of cognitive therapy
Limited view of emotion
- Emotion as outcome
Ignores interpersonal factors
Insufficient attention to therapist-client relationship
Requires insight, intellectual engagement
Summary