PRIMARY LESION
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
primary lesion
are those lesions that arise de novo
the most characteristic of the disease process
changes in your skin that aren't associated with other conditions
7 most common types of primary lesions
macules
papules
nodules
pustules
bullae
tumescence
vesicles
wheal (mosquito bite size; skin test)
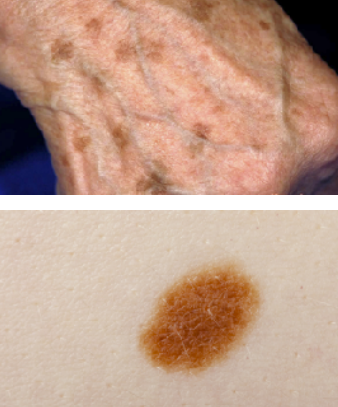
macules
size of a pin head to several centimeters
flat well circumscribed colored area of tissue that varies in size color & shape
example of macules
freckles
flat moles
petechiae
measles
color of macules
red-brown-white- black
3 types of macules
pigmentary
erythematous
petechia & ecchymosis
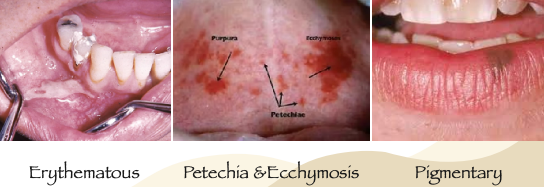
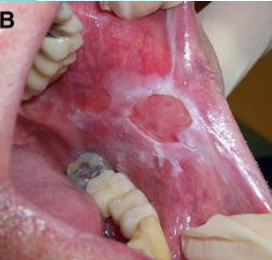
erythematous
its color fades away when pressure is applied
simple erythema caused by localized congestion in the vascularized bed

cause of erythematous
chemical (caustic drugs)
thermal (hot & cold beverages)
clinical features of erythematous
red area is tender & painful
blanches on pressures (turns white)
it’s size & shape depends on the caustic agent
aspirin burns
good examples of caustic drugs causing palatal burns which can lead to erythematous macule
common sites of erythematous
buccal & palatal mucosa
management of erythematous
if pain is present prescribe:
analgesic
topical application of hydrocortisone emollient base (kenalog in orabase)
[ majority of these cases are mild & painless ]
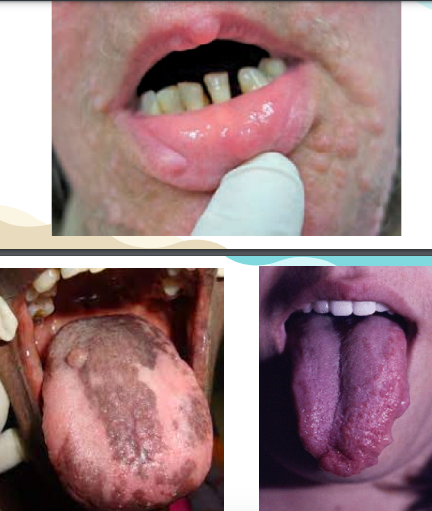
petechia & ecchymosis
the red color does not disappear on pressure
they are considered as subcutaneous or submucosal hemorrhages
palatal patches deserve special attention when it occurs as a solitary lesion at the junction of the hard and soft palate
if examined, it’s immediately red in color but when sufficient time has lapsed it will permit the breakdown of the hemoglobin pigment and turns bluish in color (bluish brown)
color of petechia & ecchymosis
red-brown → results from hemorrhages into the tissue
cause of petechia & ecchymosis
results from hemorrhages into the tissue
due to physical trauma or blunt traumatic insult to the tissue
clinical features of petechia & ecchymosis
borders are poorly demarcated
size varies according to the forces of the physical agents inflicting the damage.
does not blanch under pressure bc the RBC is located within the tissue rather than in the vessels
common sites of petechia & ecchymosis
palate
buccal mucosa
floor of the mouth
management of petechia & ecchymosis
self-limiting and removal of the cause
avoid trauma, usually persist 4-5 days
if continuous episodes, must have a systemic problem and should be examined for presence of hemostatic defects such as thrombocytopenia, leukemia, hemophelia, SBE therefore refer!
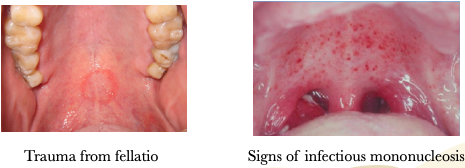
other diagnosis for petechiae & ecchymosis
trauma from fellatio
signs of hemostatic disease
signs of infectious monoculeosis
trauma from severe coughing & vomiting
signs of hemostatic disease
blood testing required to identify the disease or blood dyscrasia
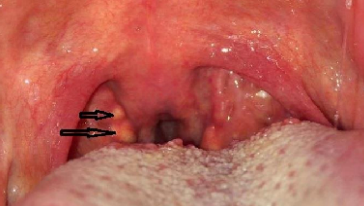
signs of infectious mononucleosis
caused by the epstein-barr virus (EBV)
kissing disease, is transmitted through saliva
glandular fever, malaise, enlarged nodes in the neck
often appears early, sometimes before the patient feels ill
sometimes appears between the 5th or 12th day of illness
small red or purple spots (6-20 petechiae) in the soft palate
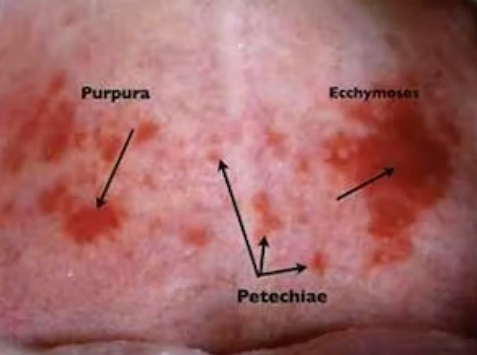
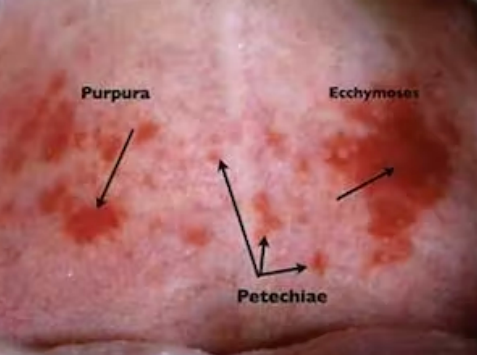
have the same clinical features but differ in size
purpura → 4mm, 10mm
ecchymosis → larger than 1cm
petechiae → pinpoint, less than 4mm
color of pigmentary macules
brown to black extrinsic pigmentation

2 types of pigmentary macules
physiologic pigmentary macules
pathologic pigmentary macules
2 types of physiologic pigmentary macules
mccune albright syndrome
von recklinghausen syndrome
2 types of pathologic pigmentary macules
addison’s disease
peutz jegher syndrome
examples of physiologic pigmentary macules
albinism
melanosis
ephelis (freckles)
smokers melanosis
labial melanotic macule
melanoplakia (black pigmentation)
cause of physiologic pigmentary macules
unknown, but has been postulated that maybe due to trauma or post inflammation
if unusual sign is seen, biopsy test is required to confirm diagnosis
clinical features of physiologic pigmentary macules
light brown to black
deeper & heavier the deposit of melanin, the more darker it appears
lightly tanned individuals → even coloration but dark complexion frequently have macules of pigmentation

melanoplakia
aka: black pigmentation
dark pigmented plaques in the oral cavity
people have discernible degree of melanin pigmentation distributed throughout the epidermis of the skin/mucosa

melanosis
ex: cigarette smoking → stimulates melanocytes
increased / abnormal melanin pigmentation in tissues

albinism
melanin formation is impaired by congenital decrease in tyrosinase

mccune albright syndrome
a disease that affects the bones, skin, endocrine system
it is not inherited & passed down from generation to the next
due to a change (mutation) in a gene that occurs by chance in the womb
majority of this have thyroid problem, like presence of enlargement or masses (nodules/cyst)
cause of mccune albright syndrome
it is caused by mutations in the GNAS1 gene
the mutation is sporadic (occurs in the womb during fetal development)
it is associated with mosaicism → meaning that the abnormal genes is present in a fraction, but not all of the patient cells
symptoms of mccune albright syndrome
range from mild to severe
related to bones, endocrine system & skin
physical examination findings of mccune albright syndrome
acromegaly
hyperthyroidism
precocious puberty
adrenal abnormalities
may experience kidney issues
café-au-lait (birthmark) spots/patches
skeletal deformities and fibrous dysplasia
renal involvement —> up to 50% of patients
mccune albright syndrome in endocrine system
precocious or very early puberty
boys → less noticeable symptoms
girls → early puberty with menstrual bleeding before age 2

mccune albright syndrome in thyroid function
thyroid gland is small in the neck that affects the metabolism
majority have a thyroid problem (presence of enlarge mass nodules/cyst)

mccune albright syndrome in growth hormone (skeleton)
treatment: surgery & medication
excess pituitary growth hormone resulting to:
coarse facial features
larger hands, feet, arthritis

von recklinghausen syndrome
no prevalence for gender and race in NF1
it is an inherited autosomal dominant trait, therefore it is hereditary condition
neurofibromatosis type 1 (NF1)
the most common form of von recklinghausen syndrome.
primary adrenal insufficiency
highly reliable sign of von recklinghausen syndrome (butterfly rash)
skin manifestations of von recklinghausen syndrome
multiple neurofibromas
café-au-lait pigmentation
cardiovascular abnormalities
bone lesions (short statute, scoliosis)
neurological issues (seizures, mental deficiency)
lisch nodules → pigmented hemartomas of the iris (translucent brown spots)
common skin manifestation of von recklinghausen syndrome
multiple neurofibromatosis

oral manifestation of von recklinghausen syndrome
overgrowth of the alveolar ridge
severe periodontitis & calcular deposits
presence of impacted displaced or missing teeth in the mandible
hemifacial disfigurement → caused by plexiform neurofibroma of the trigeminal nerve
common site of von recklinghausen syndrome
tongue, buccal mucosa
radiographic findings of von recklinghausen syndrome
enlarged mandibular canal, mandibular foramen, mental foramen
neurofibroma can develop intraosseously resulting to well demarcated unilocular & multilocular radiolucent lesion
management of pathologic pigmentary macules
if suspected, should not begin treatments seek medical consultation
addisons disease
caused by adrenocortical insufficiency due to immune attack
adrenal glands don’t produce enough of the hormones cortisol and aldosterone.
cause of pigmentation in addisons disease
bilateral tumor metastasis
amyloidosis (protein buildup)
idiopathic atrophy of adrenal glands
leukemic infiltration of the adrenal glands
bilateral adrenocortical destruction (after TB)
S/S of adrenocortical insufficiency
nausea
weakness
weight loss
hypotension
cheek
the most common site for pigmentation → also evident systemic lupus erythematosus SLE (butterfly rash)
management of adrenocortical insufficiency
supplemental corticosteroids medication
—always required prior to dental treatment to cope up with adrenal insufficiency during stressful treatment
peutz jegher syndrome
an autosomal dominant condition
characterized by:
mucocutaneous freckling
hamartomatous polyps of the GI tract (intestinal polyposis found in the jejenum)
common sites of peutz jegher syndrome
buccal mucosa, gingiva, hands, feet
similar to ephelides (freckles) but with a peri-oral distribution (around the lips)

subjective symptoms of peutz jegher syndrome
diarrhea
abdominal pain
rectal bleeding

papules
size of a pin head to about 5mm
solid elevation less than 0.5cm in diameter
shape is round to more or less polygonal
circumscribed superficial elevated areas varying in size
eroded or overlaid surface or moist epithelial desquamation
example of papules
wart
lichen planus
elevated moles
allergic eczema
colors of papules
red-yellow-white- bluish red
cause of papules
unknown, maybe due to psychologic problem like deep emotional strain and remission after a personal crisis
other causes of papules
diabetes mellitus
mechanical irritation
galvanic currents (unlike metals)
characteristics of papules
flat, conical, circular
pointed to umbilicate
elevated and raised bumps
common sites of papules
vermillon border
floor of the mouth
buccal mucosa (85%)
gingiva, tongue, palate
management of papules
topical application of cortisone (3x/day)
lichenoid drug reaction
has a clinical feature of lichen planus
caused by:
drugs like beta blockers
antibiotics (tetracycline, streptomycin)
metallic drugs (gold, salts, arsenical, mercury)
anti-inflammatory or nonsteriodal (indomethacin)
management:
removal of causative factor
5 forms of papules
reticular
papular
erosive
atrophic
bullous
reticular papules
ex: striae of wickham
type of papules that has lacework of intersecting white lines

papular papules
type of papules that acne is an example

erosive papules
type of papules that has presence of squamous cells
atrophic papules
type of papules that has presence of carcinoma

bullous papules
type of papules that has malignant lesion


nodules
no pathological reactions
solid elevation 0.5-1cm in diameter
larger than papules, deep seated in submucosa

cause of nodules
may be of traumatic origin
associated with rheumatoid arthritis, leprosy and syphilis
no pathological reactions (not associated with infection, malignancy, or pathological conditions)
examples of nodules
epstein pearls
tonsil nodules
moles, lipoma
bohn’s nodules
erythema nodosum
tonsil nodules
an example of nodules that is seen on the lingual tonsils in lateral base of the tonguefoliate papilla
epstein pearls
due to arises from the mucosa gland elements
an example of nodules that is seen on palates of new born infants. (palatine cyst)

bohn’s nodules
due to remnants of dental lamina, will exfoliate on its own
an example of nodules that is seen on the buccal alveolar ridge of newborn infants

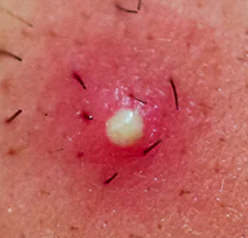
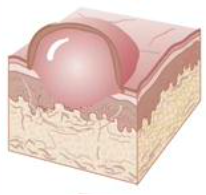
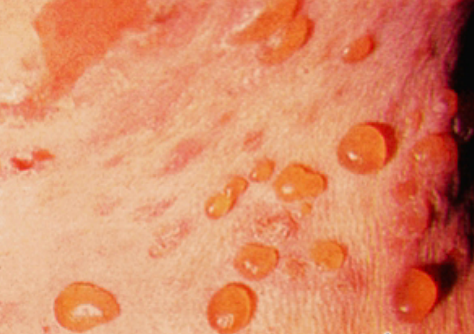
pustules
contains pus, serum fluid surrounded by area of erythema
vesicles but differs from it’s location → infrequent in oral mucosa
considered cutaneous lesion (skin) seen as superficial elevated lesions
example of pustules
acne
impetigo
psoriasis
superficial bacterial disease
psoriasis (pustular)
chronic inflammatory skin condition (itchy, scaly patches)
treatment of pustules
antibiotics
cause of pustules
staphylococci, streptococci
source of infection of pustules
pets
turkish bath
beauty parlor
swimming pool
dirty fingernails

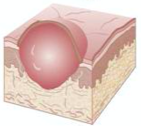
bullae or blebs
has a roof cavity more resistant to rupture
deep seated, larger than vesicles greater than 0.5cm
rubbing of non-vesiculated area may result in a formation to a vesicles or denudation of the mucosa or epidermis. (nikolsky sign) + to stippling off epithelium
examples of bullae or blebs
burn, ranula
pemphigus
behcets syndrome
steven johnson syndrome
ranula
mucous retention cyst on the floor of the mouth

treatment of bullae or blebs
corticosteroid therapy
cause of bullae or blebs
autoimmune mucocutaneous disease → characterized by intra-epithelial blister formation
tumescence
these lesion maybe reactive (non-cancerous) or neoplastic (tumor-related) in character unless confirmed by biopsy
examples of tumescence
papilloma
cyst, torus
tumor, epulis
polyps, exostosis
cyst
fluid-filled sac that can develop in various tissues, often benign

torus
bony growth in the oral cavity, especially in the palate or mandible

tumor
means swelling
solid mass larger than 1cm
abnormal growth of tissue, can be benign or malignant.

an example of tumor
squamous cell carcinoma
epulis
benign growth in the gum tissue, often caused by irritation or trauma.

polyps
abnormal tissue growth, can be benign or precancerous

exostosis
bony overgrowth on the surface of bones, typically benign
papilloma
benign growth caused by the human papillomavirus (HPV)
refers to a small nipple shaped epithelial tumor which cells are covered with finger like process of stroma neoplastic lesion

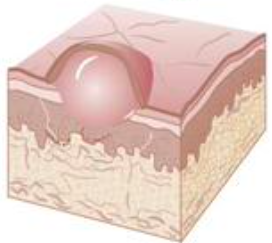
vesicles
small blister consist of fluid, serum, plasma, blood
flat, globoid or umbilicate, tense or flaccid in character
examples of vesicles
chicken pox
herpetic gingivostomatitis