Pediatrics Gastrointestinal
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
mature, small capacity, increased motility, relaxed pyloric sphincter, deficient enzymes, and a immature liver
pediatric differences in GI
6 weeks of age
when can you voluntary control swallowing
frequently regurgitate small amounts of feedings
Relaxed pyloric sphincter allows for
cleft lip + Palate
May occur singly or in combination but is a structural defect
cleft lip
failure of maxillary process to fuse in gestation
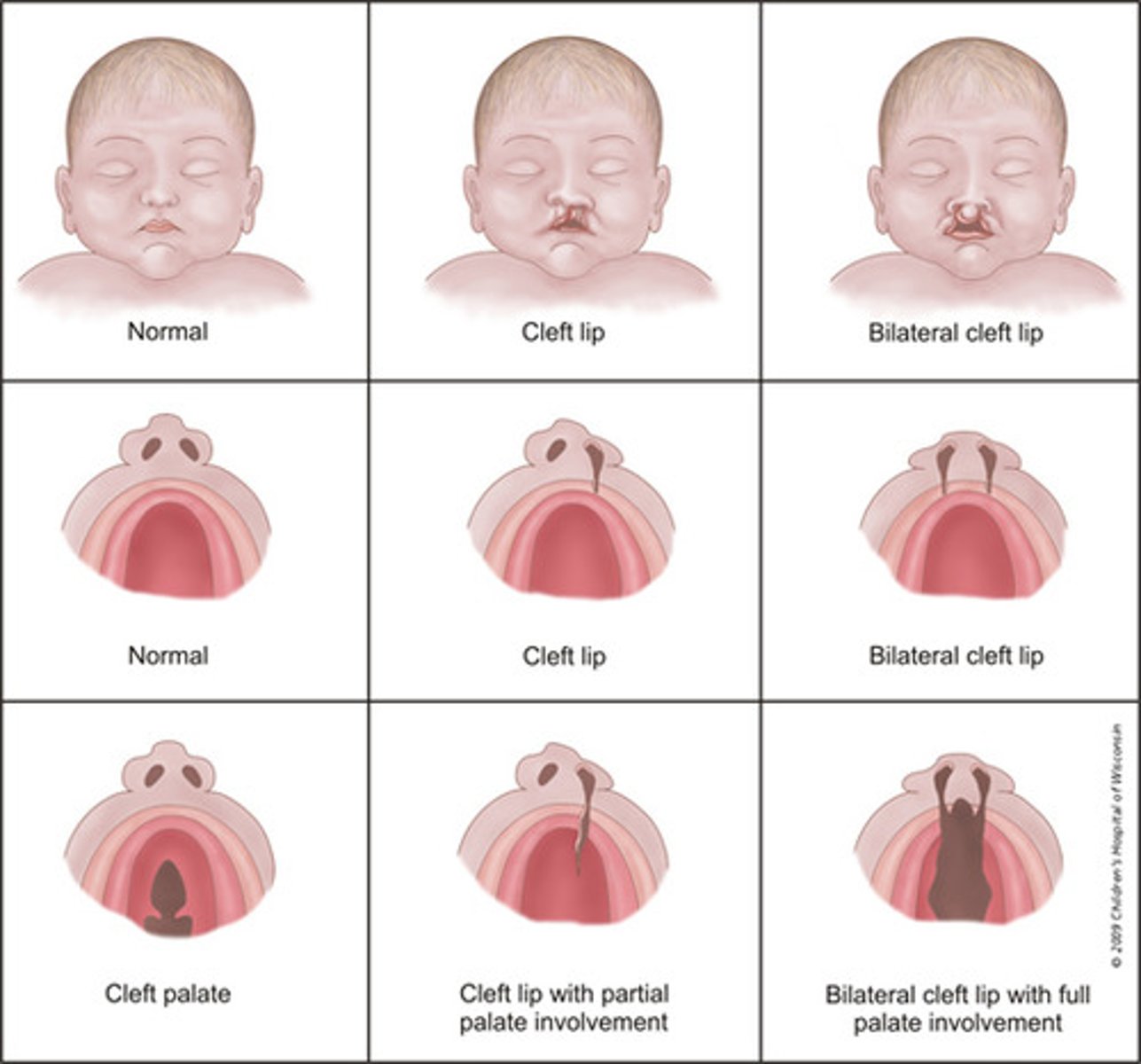
cleft palate
failure of tongue to move down at correct time (prevents palate from fusing)
feeding issues, AOM, speech, hearing, and dental issues
issues seen with cleft lip and palate
first 6 months of life
how long is lip usually impaired for with cleft lip
18 months
when is a cleft palate usually fixed
Nasoalveolar Molding
label appliance

aspiration precaution, keep suction at bedside, position upright with feeds + 30 min after, feed slowly with adaptive equipment, burp often
nursing management of these kids before they get it fixed
elbow immobilizers, prevent prolonged crying, special feeding devices, wound care
post op management of these kiddos with cleft lip/palate
vomit containing large amounts of bile -suggestsbowel obstruction
bilious vomit is
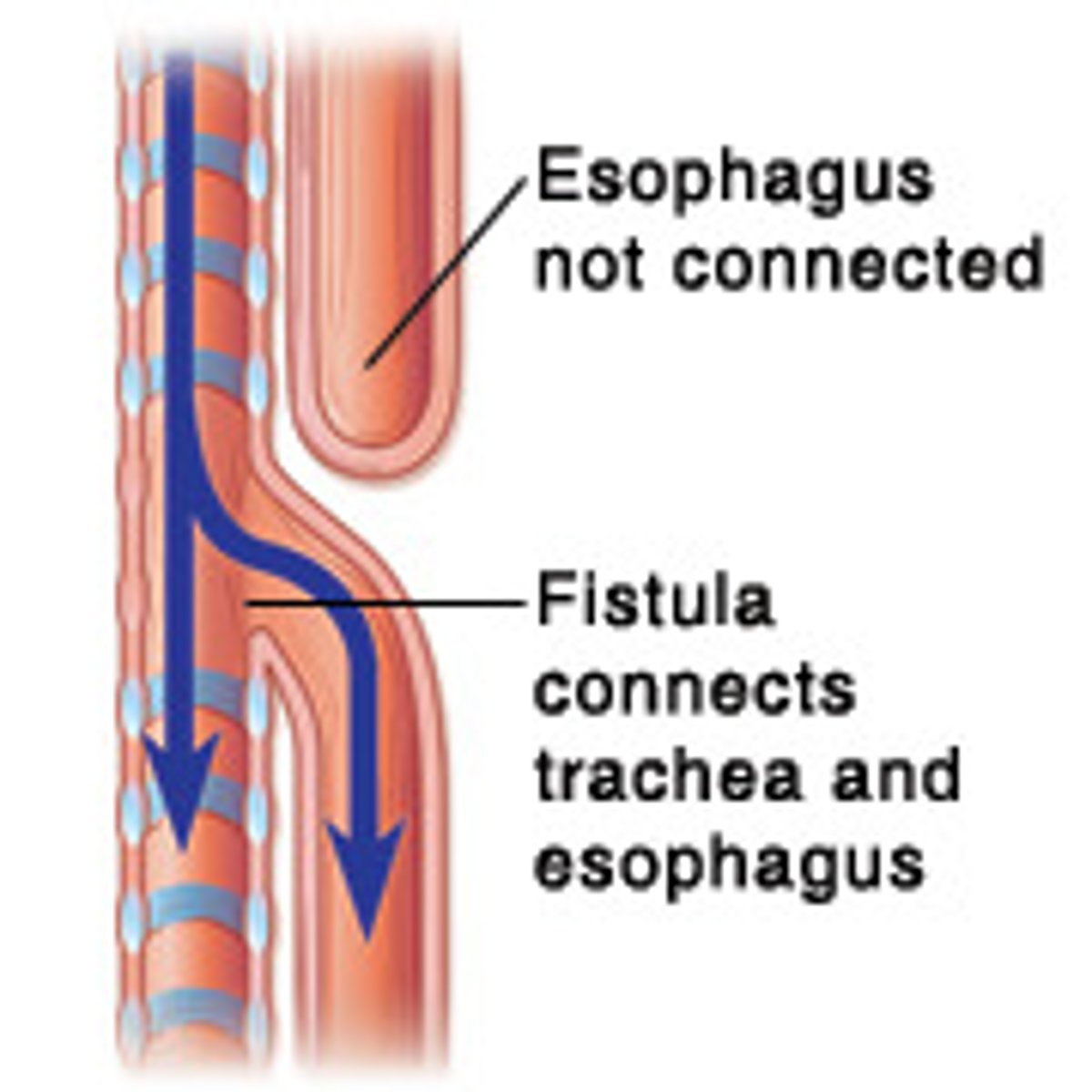
esophageal atresia
It causes the esophagus to end in ablind-ended pouch rather than connecting normally to the stomach
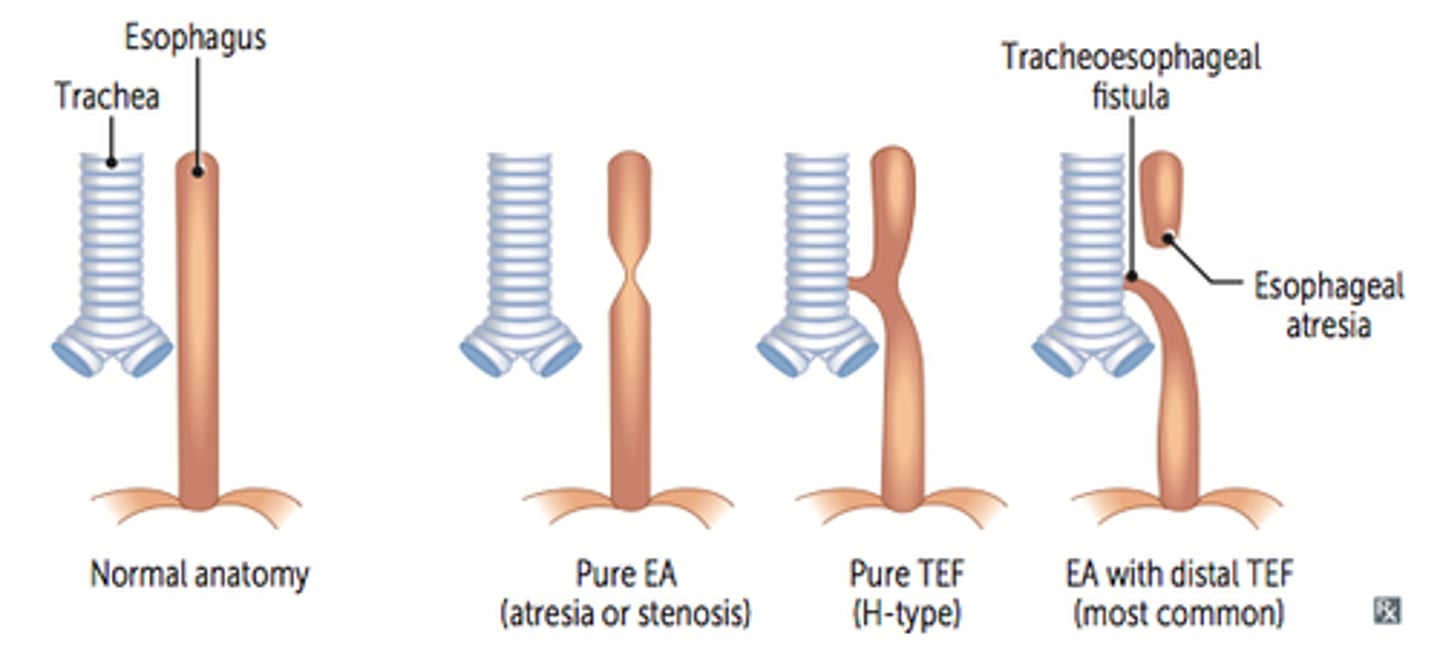
Tracheoesophageal Fistula (TEF)
an abnormal connection (fistula) between the esophagus and the trachea
• 90% of those with esophageal atresia also have a TEF
3 C: cyanosis choking + coughing, and lots of drooling, difficult to feed
s/s of those born with esophageal fistula + TEF
pneumonia
TED + fistula are at risk for
immediate identification, prevent complications, resp + nutritional support
Esophageal Atresia and TEF:Management
confirmed by attempting to pass a nasogastric or orogastric tube into the stomach and it meets resistance or unable to retrieve stomach contents
diagnosis of Esophageal Atresia and TEF
suction, elevate HOB, NPO, IV fluids
Esophageal Atresia and TEF: Nursing Management
gastrostomy tube (GT)
what may be put in place with Esophageal Atresia and TEF
Pyloric Stenosis
Hypertrophic obstruction of the circular muscle of the pyloric canal
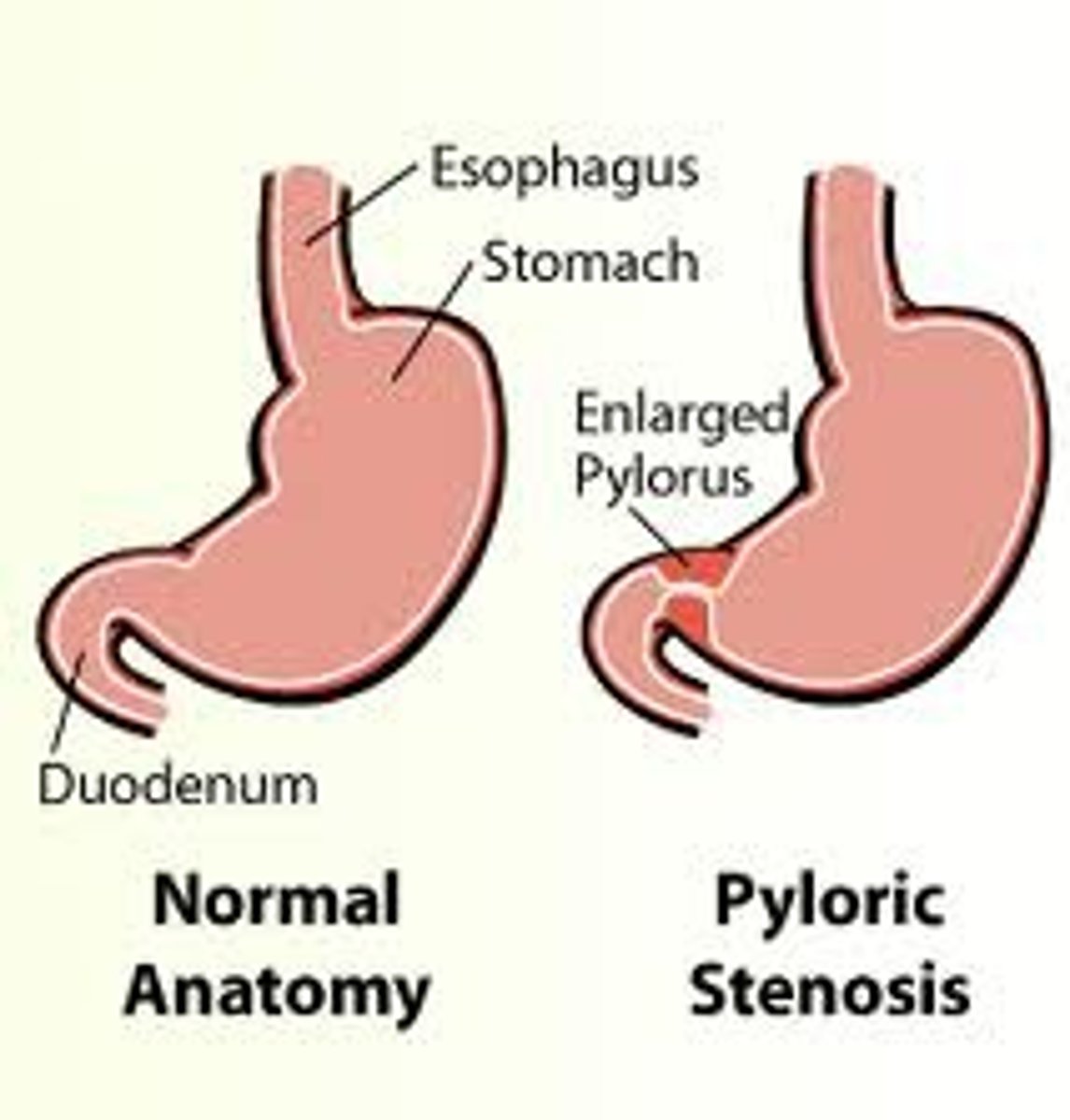
PROJECTILE VOMIT >3 feet and hungry after meals! (nonbilious emesis), irritable, FFT, small stools, dehydrated
what it seen with pyloric stenosis
peristaltic waves across the abdomen and an olive-sized mass in the upper right quadrant
what is seen on exam with pyloric stenosis
abd ultrasound
diagnosis of pyloric stenosis
Gastroesophageal Reflux (GER)
Relaxation of lower esophageal sphincter = return of gastric contents into esophagus
50% of infants have some degree of GER
Lower esophageal relaxations
• Incompetent lower esophageal sphincter
• Anatomic disruption of esophagogastric junction
Three mechanisms allow reflux to occur
pitting up or vomiting, Hungry and irritable, refusal of feedings, poor weight gain,sleep disturbance, respiratory symptoms (coughing, choking, wheezing),arching of back during feedings
Symptoms with GERD
aspiration (resp comp)
GERD are at risk for
Upper endoscopy with esophageal biopsy - assess damage and R/Oother conditions
diagnosis of GERD
Thickened feeds
Slow-feed nipple
Smaller volume feedings
Positioning upright 20-30 minutes after feeding
Feeding modification for GERD
H2 blockers: Zantac + pepcid and PPI prevacid + prilosec (take on empty stomach)
meds for GERD
Umbilical Hernia
Weak or imperfectly closed umbilical ring = soft swelling covered by skin

easily reduced by pushing bowel back through ring, resolved by 1 year or may need surgery
what else with umbilical hernia
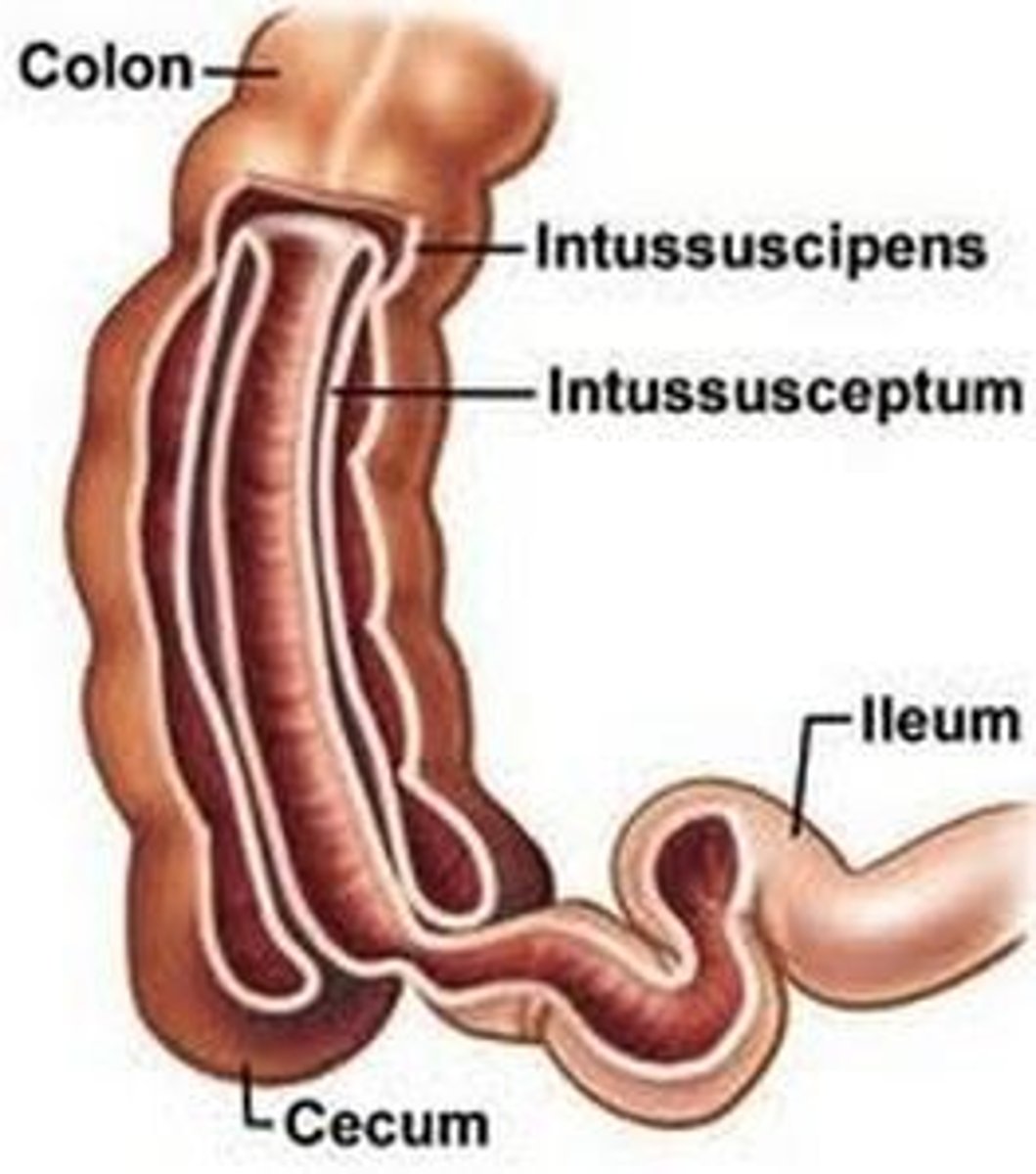
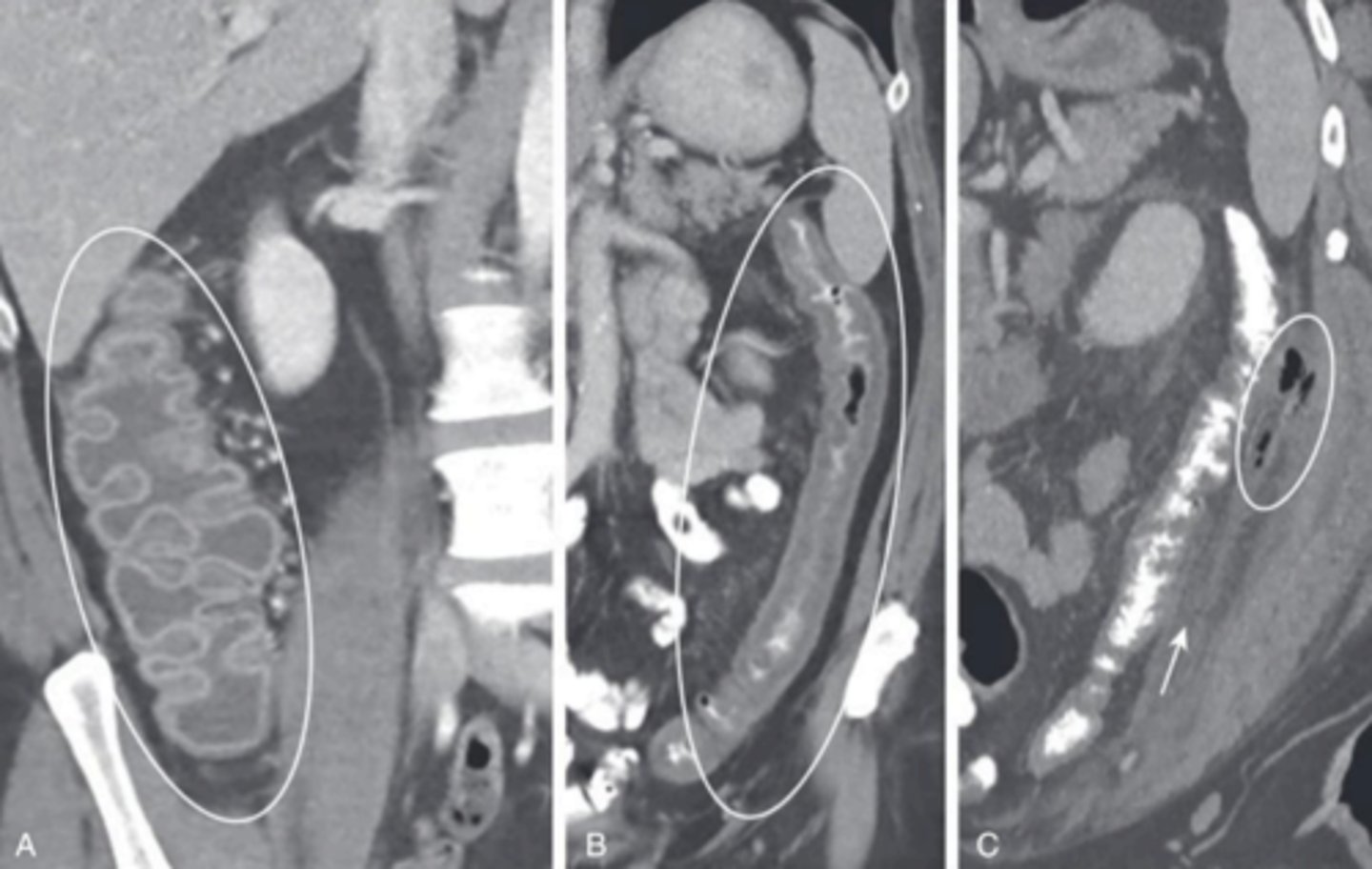
Intussusception
inversion of one portion of the intestine within another.• The telescoping of the intestine obstructs passage of stool
Abrupt onset!
•Abdominal pain
•Vomiting (bilious)
•Red/currant jelly
•Intermittent crying that becomes worse
S/S of intussusception
air contrast edema
management of intussusception
Hirschsprung disease (congenital aganglionic megacolon)
inadequate motility causes mechanical obstruction of the intestine
failure to pass meconium in 24/48 hr, abd distension, bilious vomiting, failure to gain weight + severe constipation
Hirschsprung Disease :Clinical Manifestations
Surgically remove the aganglionic bowel portion; may need temporary colostomy
Hirschsprung Disease: Management
Celiac Disease
Chronic malabsorption syndrome, intolerance for gluten
• Damages villi - impairs absorption in small intestine
solid foods containing gluten are introduced (6months to 2 years)
symptoms occur with celiac when
gluten free
treatment of celiac
Chronic diarrhea, abdominal distention, growth impairment, poor appetite, lack of energy, muscle wasting with hypotonia
s/s of celiac
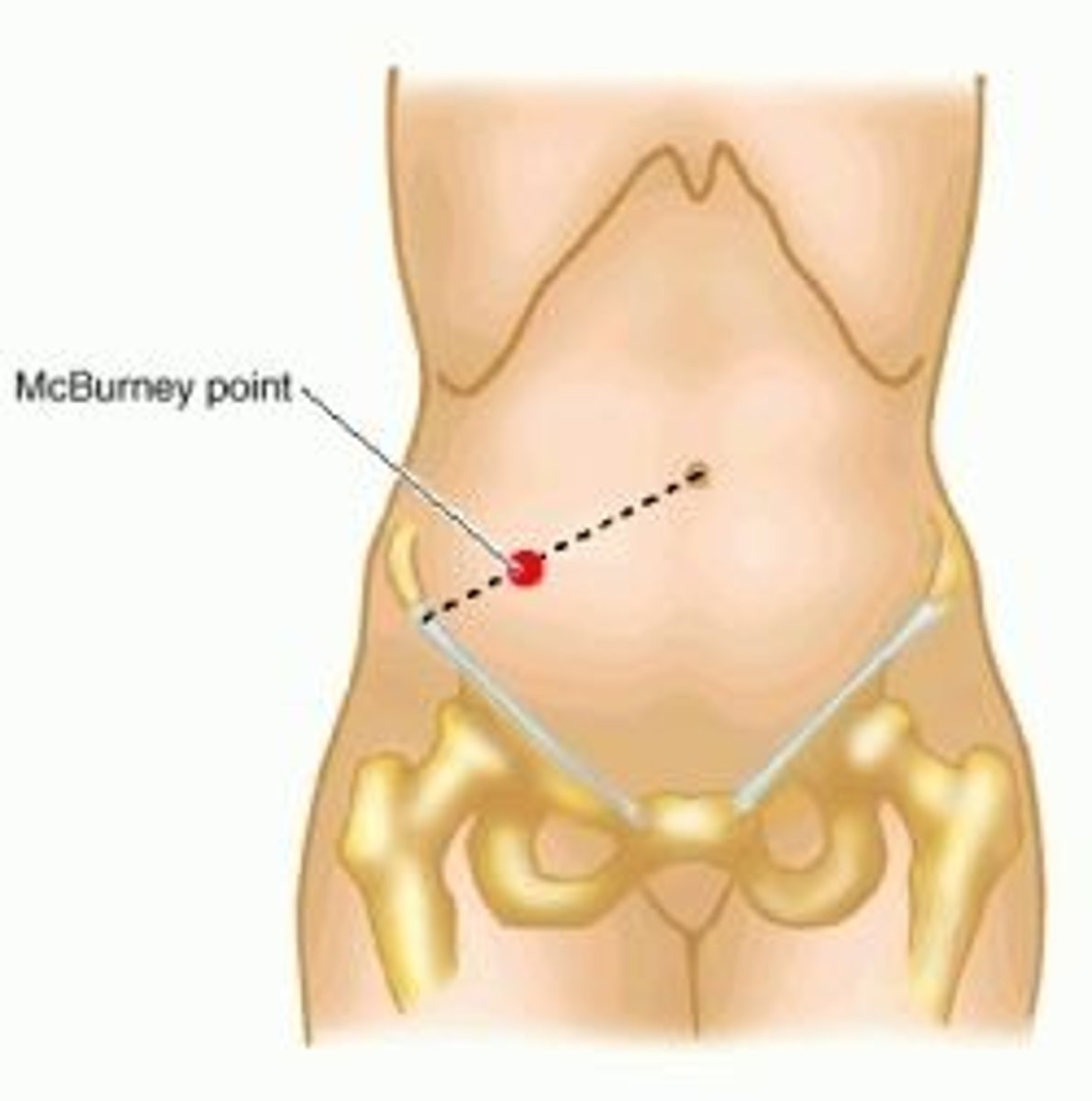
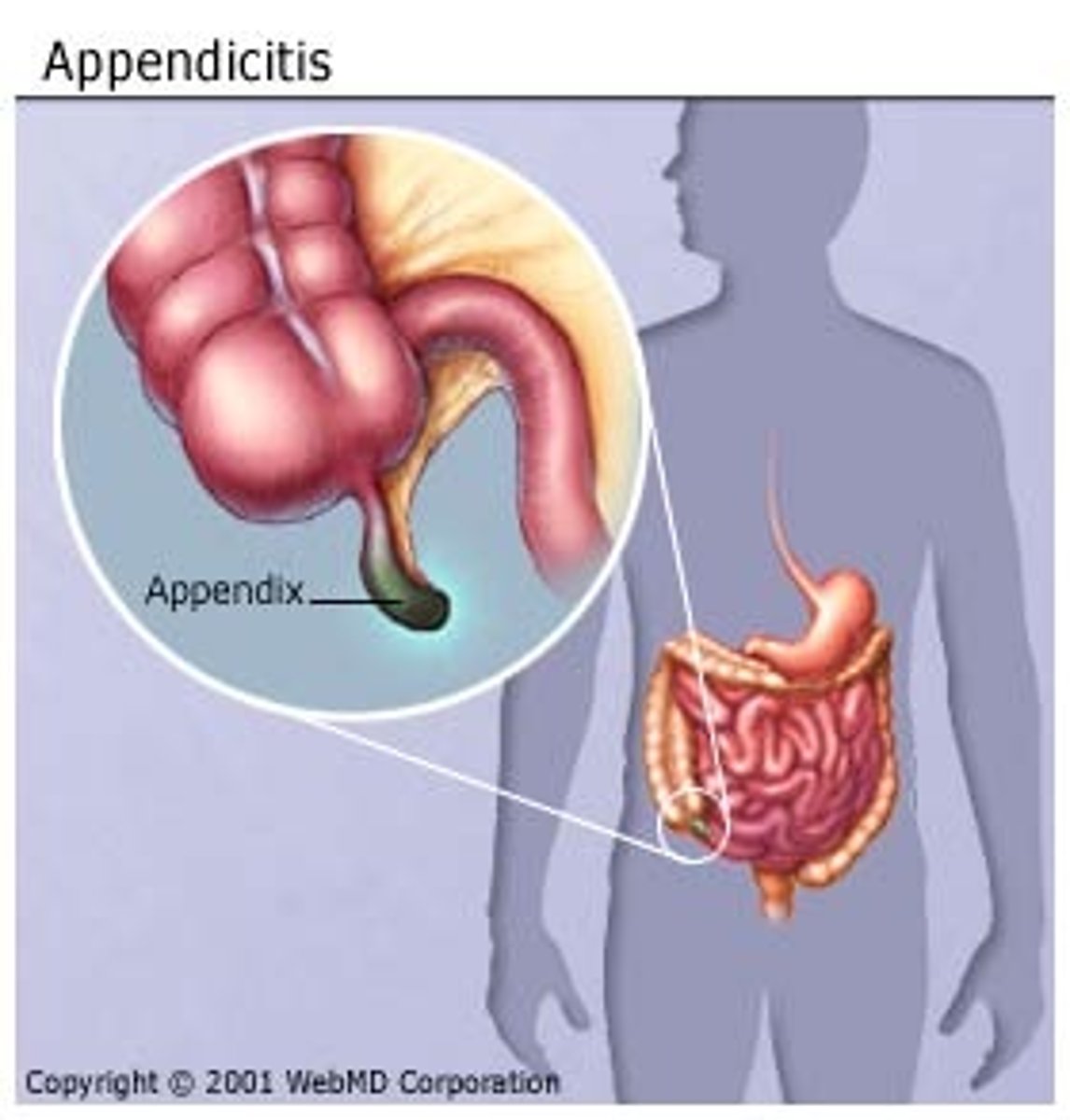
periumbilical cramp, abd tenderness, anorexia, nausea, fever, pain,
Appendicitis: Clinical Manifestations
mcburney's point
Pain in RLQ with appendicitis
NPO, pain, + hydration/antibiotic
pre op appendicitis
NPO, suction to wall, wound care, antibiotics + hydration
post op care
Appendectomy
surgical removal of the appendix
Acute Viral Gastroenteritis
Inflammation of stomach and intestines = vomiting and diarrhea
dehydration
Infants and small children at risk for
loose or watery stools, irritability, anorexia,nausea, vomiting
s/s of Acute Viral Gastroenteritis
tenting of skin, sunken fontanelle, sluggish cap refill,
dehydration manifestations
sodium can go any direction, hypokalemia, elevated BUN, low bicarb
labs seen with dehydration
• Oral rehydration solution (Pedialyte) in frequent, small amounts
• After hydration continue breastfeeding or resume age-appropriate diet
If not improving after 4 hours or worsens seek re-evaluation
mild to moderate dehydration. management
isotonic IV fluids
management of severe cases
normal diet
For all categories: once hydration achieved resume