antidepressants and anxiolytics - lecture 18
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
"food for thought"
"food for thought"
"who cares"
"who cares"
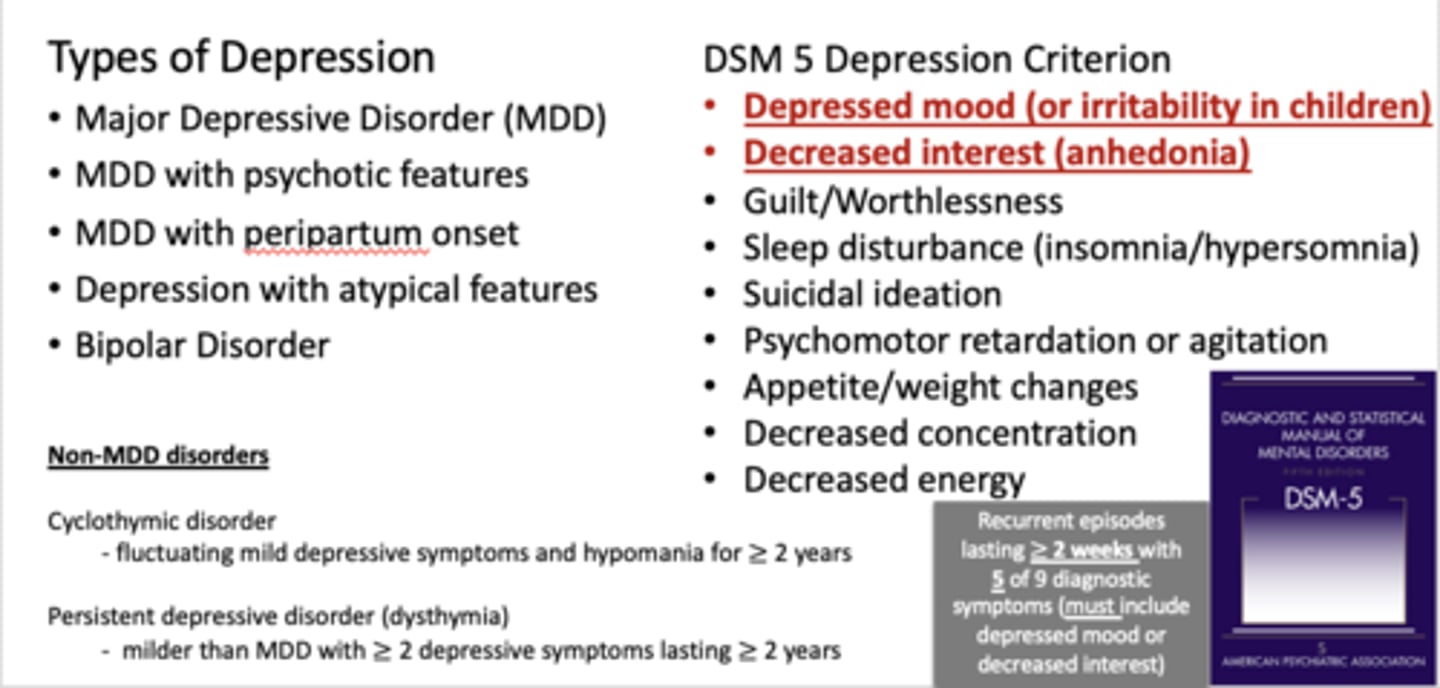
depression overview - KNOW THE RED
note: Recurrent episodes lasting ≥ 2 weeks with
5 of 9 diagnostic symptoms (must include depressed mood or decreased interest)
depression overview - KNOW THE RED
note: Recurrent episodes lasting ≥ 2 weeks with
5 of 9 diagnostic symptoms (must include depressed mood or decreased interest)
Antidepressants
prescribed specifically for affective disorders that are characterized by extreme depression (dysphoria), extreme elation (mania), or both. Major Depressive Disorder (MDD) or Monopolar Depression may affect 15% of all adults during any given year of their lifetime. Treatment usually takes 2-6 weeks and leads to 85% remission.

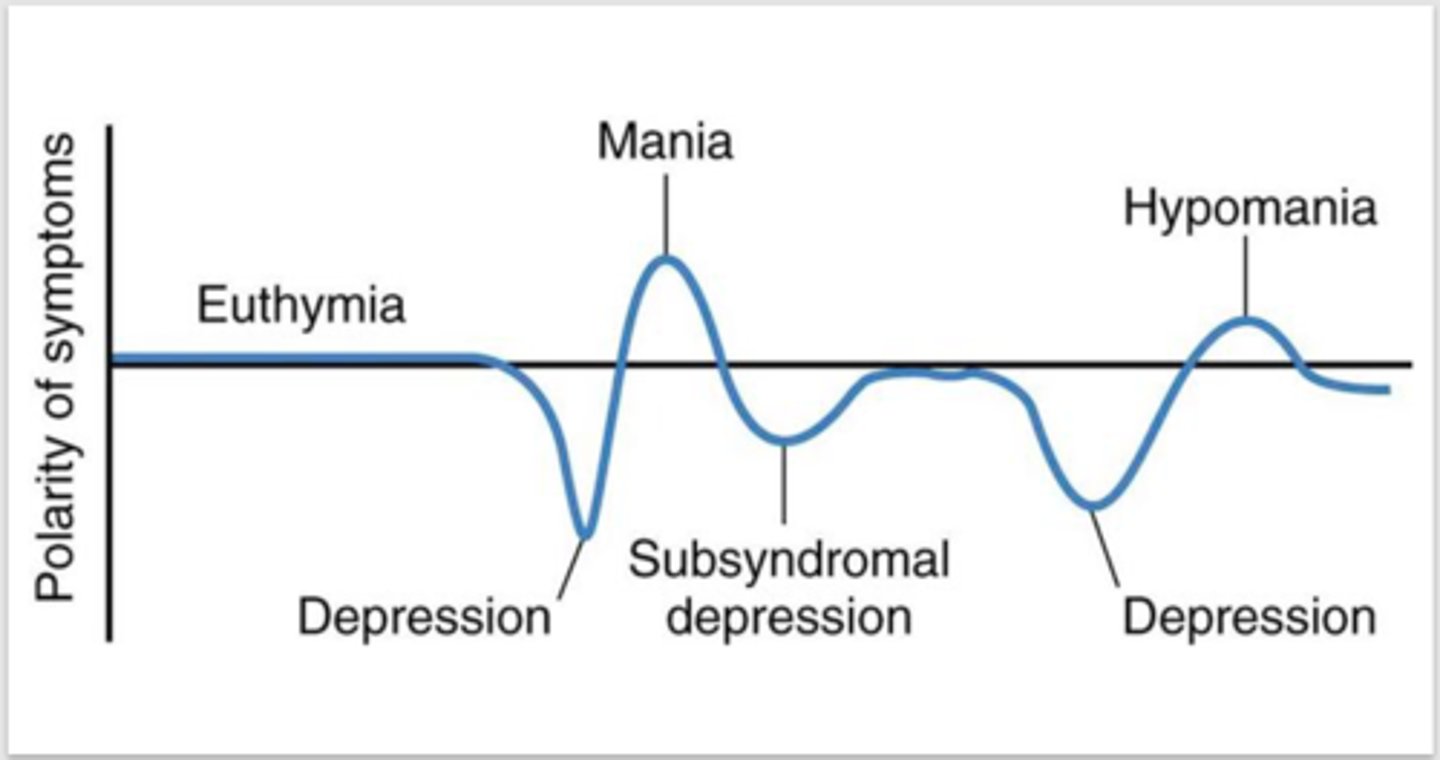
polarity of symptoms
polarity of symptoms
major depressive disorder
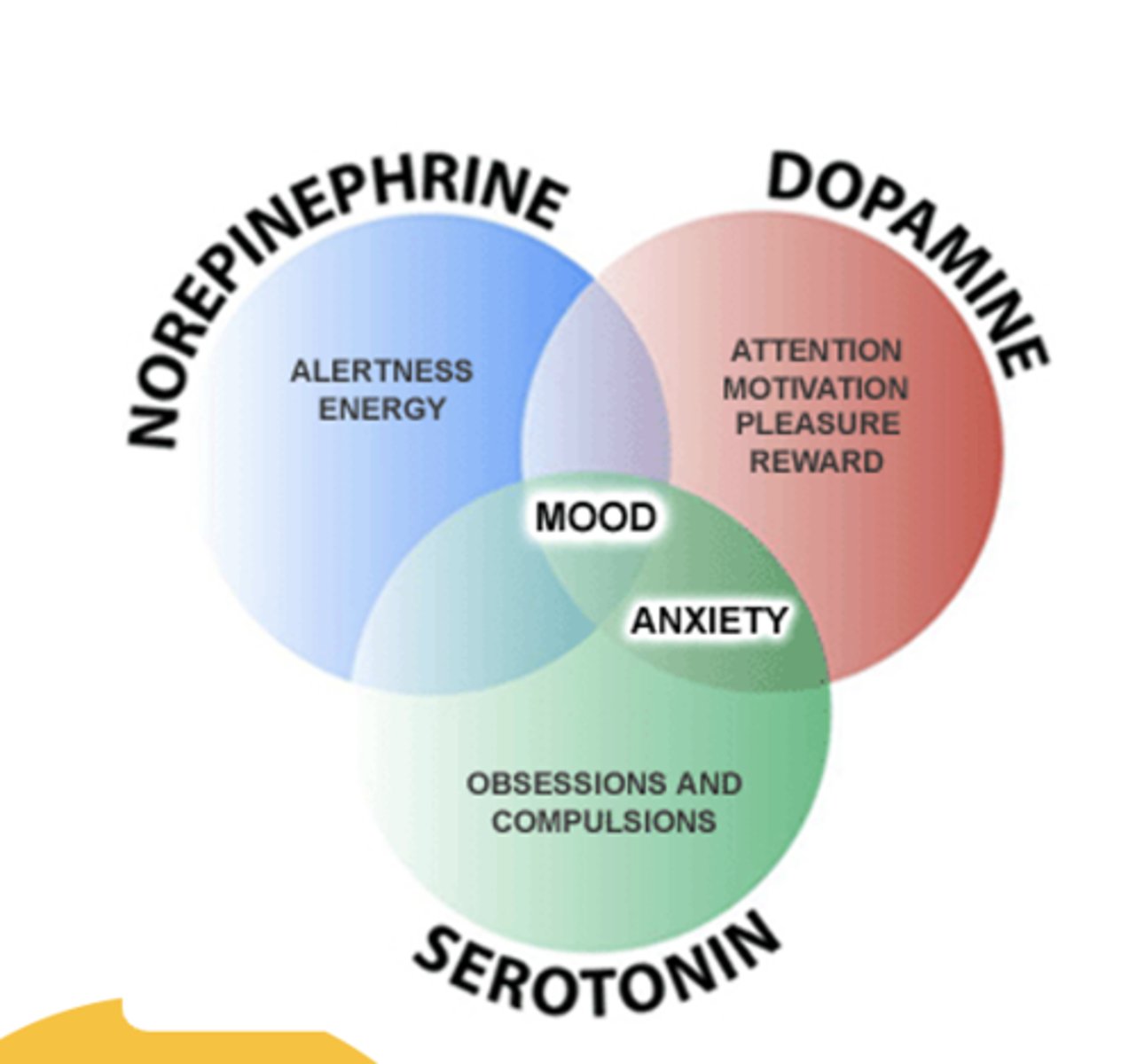
Affective disorders such as DEPRESSION are thought to result from a chemical imbalance between three neurotransmitters – norepinephrine (NE), serotonin (5-HT) and perhaps dopamine (DA). More recent research has also suggested that beta-adrenergic receptors may be involved.
- Orally administered
-- (i.m. administration very infrequent and limited to specific drugs)
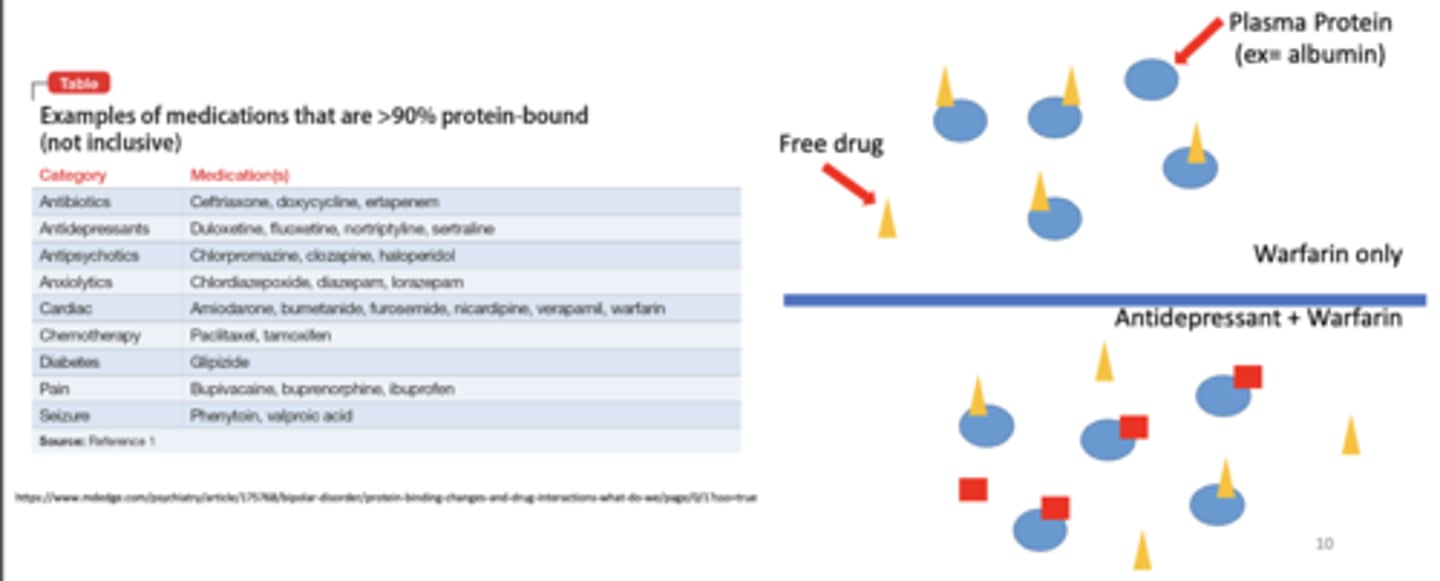
- 90-95% bound to plasma proteins
- Metabolized by the liver, with metabolites excreted in urine
- Drugs with long “half-lives” (e.g., Diazepam - t½=43 hours)
- Drugs with a relatively small therapeutic index
what are some general characteristics of antidepressants
plasma protein binding - just an example
plasma protein binding - just an example
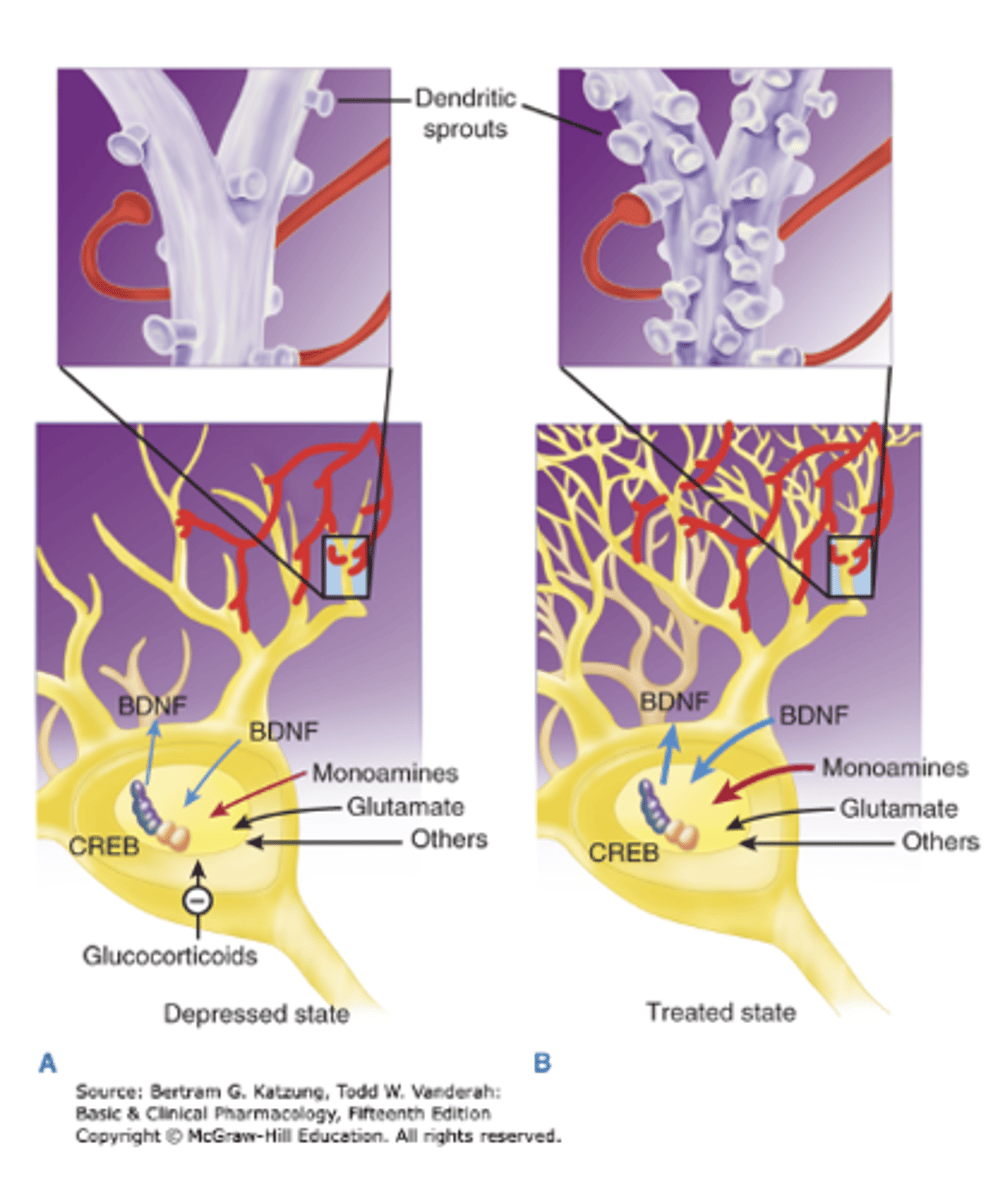
neurotrophic hypothesis
- Depression associated loss of neurotrophic support (ex- brain derived neurotrophic factor) and subsequent structural alterations (decreased dendritic spine density)
-Antidepressanttherapies increaseneurogenesis and synapticconnectivity
- Interesting correlation with proposed alternative therapies
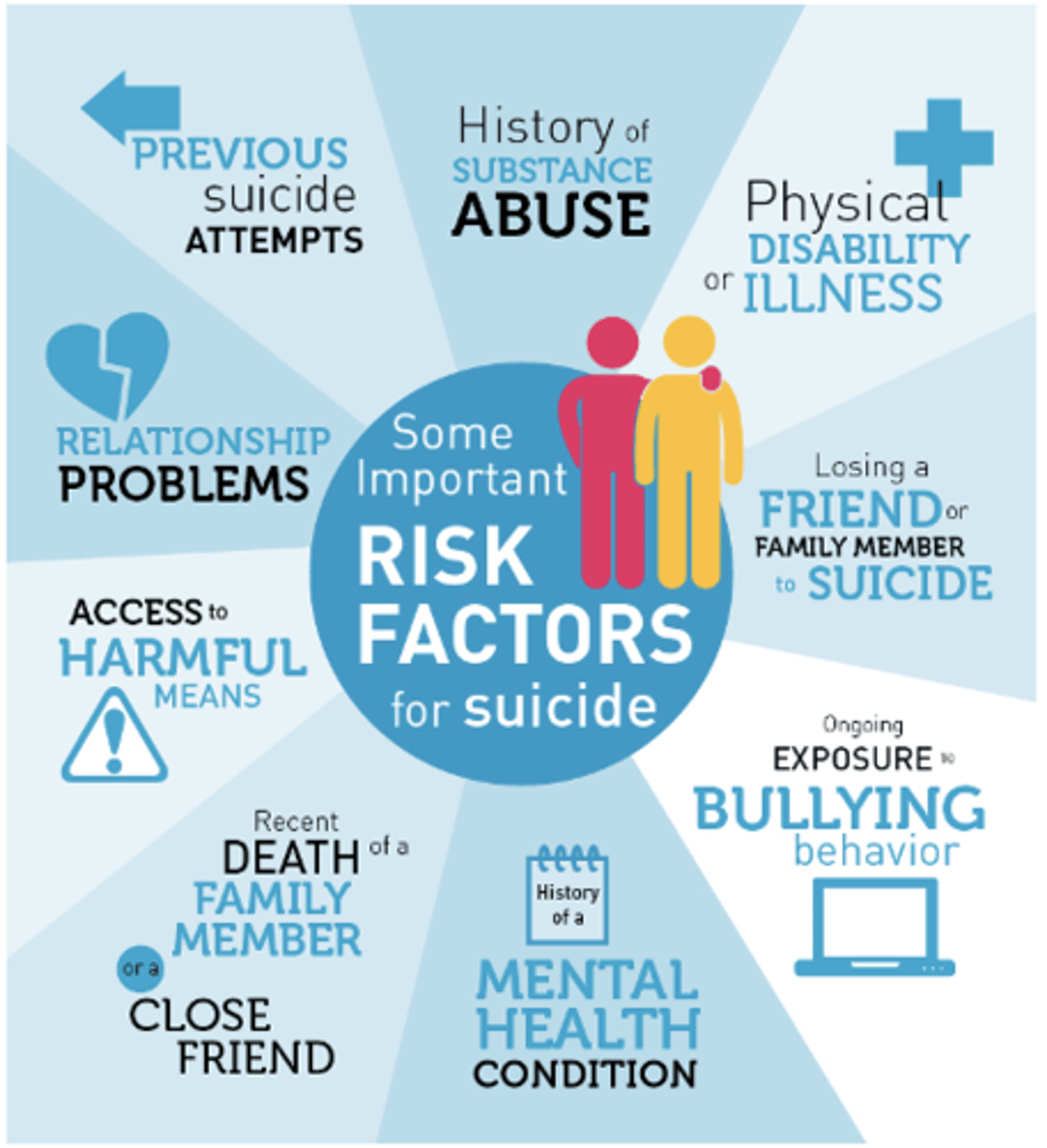
risk factors for suicide
if you have a severely depressed patient, they most likely will not have the energy or drive to commit suicide, however being put on antidepressants may push them over the edge, so make sure to monitor them closely
risk factors for suicide
if you have a severely depressed patient, they most likely will not have the energy or drive to commit suicide, however being put on antidepressants may push them over the edge, so make sure to monitor them closely
1. Tricyclics
2. Selective Serotonin Reuptake Inhibitors (SSRI)
3. Selective Serotonin and Norepinephrine Inhibitors (SNRI)
4. Atypical or Miscellaneous
Monoamine Oxidase Inhibitors (MAOI)
what are the different antidepressant classes
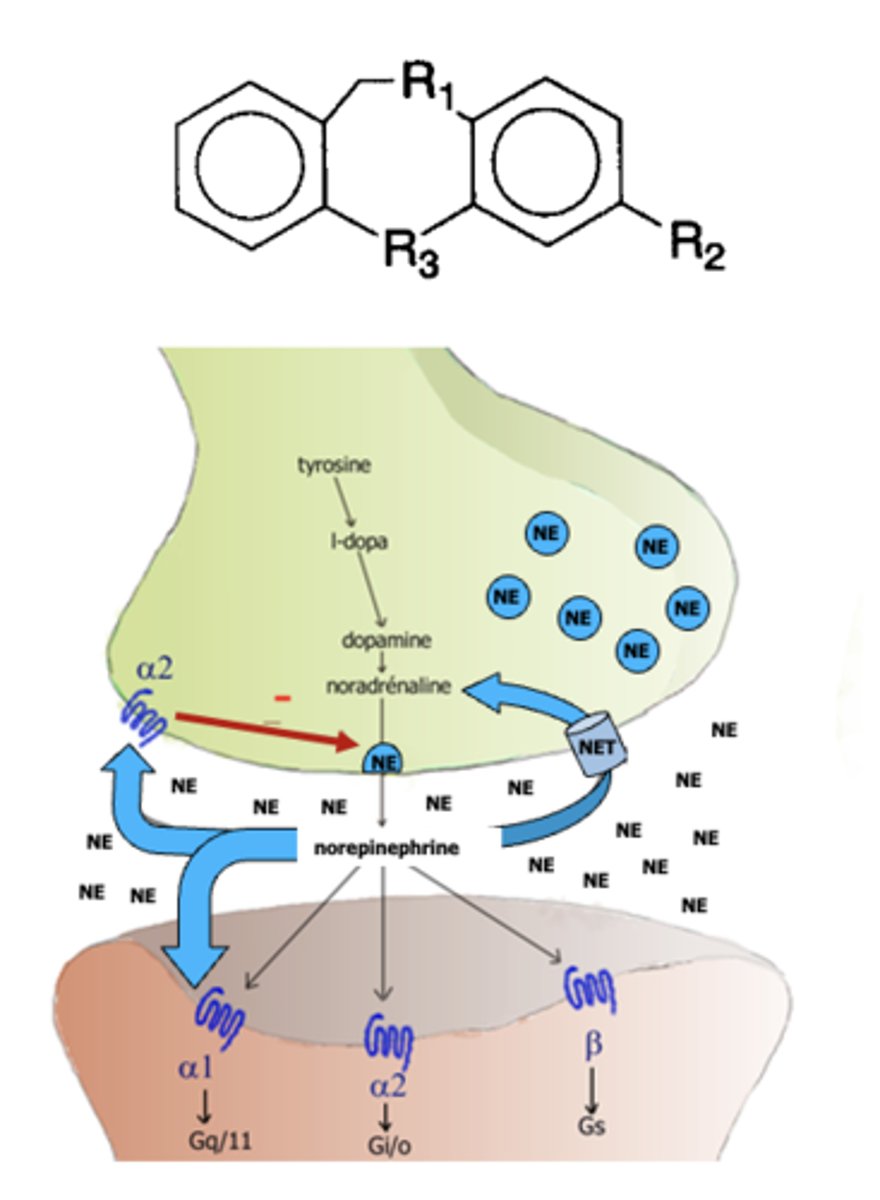
tricyclics
The __________ attempt to remedy depression by inactivating the “amine” pump on the presynaptic nerve terminal and thus limiting the reuptake of both norepinephrine and serotonin. Unfortunately, many also have effects at muscarinic receptors, histamine type-1 receptors and alpha-1 receptors
- Amitryptyline (Elavil)
- Clomipramine (Anafranil)
- Doxepin (Sinequan)
- Imipramine (Tofranil)
- Trimipramine (Surmontil)
what are the different types of tertiary amine tricyclic (NE, 5-HT) antidepressants
- Amoxapine (Asendin)
- Desipramine (Norpram)
- Maprotiline (Ludiomil)
- Nortryptyline (Pamelor)
- Protryptyline (Vivactil)
what are the different types of secondary amine tricyclics (NE)
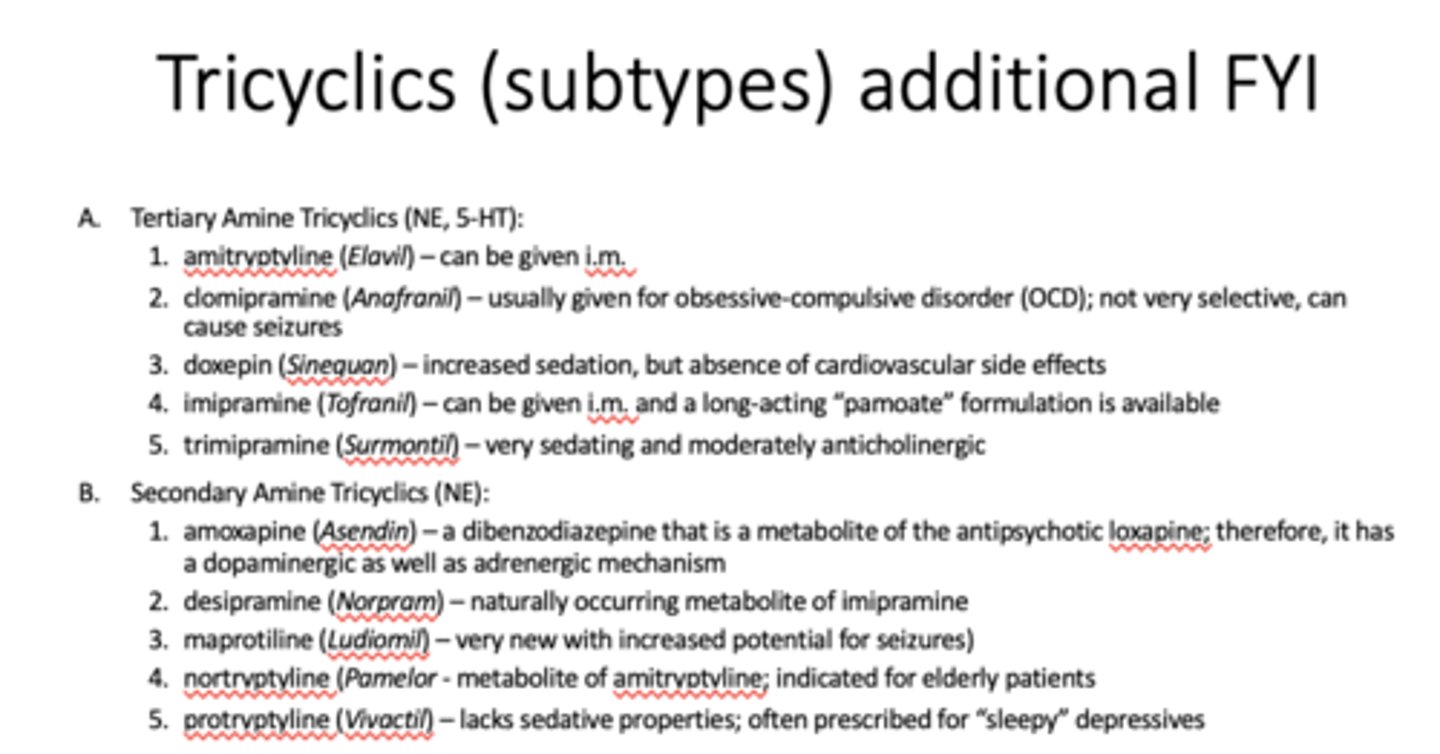
just FYI
just FYI
tricyclics
Mechanism of Action:
- Block reuptake of NE
- Block reuptake of 5-HT (serotonin)
- Block muscarinic receptors
- Block α1 receptors
- Block histamine receptors
- Block fast Na+ channel
RISK OF OVERDOSE
Side Effects:
- Widest variety of side effects due to wide variety of actions (OVERDOSE POSSIBLE)
- Histamine blockage- sedation, weight gain (due to increased hunger)
- α1 blockage- orthostatic hypotension, sedation
- NE/5-HT reuptake blockade- Lower seizure threshold
- Muscarinic receptor antagonist- anti-SLUDE (decreased- salivation, lacrimation, urination, defecation, emesis)
- Na+ channel blockade- Widened QRS complex in heart (possible arrhythmia)
Selective Serotonin Reuptake Inhibitors (SSRI)
Often first choice for monopolar depression and they appear to be the most effective agents in the treatment of premenstrual dysphoric disorder (PMDD).
- Citalopram (Celexa)
- Escitalopram (Lexapro) – approved for adolescents
- Fluoxetine (Prozac)
- Fluvoxamine (Luvox)
- Paroxetine (Paxil)
- Sertraline (Zoloft)
what are the different types of Selective Serotonin Reuptake Inhibitors (SSRI)
Selective Serotonin Reuptake Inhibitors (SSRI)
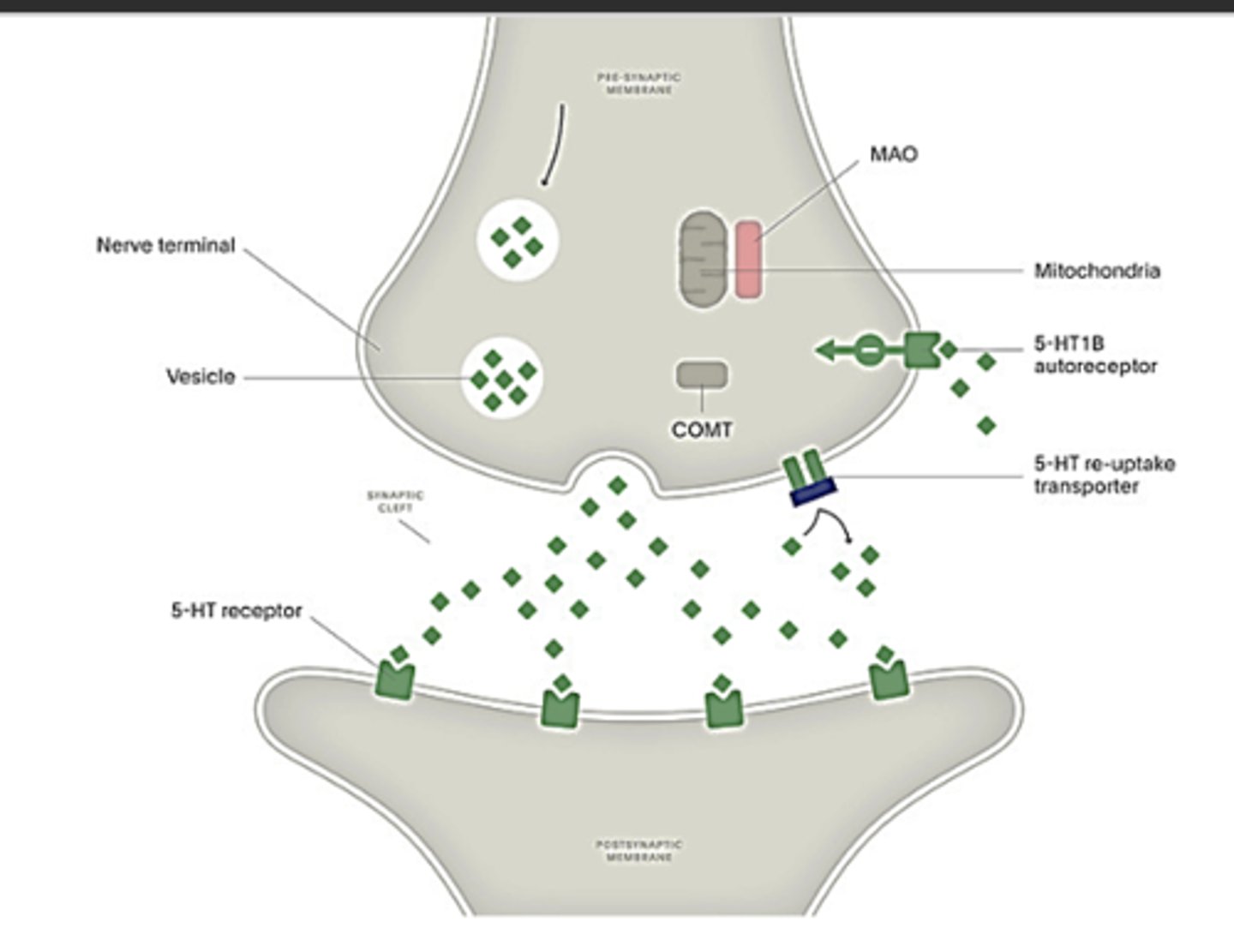
Mechanism of Action:
Inhibits the 5-HT re-uptake transporter to increase the level of serotonin in the synapse
Side Effects (all due to serotonin)
- Excess stimulation of serotonin receptors (brain and spinal cord):
-- Increased anxiety
-- Irritability
-- Decreased libido
-- Sexual side effects (erectile dysfunction, anorgasmia, ejaculatory delay)
-- Mental dullness
Gastrointestinal 5-HT3 receptor stimulation --> nausea, diarrhea, emesis
Withdrawal syndrome
- Dizziness
- Headache
- Nervousness
- Nausea
- insomnia
Study Question: Top reason for non-adherence? due to interaction with serotonin there are adverse effects that cause many patients to discontinue these medications
serotonin syndrome
- Typically begins within 12 hours – 3 days of starting treatment
- Rarely results from use of single serotonergic medication at therapeutic doses
- Can lead to coma and death if untreated
Symptoms:
- hyperthermia, muscle rigidity, myoclonus, tremors, autonomic instability
- confusion, irritability, agitation, hallucinations
- nausea, vomiting, abdominal pain
- seizures
Interventions:
- discontinue serotoninergic medication, supportive care (IV fluids, benzodiazepines/other sedatives, cooling, ventilation)
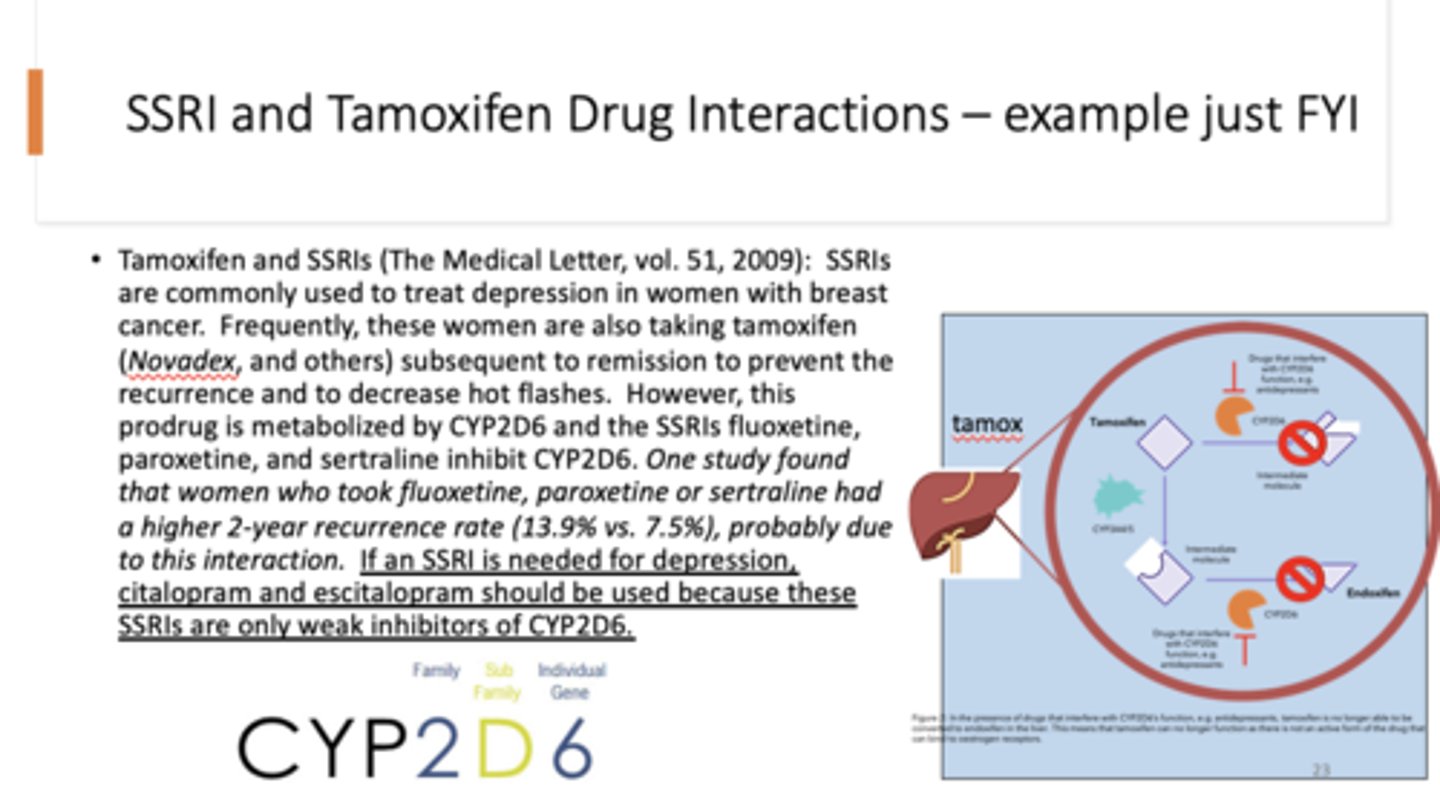
fyi - note breast cancer part, not sure if he will ask it but he said it was interesting
fyi - note breast cancer part, not sure if he will ask it but he said it was interesting
- Venlafaxine (Effexor)
- Desvenlafaxine (Pritiq)
- Duloxetine (Cymbalta) - FDA approved for fibromyalgia
- Milnacipran (Ixel)
- Levomilnacipran (Fetzima) - FDA approved for fibromyalgia
what are the different Serotonin and Norepinephrine Reuptake Inhibitors (SNRI)
allowing more norepinephrine activity at the synapse
allowing more norepinephrine activity at the synapse
- Bupropion (Wellbutrin or Zyban)
- Mirtazapine (Remeron)
- Trazodone (Desyrel) - Used commonly for insomnia
- Nefazodone
- Vilazodone (Viibryd)
- Vortioxetine (Trintellix)
what are the different types of atypical antidepressants
bupropion
Mechanism of Action:
- Inhibits Norepinephrine reuptake transporter
- Inhibits Dopamine reuptake transporter
- Mechanism of action may involve some NE and DA release
Treats:
MDD, Seasonal Affective Disorder, ADHD, Tobacco Dependence, Hypoactive Sexual Disorder, Obesity
Side Effects
- 3 FOLD increase in the incidence of seizures
- Increased sexual desire
- Reduced Appetite
- Dry mouth
- Nausea
- insomnia
- anxiety

Mirtazapine
Mechanism of Action:
- Antagonist to presynaptic α2 receptors and postsynaptic 5-HT2 and 5-HT3 receptors
- Leads to increase serotonin and NE release and 5-HT1 receptor activation
- Also H1 receptor antagonist, muscarinic receptor antagonist, α1 receptor antagonist, enhanced dopamine release
Treats:
MDD, GAD, tension headaches (off label use for insomnia)
Side Effects
- Usual serotonin side effects with less sexual side effects
- Sedation
- Increased Appetite

trazodone
Mechanism of Action:
- Antagonist to 5-HT2 receptors and serotonin reuptake inhibitor
- Effects on serotonin are dose dependent
- H1 receptor antagonist
- Alpha 1 receptor antagonist
Treats:
MDD and insomnia
Side Effects
- Typical serotonin side effects
- Drowsiness - H1
- Sedation - H1
- Orthostatic Hypotension - A1
Priapism (call your doctor for an erection lasting more than 4 hours) - A1
- Cardiac Arrhythmias
wont test on this one
wont test on this one
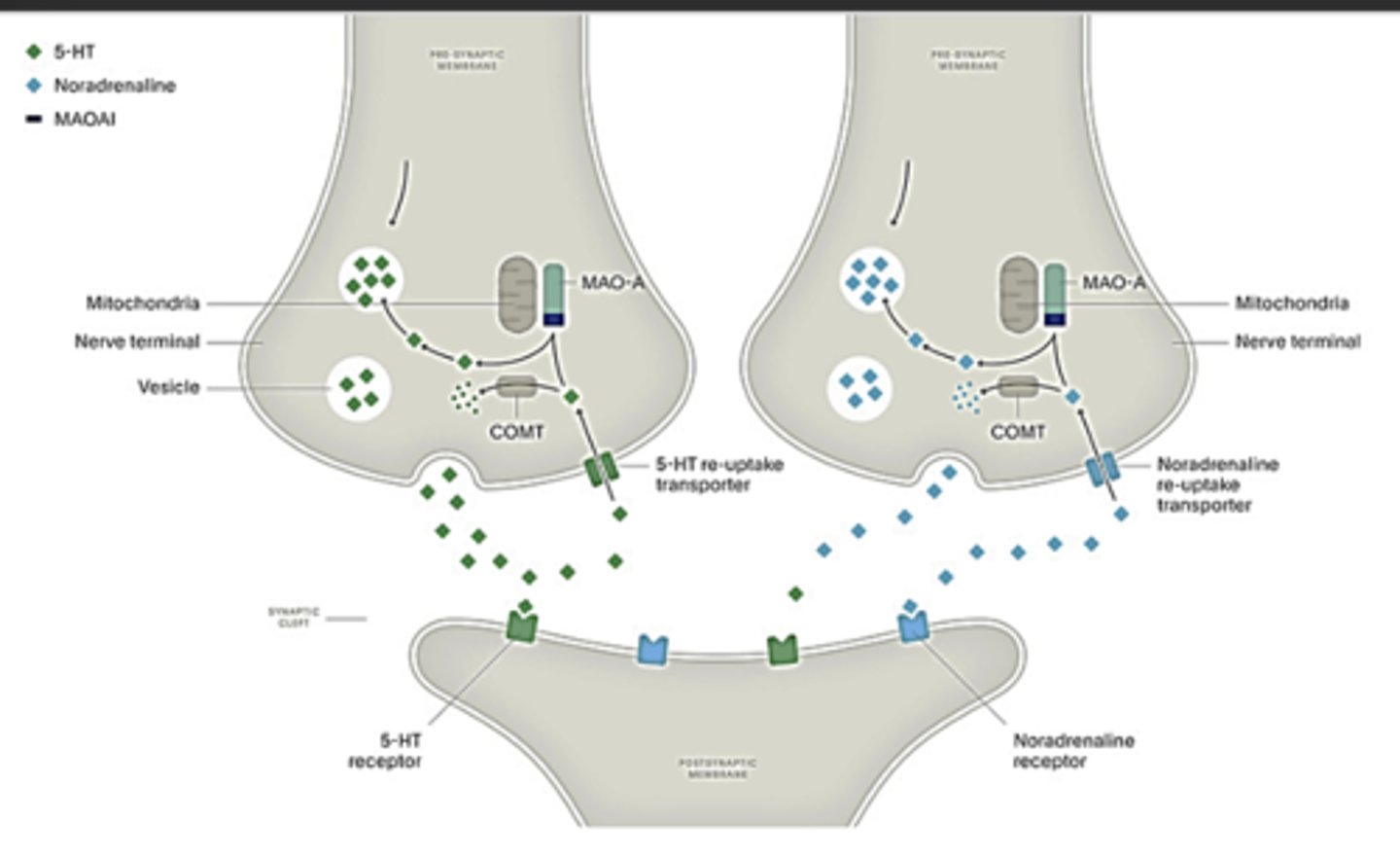
Monoamine Oxidase Inhibitors (MAOI's)
Used mostly for treatment-resistant depression or "refractory" depression; these drugs inactivate the enzyme that metabolizes norepinephrine and serotonin (monoamine oxidase, MAO).
1. isocarboxazid (Marplan)
2. phenelzine (Nardil)
3. tranylcypromine (Parnate)
what are the different Monoamine Oxidase Inhibitors (MAOI's)
isocarboxazid (Marplan)
Mechanism of Action:
- Inhibits monoamine oxidase which metabolizes monoamines: norepinephrine, dopamine, and serotonin
- Used mostly for treatment-resistant depression* or “refractory” depression; these drugs inactivate the enzyme that metabolizes norepinephrine and serotonin (monoamine oxidase, MAO).
*Treatment-resistant depression means you have tried at least two other antidepressants for at least 6 weeks each and have not experienced remission or at least a 50% improvement in mood.
Side Effects
- Risk of hypertensive crisis and serotonin syndrome
- Hypotensive- dizziness (big risk if elderly)- central alpha 2
agonist)
- Serotonin-related side effects (sexual, GI, etc)
- Suppress REM sleep (clinical significance unknown)
- Tremors, excitement, convulsions (Dopamine)
antidepressant half life
- Most antidepressants have a long half life (for example - 30 hours)
- It takes 4-5 half lives to reach therapeutic levels in the blood, meaning it can take a week for an antidepressant to get to therapeutic levels
- It can take 4-5 weeks before it effects mood in a positive way
Antidepressants
should not be given with other CNS depressants, any antimuscarinic agent, or a MAO inhibitor. That said, these combinations are typically observed/prescribed
a.indirect-acting sympathomimetics:
1) amphetamine
2) tyramine (dietary sources of tyramine are particularly a problem)
3) Of particular importance is the potential for local anesthetic solutions containing epinephrine to cause hypertensive crises in patients receiving TCAs and MAOIs.
b. mixed-acting sympathomimetics (often found OTC):
•pseudoephedrine
Interactions with various sympathomimetic agents can be very problematic, such as:
General Adverse effects of antidepressants
sedation either by increasing serotonin or by blocking histamine type-1 (H1) receptors.
General Adverse effects of antidepressants
- cardiovascular effects are some of the most serious side effects.
-- orthostatic hypotension can lead to tachycardia
-- antimuscarinic effects at the sinoatrial node can unmask sympathetic influences
- seizures - many antidepressants lower the seizure threshold
- sexual dysfunction – a very troubling adverse effect for patients, which can lead to non-compliance.
- blood abnormalities - although agranulocytosis is rare, these drugs can cause bone marrow depression, thrombocytopenia or eosinophilia. In addition, elderly people may be at greater risk for low salt (sodium) levels in the blood. Symptoms may include headache; weakness or feeling unsteady; confusion, problems concentrating or thinking or memory problems.
General Adverse effects of antidepressants
- abnormal bleeding - antidepressant medicines may increase your risk of bleeding or bruising, especially if you take the blood thinner warfarin (Coumadin®, Jantoven®), a non-steroidal anti-inflammatory drug (NSAID), or aspirin.
- Serotonin Syndrome - agitation, hallucinations, coma or other changes in mental status; coordination problems or muscle twitching; fast heartbeat, high or low blood pressure; sweating or fever; nausea, vomiting or diarrhea; muscle stiffness or tightness.
- manic episodes - greatly increased energy; severe trouble sleeping; racing thoughts; reckless behavior; unusually grand ideas; excessive happiness or irritability; talking more or faster than usual.
- Suicidality and Antidepressant DrugsAntidepressants increased the risk of suicidal thinking and behavior (suicidality) in children, teens, and young adults compared to placebo. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients of all ages who are started on antidepressant therapy should be monitored appropriately and observed closely for clinical worsening, suicidality, or unusual changes in behavior.
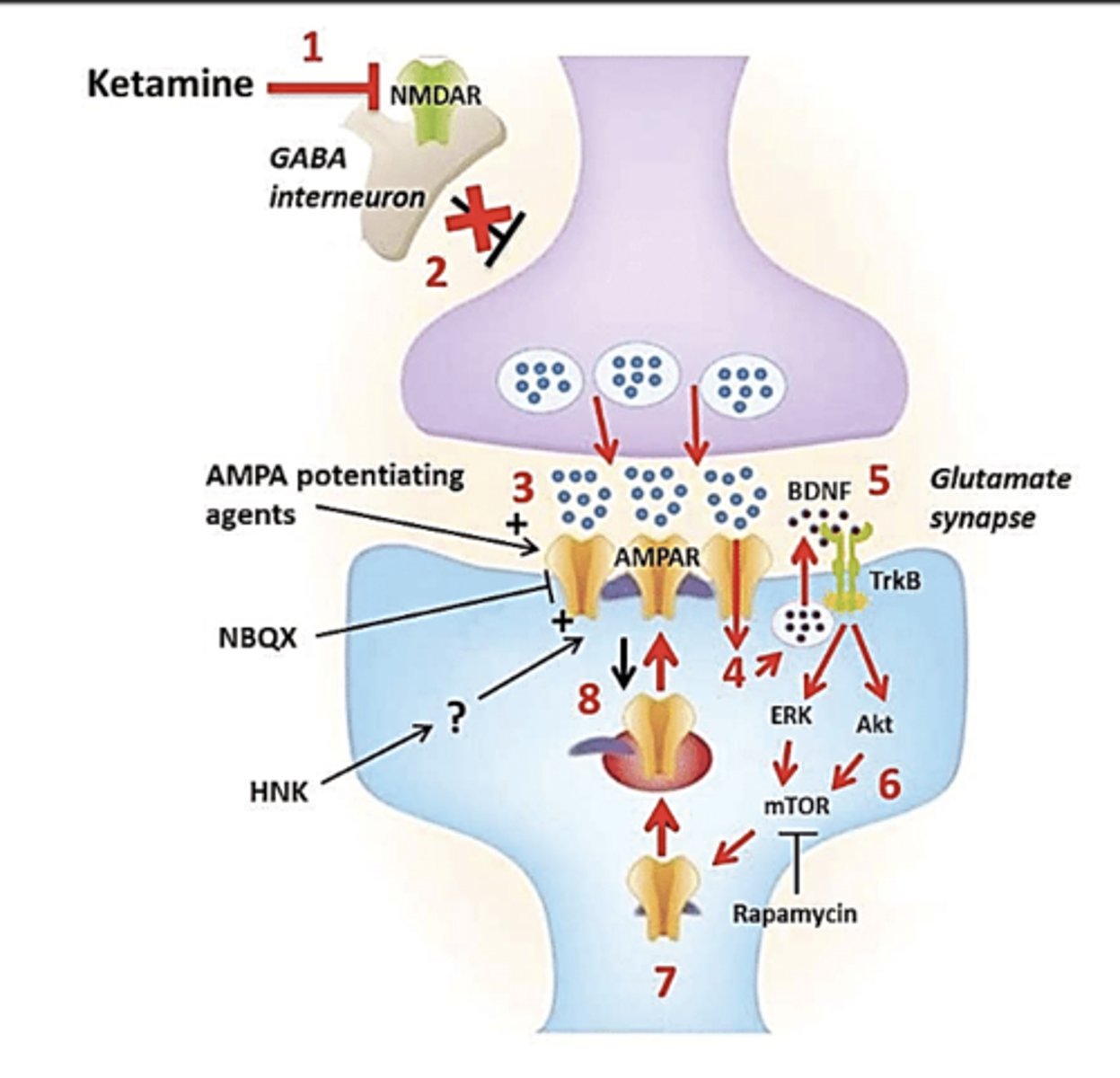
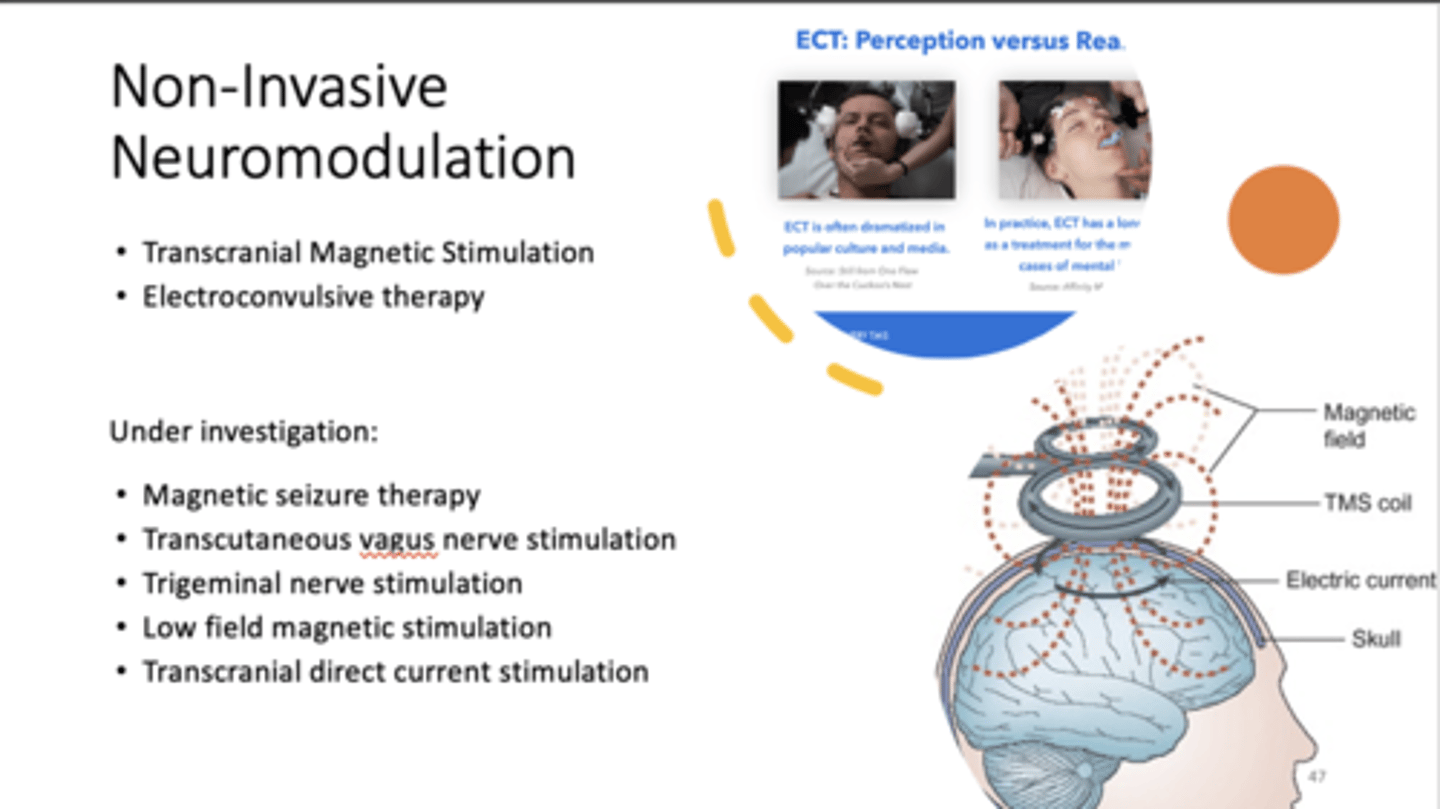
esketamine (spravato)
In 2019, the FDA approved _____________ nasal spray in conjunction with an oral antidepressant for people with treatment-resistant depression.
an isomer of the dissociative anesthetic ketamine. Suicidal ideation may decrease after administration of ____________. Adverse effects are similar to those for ketamine.
esketamine (spravato)
New treatment option for treatment-resistant MDD (two previous failed treatment attempts and less than 50% symptom reduction)
Increases levels of glutamate and can lead to relief of depressive symptoms within hours
Induces rapid synaptogenesis
Must be administered through a nasal spray in a clinic due to the potential for side effects
--Hallucination and dissociation
Derived from the anesthetic, Ketamine, this drug must be used with a traditional antidepressant medication
psilocybin
- Serotonergic, psychedelic drug derived from psilocybe cubensis
- psilocybin + Psychotherapy proved effective for unipolar treatment resistant depression
- Increased remission rates and efficacy comparable to escitalopram over a 6-week study
- Increased dendritic spine formation and dendritic spine density
- Depression relief confirmed a year post treatment (Hopkins study)
- Appears in the majority of clinical trials to cure, not treat, depression
"wont talk much about because it freaks him out"
"wont talk much about because it freaks him out"
CBT + Pharmacotherapy
better than CBT on its own or pharmacotherapy on its own both short and long term.
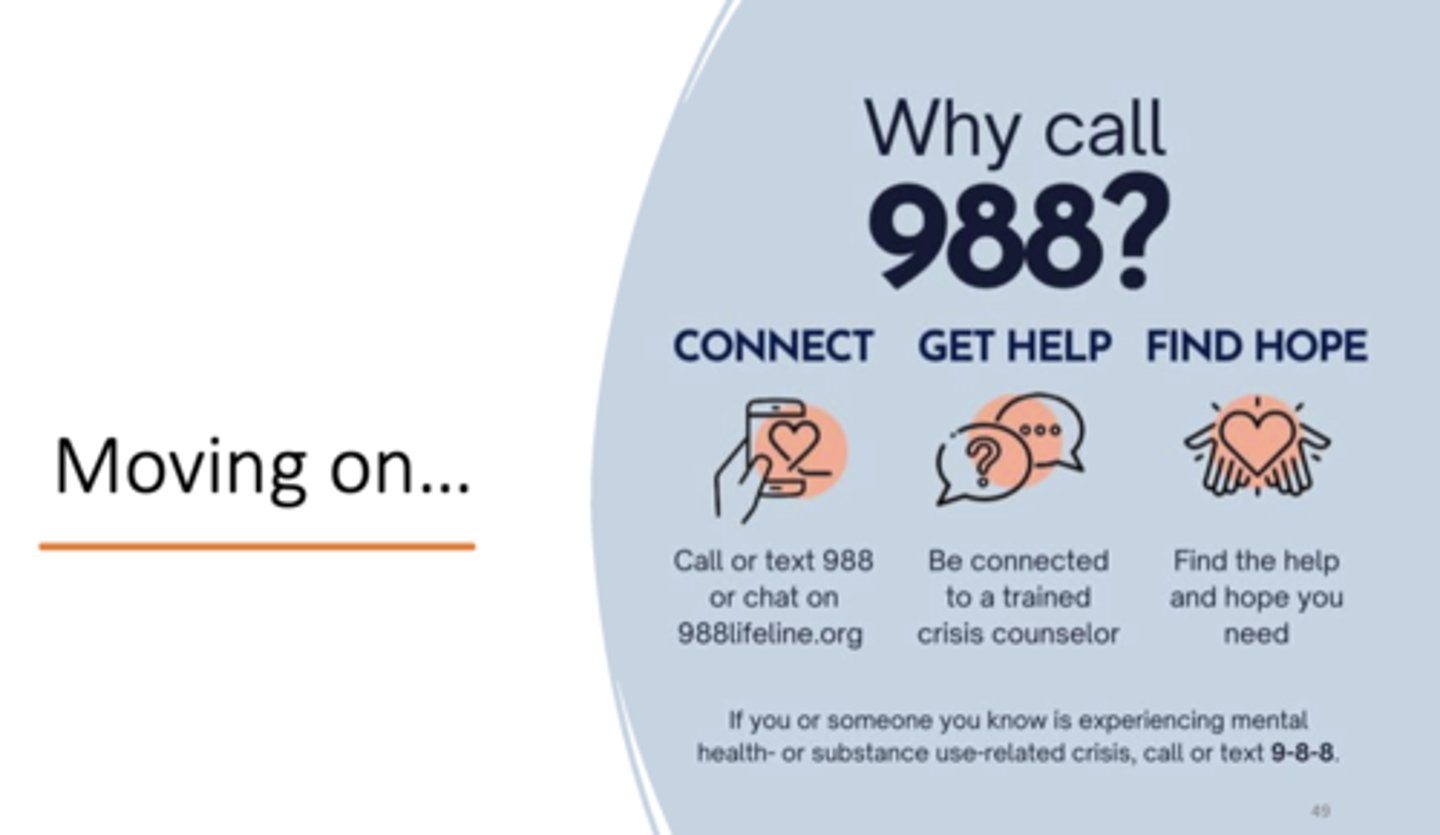
why call 988? - suicidal hotline
why call 988? - suicidal hotline
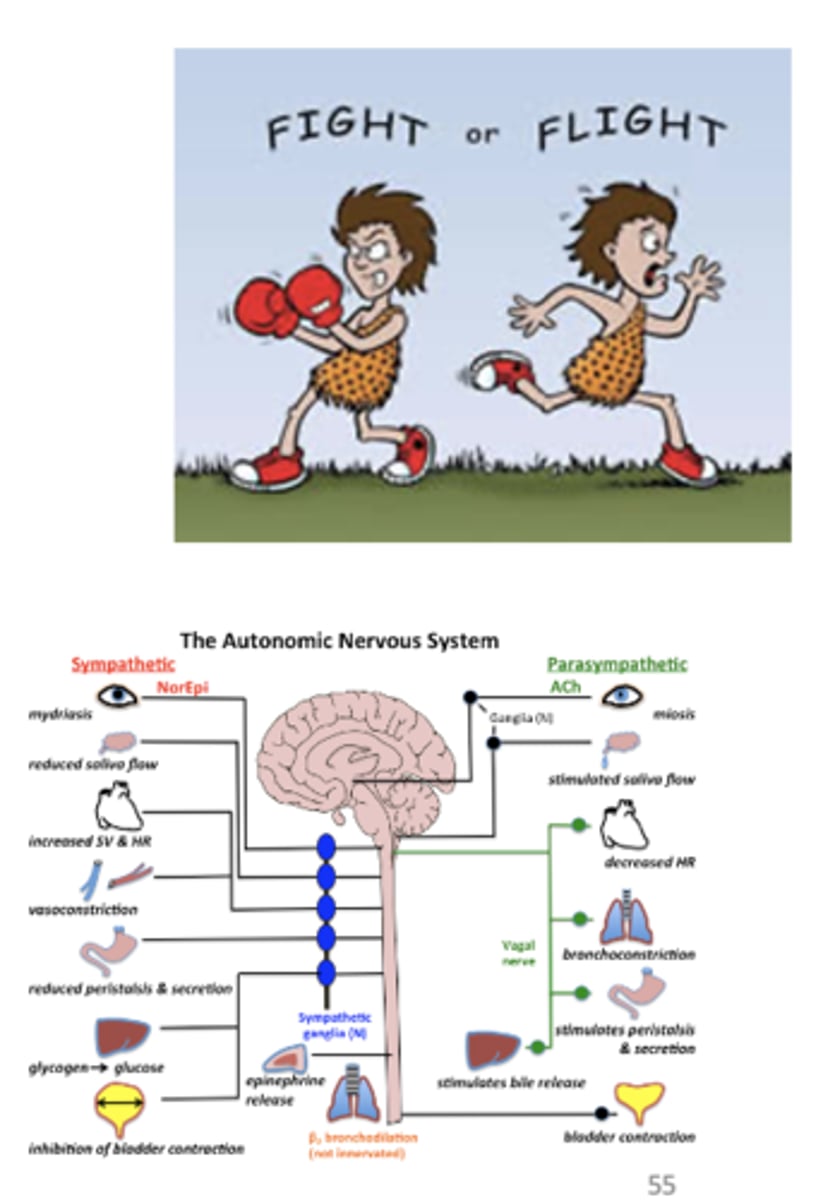
Anxiolytics
are medications used to treat anxiety disorders. They work by calming the nervous system and reducing feelings of fear, worry, and tension.

anxiety
"Unpleasurable state of tension which indicates the presence of something dangerous to the organism."
Learned response, acquired from personal experience or secondary through the experience of others
Physiologic reaction
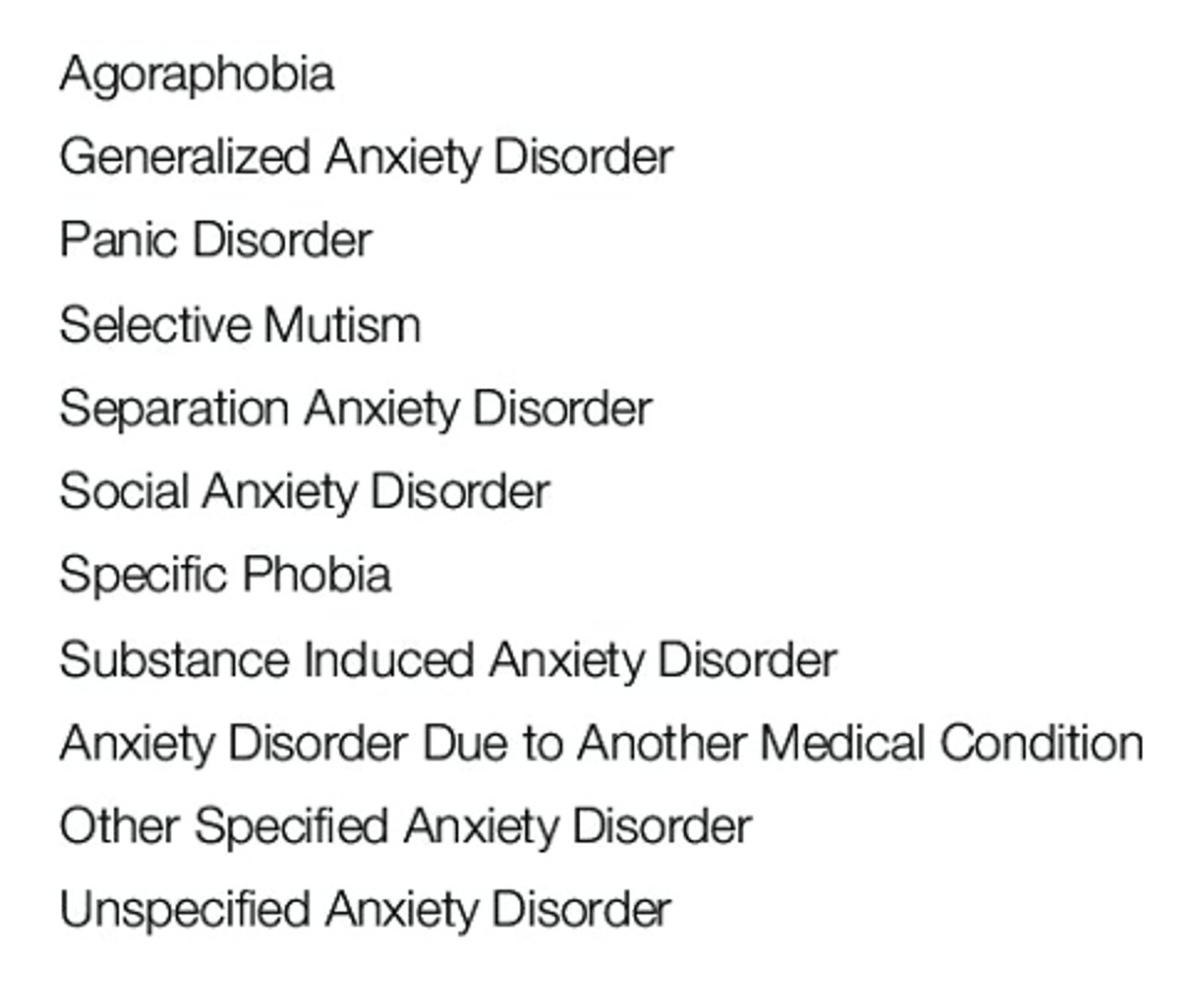
DSM-5 List of Anxiety Disorders
DSM-5 List of Anxiety Disorders
Generalized Anxiety Disorder (GAD) Symptoms
Generalized Anxiety Disorder (GAD) Symptoms

- Tension, restlessness
- Increase blood pressure and heart rate
- Excessive sweating
- Dyspnea (shortness of breath)
what are some physiological effects of anxiety
Beta- Adrenergic Antagonists
Propranolol
Nadolol
- Used for performance anxiety (fear of public speaking)
- Helpful for tachycardia and tremor
- Side effects: hypotension, GI symptoms, sexual dysfunction, poor circulation
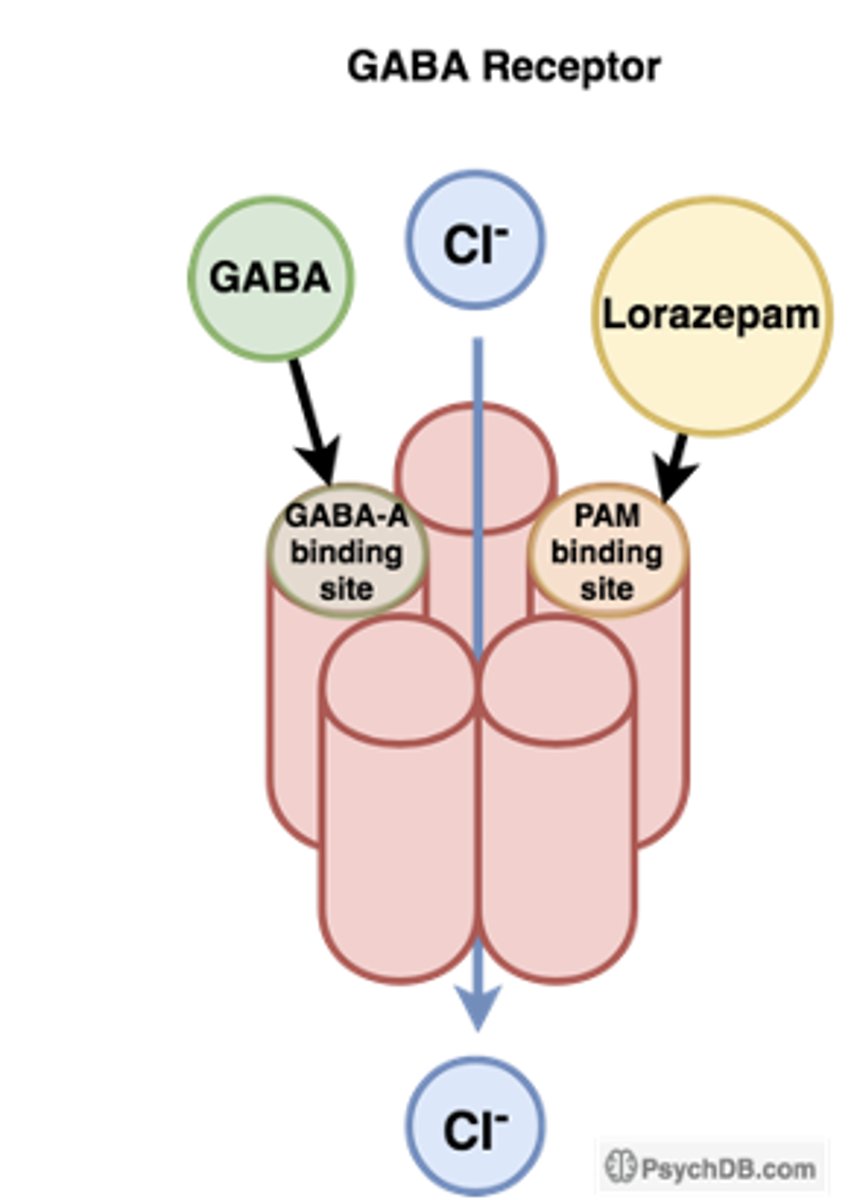
Benzodiazepines
Alprazolam (Xanax)
Lorazepam (Ativan)
Clonazepam (Klonopin)
Diazepam (Valium)
- Situational anxiety, generalized anxiety disorder, panic disorder
- Side effects: impaired psychomotor performance, amnesia, dependence, withdrawal, rebound anxiety
Enhance receptor affinity for GABA, so GABA binds more frequently.
Allosteric modulation
what is the MOA of acute anti anxiety agents
- anxiety
- insomnia
- anticonvulsant
- muscle relaxant
- acute psychosis
- post-ventilator anxiety
- alcohol withdrawal
- off label: bipolar disorder
what are some benzodiazepine usages
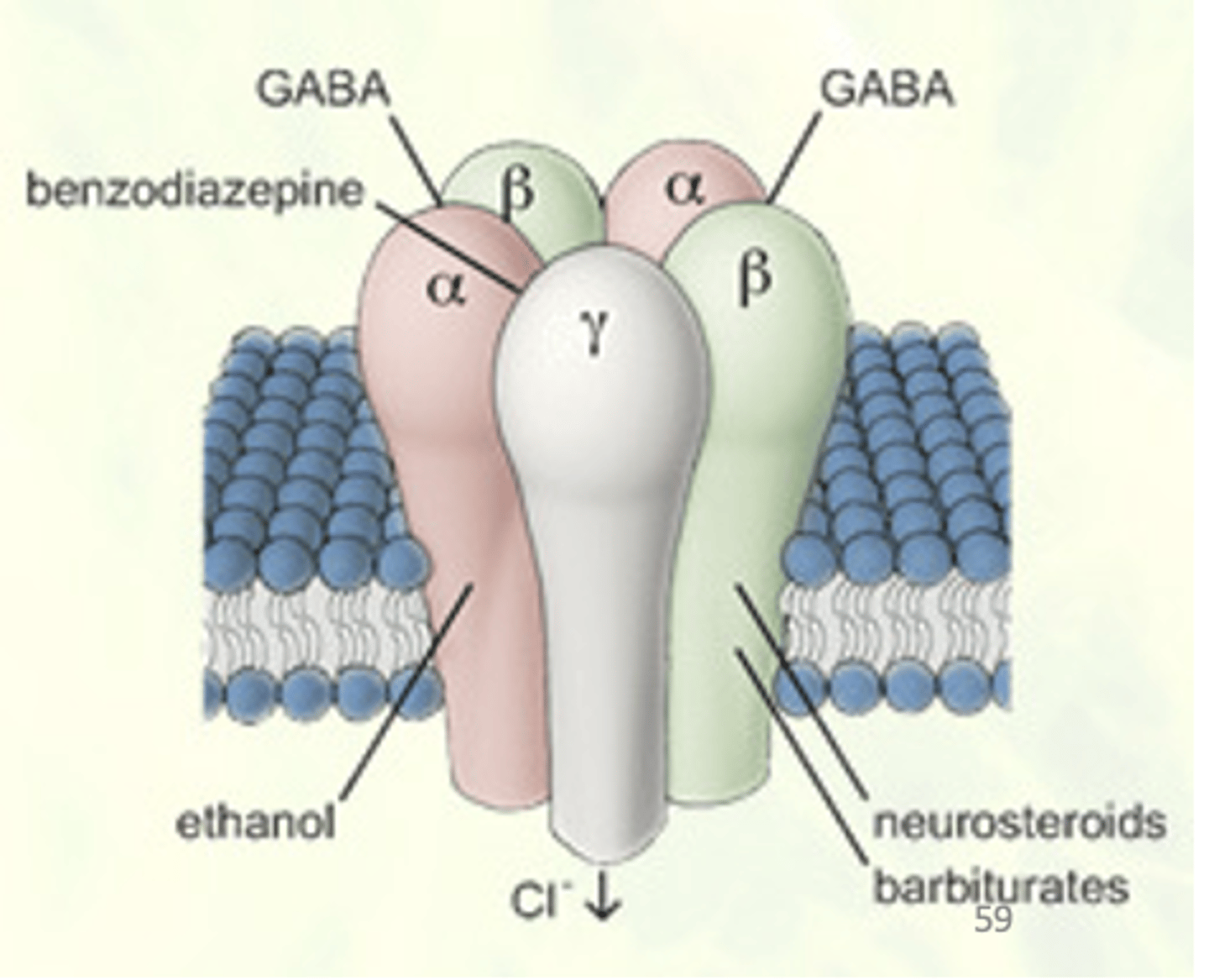
benzo mechanism of action
- These drugs are predominantly positive allosteric modulators of the GABAA receptor complex – i.e., they have a binding site on the GABA receptor complex.
- Produce marked psychological and physical dependence, with a life-threatening withdrawal. One of the most difficult drug dependencies to discontinue. Huge problem
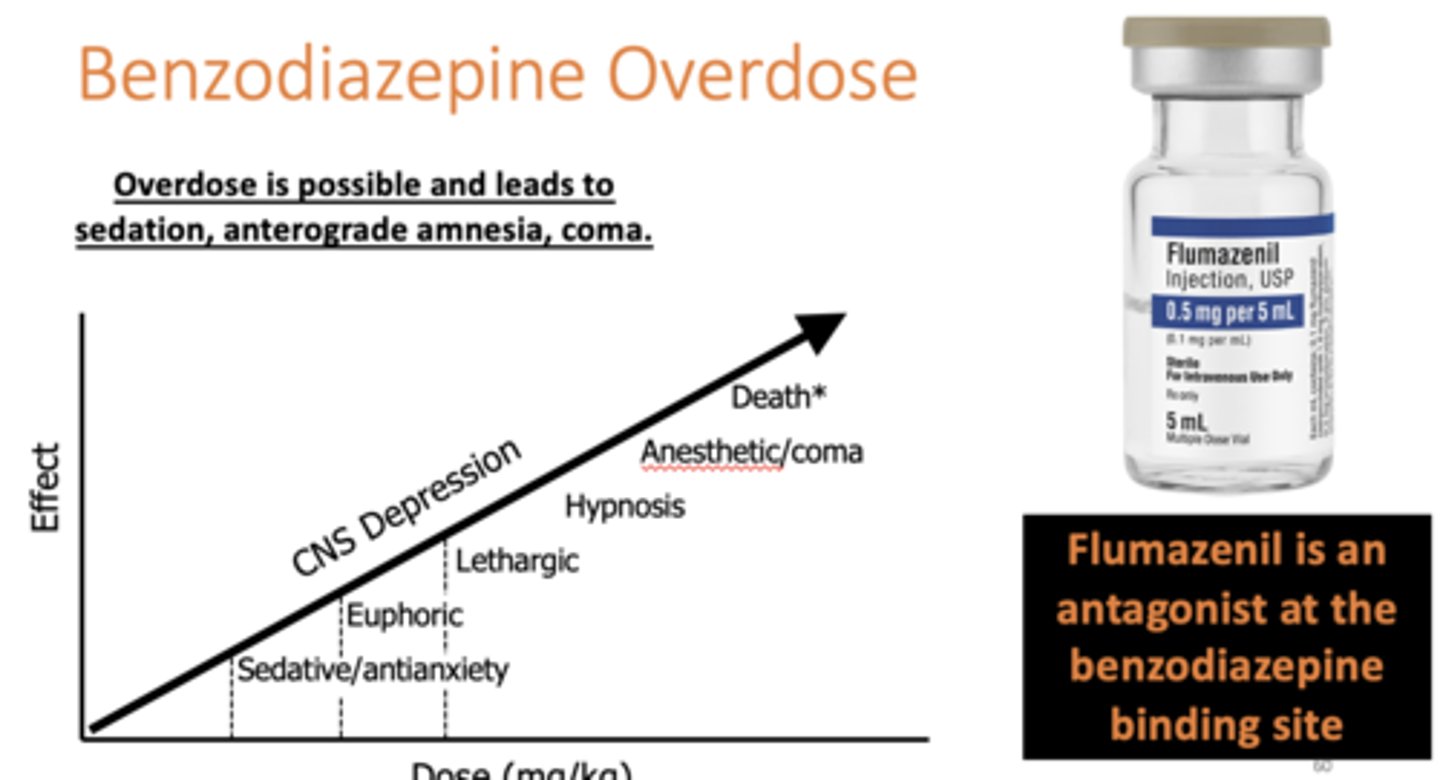
Flumazenil
an antagonist at the benzodiazepine binding site
Benzodiazepine Overdose
Benzodiazepine Overdose
fyi
fyi
SSRIs and SNRIs
Doses used are similar to doses used to treat depression - chronic anxiety
Buspirone (Buspar)
5-HT1A agonist (used for Generalized Anxiety Disorder) - chronic anxiety
Trazodone
Nefazodone
Mirtazapine
what are some other antidepressants for chronic anxiety
Alprazolam
Lorazepam
Clonazepam
Diazepam
what are the benzodiazepines for chronic anxiety
grounding technique
grounding technique
