ch 15: psychedelic and hallucinogenic drugs
1/48
Earn XP
Description and Tags
502-524
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
what are the hallucinogens (2) + their classifications? (3)
drugs that distort perceptions of reality at relatively low doses
most are schedule III → although most are safe + non-addictive
psychedelics
deliriants
dissociatives
deliriants vs dissociatives? (2)
deliriants: result in mental confusion + inability to differentiate reality from fantasy
dissociatives: cause analgesia, amnesia, catalepsy, and a sense of detachment from environment
psychedelics produce __(4)__ without producing __(1)__ → types (2) + examples (6)
produce vivid sensory experiences, altered perceptions, cognitive distortions, altered awareness
do not produce a state of toxic delirium
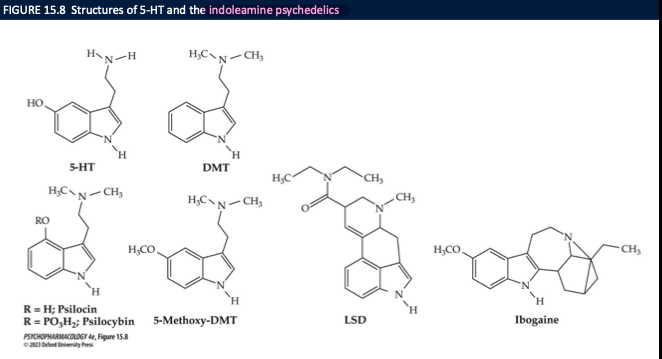
indoleamines: structurally similar to 5-HT
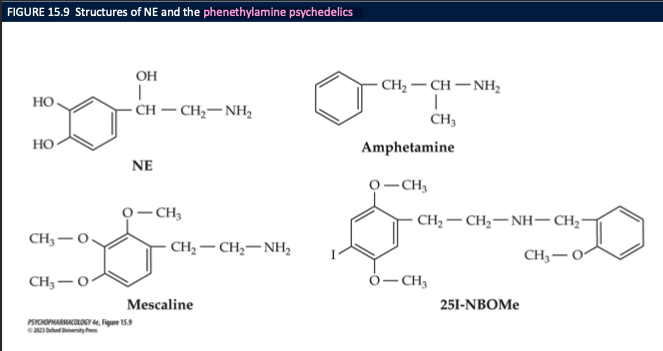
phenylethylamines: structurally similar to DA + NE
LSD, mescaline, psilocybin, bufotenine, DMT, 5-MeO-DMT
hallucination vs illusion (2)
hallucination: sense perception for which there is no external stimulus
illusion: altered + distorted perceptions, thoughts, feelings, insights, awareness
mescaline
derived from dried top of the peyote cactus
psilocybin (3)
alkaloid from several mushroom species
dried + eaten or made into tea
converted into psilocin after ingestion → psychoactive agent
where are DMT, 5-MeO-DMT and 5-HO-DMT found, how are they consumed and synthetic analogs? (3)
found in plants indigenous to South America and frog venom
smoked or snorted → produce brief but intense hallucinatory experience
synthetic analogs; alpha-methyl tryptamine (AMT), foxy methoxy
ayahuasca (4)
hallucinogenic drink made by natives from the Amazon from 2 plants
contains DMT
the other supplies alkaloids ß-carbolines which inhibit MAO activity
used in spiritual/religious ceremonies
Lysergic acid diethylamide (LSD) (3)
synthesized from fungal alkaloids on rye
CIA carried on unethical experiments w LSD
Charles Manson
how have some researchers tried using LSD as a tool in psychotherapy or psychoanalysis (2)
psycholytic therapy: drug-induced psychosis meaning psychic loosening or opening
psychedelic therapy: patient was given a high dose of LSD in hopes of gaining insight into his/her problems
NBOMes (3)
appeared in 2010s → continue to be widely distributed
subject to first-pass metabolism when consumed orally → taken sublingual or buccal routes
v. potent → cases of toxicity have severe even fatal consequences
salvinorin A (3)
psychoactive ingredient in Salvia divinorum → inactivated in the GI tract
leaves can be chewed or extracts made
absorbed through the mouth or smoked
ibogaine low vs high dose (4)
derived from bark and roots of a west African shrub → chewed or made into a powder
can help counteract opioid withdrawal symptoms + cravings
low doses: psychostimulant → ↑ energy, ↓hunger, produce euphoric feeling
high doses: produce psychedelic effect
PCP and Ketamine (2) + routes of administration (4)
ketamine: short-acting anesthetic
may have potential to treat depression
ingested, snorted, smoked, injected
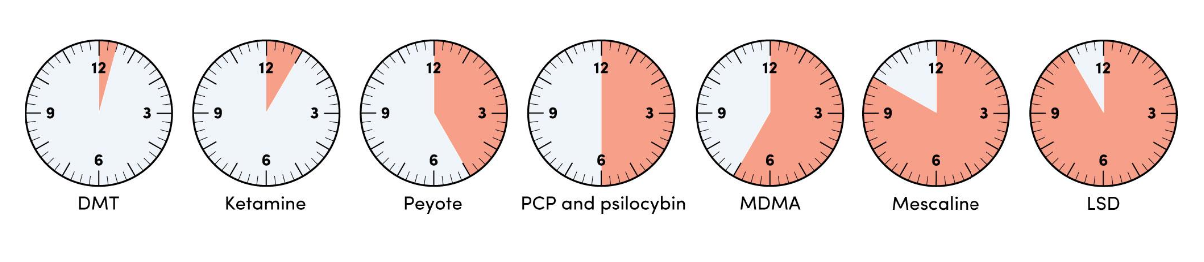
hallucinogens are taken ____ and typically take effect in ____ → onset of action faster when __(3)__. duration of action depends on factors like __(3)__ → they are metabolized by ___ and excreted in ____
orally
20-60 minutes
snorted, smoked, or given IV
dosage, purity, drug taken ie. DMT= 30 mins, LSD = 1 hr
liver
urine
3 stages of an LSD trip (3)
sympathomimetic physiological effects
alterations in perceptions + sensations → synesthesia
self-perceptions change → leading to distortions of space and time, cognitive ∆s and emotional swings
bad LSD trips are characterized by (3)
frightening hallucinations, confusion, disorientation, agitation, depression, terror, intense anxiety or panic, paranoia
can leave long-lasting psychological scars
can exacerbate a pre-existing psychiatric illness or affective disorder
other acute effects of LSD (2)
flashbacks: visual disturbances that occur long after the drug has left the body
high therapeutic index → no evidence of organ damage
psilocybin vs mescaline trip (4)
psylocybin
less emotionally intense → more visual and euphoric → fewer panic rxns
risk of OD is v low
mescaline trip
gradual onset → fewer ∆s in mood + sense of self
more toxic + more side effects
salvia (1) vs PCP (3) vs ketamine (1) trips
salvia: vivid visual imagery, sensory disturbances, time distortions
PCP:
variable effects depending on dose, environment, characteristics of the user
stimulant, depressant, analgesic, hallucinogenic, anaesthetic
high doses can cause convulsions, rep failure, coma, death
ketamine
effects similar to PCP but shorter duration + fewer hallucinations
LSD trip can be divided in 4 phases ____, plateau, ___, and comedown. phase 1 occurs ___ after LSD ingestion
onset
peak
30 minutes to an hour
onset phase of LSD trip (3)
visual effects
intensification of colors
appearance of geometric patterns or strange objects that can be seen with one’s eyes closed
plateau phase of LSD trip (3)
2 hrs
sense of time slowing
visual effects become more intense
peak phase of LSD trip (4)
begins after 3 hrs → lasts 2-3
user feels in another world + time stopped
sees bizarre distorted images that can be beautiful or menacing
experiences synesthesia: colours are heard, sounds are felt
comedown phase of LSD trip (4)
2 hrs or longer
most drug effects gone
user may still not feel completely normal
feelings of depersonalization, emotional shifts from euphoria to anxiety, fearful state, disruption of logical thought
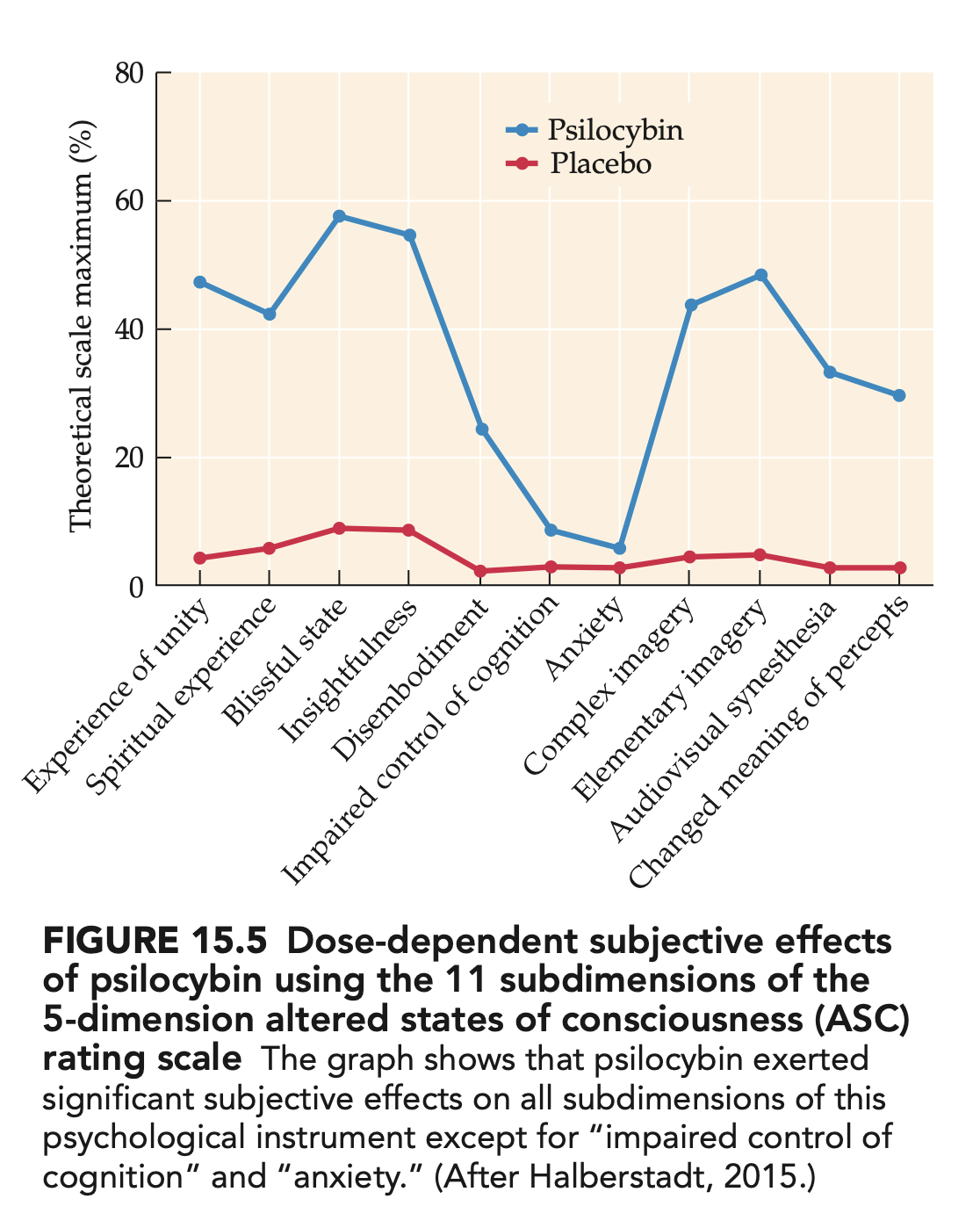
altered states of conciousness (ASC) rating scale dimensions (5)
developed to quantify the effects of hallucinogens
oceanic boundlessness: feeling one w the world
ego-disintegration anxiety: negative emotional responses bc of loss of ego boundaries
visionary restructuralization: distortions of visual perceptions
reduced vigilance: less important measure
auditory alterations: auditory hallucination
physiological responses to hallucinogens reflect ______ (3)
activation of the sympathetic NS
dizziness
nausea
vomiting
hallucinogenic drugs with serotonin-like molecular structure (7) (indolamine)
LSD
psilocybin
psilocin
DMT
5-MeO-DMT
synthetic tryptamines
ibogaine
hallucinogenic drugs with catecholamine-like molecular structure (3)
mescaline
NBOMs
amphetamine analogs DOM/TMA
known as phenethylamine psychedelics
What is the main receptor target of classic psychedelic hallucinogens, and what evidence shows it’s necessary for their effects? (3)
Indoleamine and phenethylamine psychedelics (e.g., LSD, psilocybin, mescaline) are 5-HT₂A receptor agonists.
5-HT₂A knockout mice or humans pre-treated with the 5-HT₂A antagonist ketanserin show little to no psychedelic response,
and brain imaging shows that neocortical 5-HT₂A receptor occupancy strongly correlates with subjective trip intensity.
What is the head-twitch response and how is it used in psychedelic drug research? (3)
The head-twitch response is a rapid, repetitive side-to-side head jerk seen in rodents after 5-HT₂A agonist psychedelics.
It increases dose-dependently
is used as an animal behavioral measure of psychedelic effect strength (more drug → more head-twitches).
What happens to the default mode network (DMN) during a psychedelic trip?
DMN activity goes down, meaning less self-focused, ruminative “ego” activity.
How do psychedelics change sensory processing in the brain?
They reduce thalamic gating and increase cortical sensory processing, so more raw sensory info gets through and feels more intense.
In psychedelic therapy, what is meant by the “peak experience” and “afterglow”?
The peak experience is the most intense part of the trip (desired in therapy); the afterglow is a period of days–weeks after where mood and insight are improved.
What is the best predictor of a good therapeutic response to psychedelics?
The intensity of the psychedelic experience (how strong the trip feels to the person).
What neuroplasticity effect is thought to underlie psychedelics’ antidepressant actions?
Rapid glutamate-dependent plasticity: increased synapse growth and connectivity (more dendritic spines/synapses) in key brain regions.
Historically, what disorder was LSD explored to treat before it became Schedule I?
Alcohol dependence.
Are classic 5-HT psychedelics strongly addictive?
No. They are not strongly dependence-forming for most users, though a few heavy users can develop hallucinogen use disorder.
Why do classic psychedelics show rapid tolerance?
Repeated use causes down-regulation of 5-HT₂A receptors, so the same dose has less effect.
Name two serious long-term adverse effects of classic psychedelics.
Flashbacks and HPPD (hallucinogen persisting perception disorder) with ongoing visual disturbances.
What type of drugs are PCP and ketamine, and what is their receptor action?
They are dissociative anesthetics and act as uncompetitive antagonists at the NMDA glutamate receptor (block the channel from inside).
What kind of subjective state do anesthetic doses of ketamine/PCP produce?
A dissociated state (e.g., “K-hole”) with out-of-body feelings, time loss, and strong distortions of body and space.
How does NMDA blockade by PCP/ketamine affect cortical glutamate?
Blocking NMDA receptors on GABA interneurons reduces inhibition and increases cortical glutamate release.
How do PCP and ketamine support the glutamate hypothesis of schizophrenia?
High doses of PCP/ketamine block NMDA receptors and produce schizophrenia-like symptoms (disordered thought, delusions, motor and negative symptoms),
suggesting NMDA hypofunction can contribute to schizophrenia.
Do PCP and ketamine have reinforcing (rewarding) effects? How do we know?
Yes. Rodents and primates self-administer them, and they increase DA firing and release in reward areas (NAcc, dorsal striatum, PFC), producing dose-dependent “drug liking” in humans.
What’s the typical subjective effect of low vs high ketamine doses?
Low dose: relaxed, mild dissociation (“going to K-land”).
High dose: strong dissociation/altered state similar to LSD; many users avoid this intensity.
Name two clinical uses of ketamine.
Rapid relief of depression (before SSRIs work)
non-opioid analgesia for acute or chronic pain.
What are some long-term problems from chronic PCP/ketamine use? (4)
Memory and cognitive deficits, psychosis-like symptoms, and urinary tract/bladder damage (can lead to renal issues).
How addictive are classic psychedelics compared with PCP/ketamine?
Psilocybin, LSD, mescaline → low abuse potential, not considered addictive; rapid, reversible tolerance and cross-tolerance.
PCP/ketamine → some potential for dependence and more toxic chronic effects.