immuno exam 2
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
List the important surface markers that distinguish T + B cells. Describe their fxn
T cells
T cell receptor (TCR) = Ag receptor
all T cells have 1 of 2 types: αβ (alpha beta) and γδ (gamma delta)
CD3 = signal transduction molecule complexed w/ TCR to help transduce signal when Ag binds
pan T cell marker = on all T cells
CD4 = binds constant region MHC 2
αβ marker
CD8 = binds constant region MHC 1
αβ marker
B cells
BCR = surface Ig w/ transmembrane region
CD20 + CD19 = regulatory fxn in B cell dev/differentiation
pan B cell marker = on all B cells
important for K9 lymphoma immunotherapy
What is immunophenotyping? What is the flow cytometry method for this w/ an example of immunophenotyping a bovine blood sample for CD8 + CD4 T cells? Other clinical applications?
immunophenotyping = lab techniques to ID + classify B and T cells
flow cytometry method = Ab to surf. marker specific to cell of interest tagged w/ fluorescent dye → allows us to ID + classify B and T cells
ex) immunophenotyping a bovine blood sample for T cells
1) rabbit anti-bovine CD8+ Ab tagged w/ blue fluorescent dye + rabbit anti-bovine CD4+ Ab tagged w/ red fluorescent dye
2) both added to sample of isolated lymphocytes → incubate → wash out unbound Ab → flow cytometer counts cells that fluoresce
cells that fluoresce blue → are CD8+ T cells
cells that fluoresce red → are CD4+ T cells
other clinical apps of flow cytometry:
det. type of lymphocyte causing lymphoma in dogs
evaluate vaccine efficacy in inducing T cell-mediated immunity + what kind of T cells are stimulated
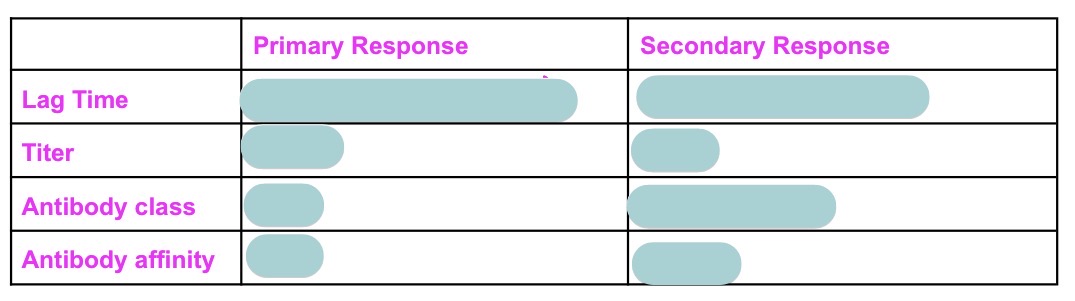
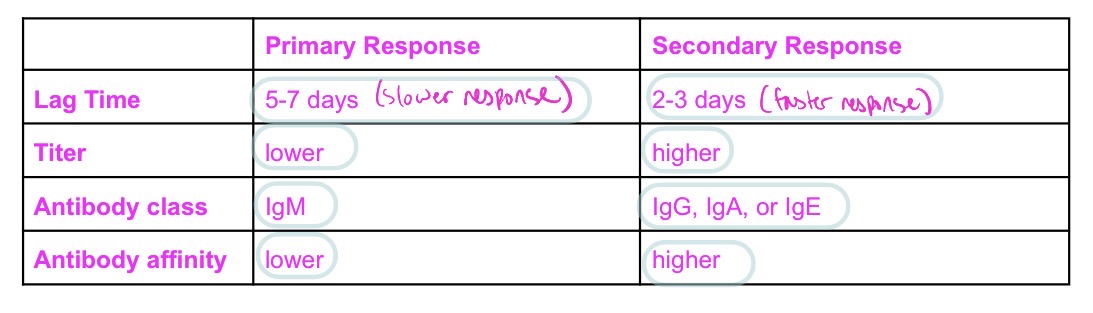
Compare + contrast primary vs secondary Ab response + why different using response to virus/bac as an example for each
primary Ab response to virus/bac:
virus/bac invade body → ends up in LN → meets lymphocytes that recognize it → lymphocytes become stimulated → clonal expansion
virus/bac has many epitopes → each epitope stim. a diff. clone of T/B cell → induce polyclonal response
some B cells turn into plasma cells → secrete IgM
some B cells undergo mitosis → get help from T cell cytokines to rearrange DNA + class-switch → differentiate into plasma cells that secrete diff. Ig isotype w/ same antigen specificity but diff. effector fxn
some of those clones become memory B cells of that new isotype
the plasma cells die or continue as long-lived plasma cells
w/o further Ag stim. → Ab conc. decreases
secondary Ab response to virus/bac:
virus/bac invade body → ends up in LN → meets lymphocytes that recognize it → activates lymphocytes
same B cell clones that recognized Ag during primary response turn into plasma cells → secrete IgM
B cell clones prod. during primary response (class-switched memory B cells + long-lived plasma cells) activate → memory B cells differentiate into effector (plasma) cells → plasma cells secrete IgG, IgA, and/or IgE
secondary response diff. bc Ag-specific B cell clones have alr. undergone mitosis → clonal expansion → maturation → thus Ab prod. at most efficient class + highest affinity + higher in titer than primary response
CD4+ + CD8+ T cells also have undergone mitosis → clonal expansion → maturation → more cells that can recog. that Ag
Why is lymphocyte clonal expansion important for immunity?
clonal expansion = mitosis of a lymphocyte → basis for immunologic memory
creates lots of clones specific to an Ag
naive lymphocyte meets its Ag for 1st time → undergo clonal expansion to make many clones specific to that Ag that differentiate into either:
effector cells = activated differentiated lymphocytes that directly carry out immune responses
ex) B cell effector cell = plasma cells that secrete a specific Ab
memory cells = clones that have the same Ag specificity that lie dormant until presented w/ Ag again → then quickly become effector cells
Describe polyclonal activation as it occurs naturally in the body
polyclonal activation = when Ag stim. many diff. lymphocytes that target many diff. epitopes to clone themselves to create a large population of diff. lymphocytes that all target diff. epitopes on that specific Ag
What makes a hybridoma + why do we make them?
hybridoma = hybrid cell prod. by fusion of an Ab-producing B cell + myeloma cell (plasma cells tumor)
B cell → provides blueprint for printing machine for a specific Ab
myeloma cell → immortal printing machine
allows us to make large quantities of monoclonal Ab = identical Ab that recognize same epitope on the same Ag
Polyclonal vs monoclonal Ab?
polyclonal Ab = mixture of diff. Ab prod. by diff. B cell clones of an animal that all recognize the same Ag but diff. epitopes
monoclonal Ab = Ab derived from 1 cell that clonally expanded and prod. Ab that recognize same Ag + same epitope
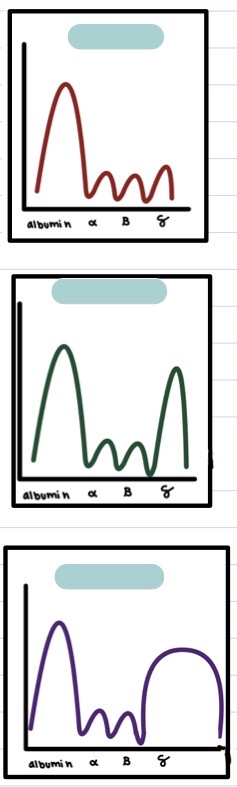
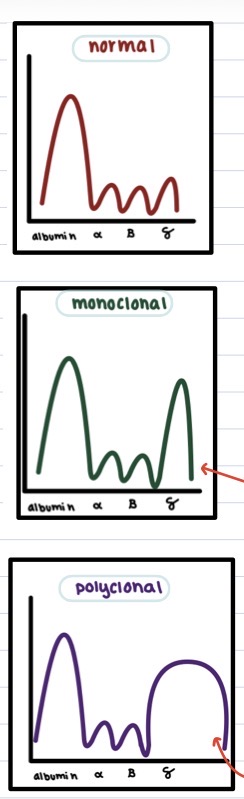
Normal vs monoclonal vs polyclonal gammopathy in a printout of serum electrophoresis + why?
normal:
large albumin peak
all other peaks tgt look small/flat/plateau-shaped
monoclonal gammopathy:
large albumin peak
tall, narrow, gamma globulin peak
indicative of cancer (esp lymphoma) bc many of 1 specific Ab present usually d/t tumor cell overproducing that Ab
polyclonal gammopathy:
large albumin peak
tall, wide, gamma globulin peak
indicative of chronic infection bc many diff. Ab present d/t persistent Ag presentation + B cell activation
How do naive vs memory lymphocytes enter lymphoid tissue from the bloodstream?
naive lymphocytes → via high endothelial venules
bloodstream → high endothelial venules → secondary lymphoid tissue → efferent lymphatic vessels → thoracic duct → bloodstream
mature lymphocytes → via afferent lymphatic vessels
bloodstream → site of infxn in peripheral tissues → afferent lymphatic vessels → secondary lymphoid tissue → efferent lymphatic vessels → thoracic duct → bloodstream
both naive + mature lymphocytes leave secondary lymphoid tissue via efferent lymphatics → thoracic duct → bloodstream
Describe high endothelial venules, fxn, surface molecules, and location
special venules b/t blood + all secondary lymphoid tissues except spleen
have addressins (adhesion molecules) that allow naive lymphocytes to enter secondary lymphoid tissues from bloodstream
How does lymphoid tissue structure help lymphocyte meet Ag?
circulating Ag is picked up → taken to locations of concentrated lymphocytes (aka lymphoid tissues) → much more efficient than lymphocytes needing to circulate to find their 1 specific Ag
3 professional Ag-presenting cells (specifically MHC 2)?
1) dendritic cells = presents Ag on MHC 2 to NAIVE + memory CD4 T cell
2) B cells = presents Ag on MHC 2 to MEMORY CD4 T cell
3) macrophage = presents Ag on MHC 2 to MEMORY CD4 T cell
only professional APCs have MHC 2
only CD4 T helper cells can recognize Ag that is bound to MHC 2
only dendritic cells can present to naive CD4 T helper cells
Immature vs mature dendritic cells?
immature dendritic cells → capture Ag
many Fc + C3b receptors for capturing Ag
do not migrate; must first capture Ag → then mature + migrate to T cells
mature dendritic cells → present Ag to T cells
many costimulatory molecules + MHC 2 + T cell attracting cytokines for presenting Ag
able to migrate, found in T cell rich area of lymphoid tissue
What is a Langerhans cell? Where is it found?
Langerhans cell = immature dendritic cell in epidermis
picks up Ag in epidermis → matures → travels to T cell rich area of regional LN → present Ag to naive/memory CD4 T helper cells
How + where are B cells activated in the LN/spleen?
B cell zone = follicles in LN where B cells hang out
in LN, B cells bind intact, unprocessed Ag via BCR thru either
free Ag
Ag being held onto by follicular dendritic cells
follicular dendritic cells live in B cell zone of LN + hold onto intact Ag for B cells
diff. from regular dendritic cells who are pro APCs for T cells
What are the 3 signals a naive T cell needs from a dendritic cell to begin mounting a response?
1) TCR + CD8/CD4 must bind MHC1/MHC2 + Ag peptide complex
2) costimulatory molecules on DC binding to T cell
3) cytokines binding to receptors
in response, T cells will activate → clonal expansion → mature + differentiate
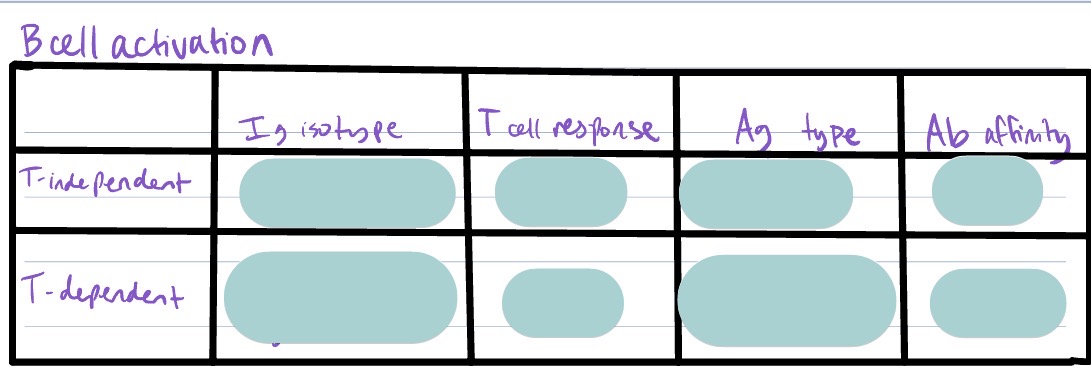
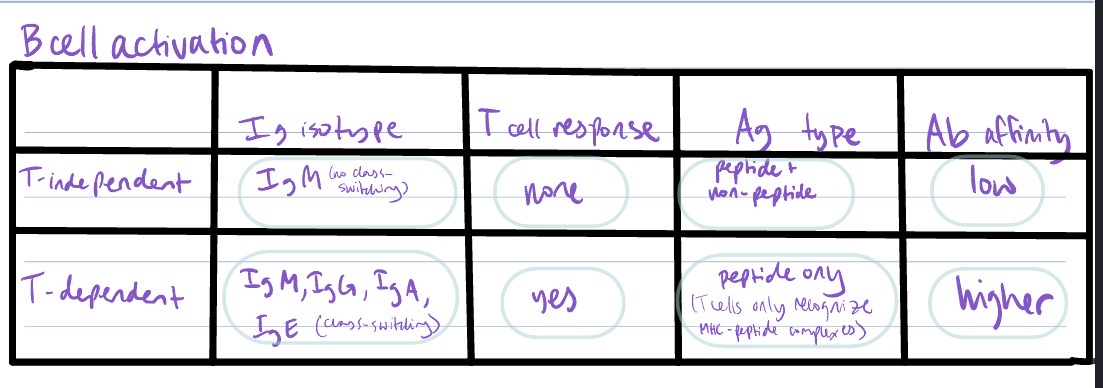
Difference in humoral response for a T-independent B cell response vs T-dependent B cell response?
T-independent B cell activation
low affinity Ab
secretion of only IgM
no class-switching
short-lived plasma cells
Ag can be non-peptide
T-dependent B cell activation → T cells secreting cytokines that stim. B cell
proliferation
differentiation → memory B cells + plasma cells
class-switching
higher affinity Ab
Ag must be peptide bc T cells only recognize MHC-peptide complexes
4 different types of lymphocytes + how they recognize Ag?
TH cell subtypes + signature secreted cytokine + fxns
How can an immune response to 1 type of pathogen inhibit the response to a different kind of pathogen w/ a clinical example?
Describe what you could do to get T cell help to B cells when B cells are responding to a polysaccharide antigen (like a bacterial capsule). Remember, a TH cell recognizes a peptide in an MHC II molecule
3 significant signals req. to activate a T helper cell + 2 significant factors that determine predominant TH cell subtype?
General expected response to a modified live vaccine vs inactivated (killed) vaccine?
all 5 canvas diagrams
Animals infected with Mycobacterium bovis (bovine TB), an intravesicular pathogen, will test positive on a bovine TB intradermal skin test + gamma interferon test.
In a bovine TB intradermal skin test, Tuberculin (a purified protein from the organism) is injected into the skin dermis. 72 hrs later, there is a palpable lump at the site where the antigen was injected, indicating the animal is infected. The lump does not appear in an animal that is not infected.
a) If you did a biopsy of the lump with a light microscope, what would the predominant cell type be? (The lump is an indication of an immune memory response to this intravesicular pathogen.
b) Explain how the predominant cells leave the bloodstream, including the initiating event and important molecules involved. (FYI - when the tuberculin is injected there is a local inflammatory response)
c) The gamma interferon test for bovine TB is a blood test. The mononuclear cells from a whole blood sample are isolated from a cow. What are the two different types of mononuclear cells identifiable with a light microscope in the bloodstream (i.e., those that are not RBCs or granulocytes)?
e) When the tuberculin is added to these cells, a measurable amount of gamma interferon is produced if the cow is infected with the organism. In a cow that is not infected, there is not a measurable amount of gamma interferon produced. What cell type is producing the majority of the gamma interferon?
f) How would this cell be presented with the antigen in this in vitro test? And what cell type is presenting the antigen?
Haemophilus influenzae B conjugate vaccine (diphtheria toxoid-conjugate) is a vaccine approved for use in ppl 18 mo or older. The vaccine consists of Haemophilus b capsular polysaccharide covalently linked to diphtheria toxoid. In clinical trials, the conjugate vaccine showed greater immunogenicity than the polysaccharide only vaccine. >90% of the children vaccinated with conjugate vaccine responded with IgG levels considered to be protective. In contrast, less than 50% of the children vaccinated with polysaccharide vaccine had such a response. Please explain the improved immunogenicity of the conjugate vaccine over the polysaccharide
alone.
a) Based on what you know about B cell and T cell recognition of antigen, what type of immune response would you expect from the polysaccharide alone vaccine?
b) What type of immune response would you expect following the conjugate vaccine?
c) What is the reason for the differences in the responses?
Explain what a γδ T cell is + its role in the immune response
Generally, how is apoptosis induced + what happens in a cell that is induced to undergo apoptosis?
Apoptosis vs necrosis cell characteristics
3 mechanisms that cytotoxic T cells (CTL) use to kill target cells?
3 mechanisms for NK cell activation? How do normal cells escape NK cells?
How do CTL + NK cells complement each other?
7 (?) killing cells of the immune system, broad 2 categories of killing mechanisms (necrosis vs apoptosis), more in depth ab how they kill
2 parts of innate immune response + 2 parts of adaptive immune response important for protection against viruses?
Where do Type 1 interferons come from + what do they do?
Type 1 interferon (alpha + beta) vs Type 2 interferon (gamma)
What important properties do you need for a vaccine to stimulate CTLs?
Draw an ELISA to detect an Ag like feline leukemia virus. Label all reagents + conjugate. Interpret a positive vs negative result.
Draw an ELISA to detect an Ab like feline Ab to FIV. Label all reagents + conjugate. Interpret a positive vs negative result.
Draw the last well of an ELISA test showing positive for FIV Ab. Be sure to draw the Ag-binding site of the Ab binding its epitope. Label all molecules + conjugate.
Explain the differences in interpretation of a positive Ag test vs positive Ab test.
Describe a lateral flow immunoassay (lateral flow chromatography) + the basic differences compared to an ELISA-based assay.
Explain what the precipitate is in a precipitation assay, what the equivalence zone means, and why there is no precipitate when there is Ab/Ag excess.
Define titer + describe how a titer is determined.
Describe the consequences of fetal infection. What factors influence the outcome?
Compare + contrast how neonates of different domestic species receive passive Ab from their mother (primates, SA, horse, cow, pig)
Explain how the absorption of colostral Ab + describe the unique neonatal gut features that allow absorption of whole Ig molecules.
What is “gut closure”? When does it occur? How does it occur?
Colostrum vs milk including type of Ab, source of Ab, concentration of Ab
Briefly explain + draw how SRID vs SNAP vs TIA assays work for diagnosing FPT in foals
How is central vs peripheral tolerance induced?
Explain the 4 major components of T cell tolerance + when, where, and how it develops
How does the thymus change w/ age? How does that affect immunity + disease later in life?
2 most conserved immune protective mechanisms in insects up thru mammals?
How do birds transfer immunity to their young?
Explain major differences b/t protective immune response induced by vaccines in mammals, avians, and higher-lvl aquatic animals vs crustaceans + insects
5 nonimmunologic surface protective mechanisms
Common mucosal vs systemic immune system
What are M cells? Where are they found? What is their fxn?
Draw basic IgA molecule. List unique characteristics, location, and key fxns
Draw + list steps to explain transfer of IgA from basal side of mucosa across epi. cell into lumen.
Explain the fxn of the secretory component as it relates to IgA + where IgA acquires it
Explain how sIgA to an intestinal pathogen can be found in the milk of a mare + how it protects her newborn foal from that pathogen?