CHAPTER 7: PART II
1/51
Earn XP
Description and Tags
ERRORS IN ACCESS CAVITY PREPARATION & CLASSIFICATIONS OF C-SHAPED / PULP FLOORS
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
52 Terms
safety-tip tapered diamond bur
used to blend and funnel the axial wall from the cavosurface margin to the orifice
used to shape the axial wall in one plane from the orifice to the cavosurface margin
mouse hole effect
orifice that lies completely on the pulp floor
caused by extension of the orifice into the axial wall
cause of loss of significant clinical crown structure
untreated caries, which undermine the tooth
fractures from occlusal stress in badly decayed teeth
trauma, sometimes shearing the crown to the free gingival margin
teeth heavily restored with amalgam, composite, or glass ionomer, which provide no extra-coronal support
access preparation on heavily restored teeth is challenging due to:
reduced visibility — because most restorative materials block light from reaching the pulp chamber
altered external anatomical landmarks — as restorations and full crowns rarely reproduce the original tooth anatomy
changed crown-to-root angulation — especially when large restorations or crowns were placed to correct occlusal discrepancies
reasons for complete removal of restorations:
facilitate treatment of calcified canals (under class V restorations)
prevent coronal leakage: loose fragments can be vibrated or displaced during drilling
avoid canal contamination: fragments can be carried into the canal during shaping, creating metal or composite filings
improve visibility: removal allows direct access to root canals and helps detect recurrent caries, fractures, or calcifications
chamber floor
darker than walls
developmental grooves
lighter than floor
additional aids for locating calcified root canals
canal bleeding points
1% methylene blue staining
sodium hypochlorite “champagne bubble” test
common problems if rotated tooth is not considered:
failure to locate additional or extra canals
instrument separation during canal location attempts
incomplete removal of pulp tissue from the chamber
excessive gouging of coronal or radicular tooth structure
mistaking one canal for another → searching in the wrong direction
poor access placement / inadequate mesial extension
mesial orifices left uncovered
causes:
failure to correctly locate pulp chamber
inadequate evaluation of tooth anatomy
prevention for poor access placement / inadequate mesial extension
carefully plan access outline
assess CEJ and tooth morphology
use pretreatment radiographs (especially bite-wings)
inadequate distal extension
distobuccal canal orifice unexposed
causes:
developmental grooves not traced to termination; cavity not extended distally
prevention for inadequate distal extension
trace all developmental grooves full
ensure distal access reaches canal orifices
gross overextension
weakens coronal tooth structure, compromises restoration
causes:
improper bur angulation
incorrect determination of pulp chamber position
prevention for gross overextension
avoid excessive removal
follow correct access cavity guidelines
evaluate pulp chamber position and angulation
debris in canal orifices
blocks canals, hinders shaping and cleaning
allowing amalgam or dentin fragments to fall into orifices
prevention for debris in canal orifices
completely remove restorations; perform copious irrigation before locating canals
failure to remove pulp chamber roof
pulp horns exposed
underextension; incomplete access
prevention for failure to remove pulp chamber roof
ensure roof and pulp horns fully removed
use bite-wing radiographs to determine vertical depth
mistaking pulp horns for canal orifices
causes:
roof remains
shallow cavity
shallow depth
absence of grooves
lack of developmental grooves
color differences not recognized
prevention for mistaking pulp horns for canal orifices
remove roof completely
identify whitish roof color
remember true orifices are at or slightly apical to CEJ
overzealous tooth removal
causes:
weakens / mutilates coronal structure
risk of coronal fracture
improper bur angulation
failure to recognize lingual inclination
prevention for overzealous tooth removal
evaluate tooth angulation
adjust bur orientation
remove dentin gradually and conservatively
inadequate opening
causes:
access too gingival
pulp horn retention
poor instrumentation
leads to bur/file breakage
ledging, apical transportation
access cavity misplaced or too small
insufficient extension & no incisal extension
prevention for inadequate opening
check pulp chamber depth
ensure proper incisal extension
follow straight-line access principles
labial perforation
causes:
failure to extend preparation incisally before bur penetration
prevention for labial perforation
plan cavity outline carefully
extend incisal wall before full penetration
confirm with radiographs
furcation perforation
opening into periodontal tissues, weakens tooth
cause:
incorrect depth measurement between occlusal surface and furcation
prevention for furcation perforation
use careful bur control
confirm with radiographs
repair immediately if occurs
measure occlusal-to-furcation distance
mesial perforation
often in crowned teeth
causes:
bur not aligned with long axis
failure to recognize tooth tipping
causes long-term periodontal problems
prevention for mesial perforation
align bur with long axis
radiographic confirmation
cautious preparation in crowned teeth
evaluate crown angulation preoperatively
entering the wrong tooth
high risk of medical / legal consequences
causes:
incorrect dental dam placement
visually similar crowns
prevention for entering the wrong tooth
mark the correct tooth with a felt-tip marker before placing the dental dam
verify tooth identity carefully
broken burs or files
can lock in canal
causes:
improper motion
excessive pressure
may require excessive tooth removal
prevention for broken burs or files
using instruments before proper access
handle instruments carefully
use correct motion and pressure
ensure proper access cavity preparation first
main cause of C-shape roots and canals
failure of Hertwig’s epithelial root sheath to fuse on either the buccal or lingual root surface
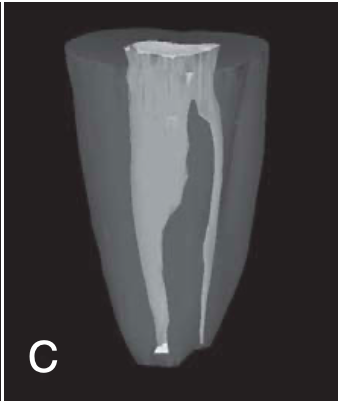
C-shaped roots and canals
most common in MN 2nd molars
also reported in MN 1st molars, MX 1st & 2nd molars, MN 1st premolars
can vary along the root depth so that the appearance of the orifices may not be good predictors of the actual canal anatomy
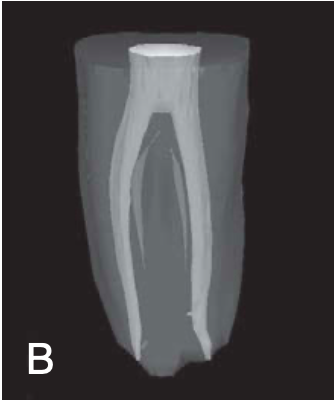
2 basic types of C-shaped roots and canals
single ribbonlike canal — from orifice to apex (rare)
multiple distinct canals — below the C-shaped orifice (more common)
feature of a root canal obturation
ribbonlike canal space with an arc of 180 degrees or more
category I (C1) of C-shaped root canal
the shape is an uninterrupted “C” with no separation or division

category II (C2) of C-shaped root canal
should be no less than 60 degrees
the canal shape resembles a semicolon resulting from a discontinuation of the “C” outline

category III (C3) of C-shaped root canal
2-3 separate canals and both angles are less than 60 degrees

category IV (C4) of C-shaped root canal
only one round or oval canal is in the cross-section
category V (C5) of C-shaped root canal
no canal lumen can be observed (is usually seen near the apex only)
MN 2nd molars
where four types of pulpal floors are found
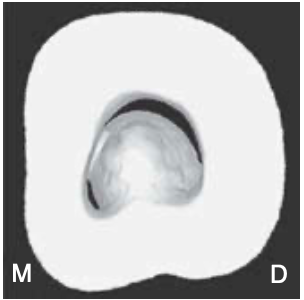
type I of pulpal floors
a peninsula-like floor with continuous C-shaped orifice
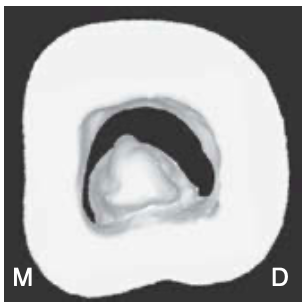
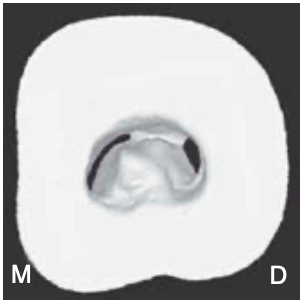
type II of pulpal floors
A buccal, striplike dentin connection between the peninsula-like floor and the buccal wall of the pulp chamber that separates the C-shaped groove into mesial (M) and distal (D) orifices.
Sometimes the mesial orifice is separated into a mesiobuccal (MB) orifice and a mesio- lingual (ML) orifice by another striplike dentin connec- tion between the peninsula-like floor and the mesial wall of the pulp chamber (most common)
type III of pulpal floors
only one mesial, striplike dentin connection exists between the peninsula-like floor and the M wall
which separates the C-shaped groove into a small ML orifice and a large MB-D orifice
MB-D orifice was formed by the merging of the MB orifice and the D orifice (second most common)
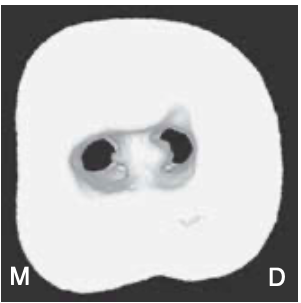
type IV of pulpal floors
non–C-shaped floors
one distal canal orifice and one oval or two round mesial canal orifices are present (least common)
type I of Three-dimensional classification of C-shaped canal
(merging type)
canals merge to one main canal before exiting at the apical foramen

type II of c-shaped canal
(symmetrical type)
separated mesial and distal canals in each root, which exit as separate canals
type III of c-shaped canal
asymmetrical type
separated mesial and distal canals, with the distal canal having a long isthmus across the furcation area