The nature of depression
1/30
Earn XP
Description and Tags
Aftab Laher
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
31 Terms
What is depression?
A clinical syndrome distinct from sadness and includes non-transient depressed mood.
Key themes include Pervasive feelings of loss, emptiness, entrapment/helplessness, worthlessness, and hopelessness.
Impairment in aspects of daily functioning.
Clinical presentation may be ‘asked’ or may vary.
Physiological, emotional cognitive-motivational, behavioural and social/interpersonal symptoms and signs which interact.
Importance of validating feelings in context.
Importance of seeing ‘depression’ as a socio-cultural construct.
How does the ICD-11 describe depressive disorders?
o Single episode depressive disorder
o Recurrent depressive disorder- continuous in one shape or abother
o Dysthymic disorder
o Mixed depressive and anxiety disorder.
o Other specified depressive disorders
o Depressive disorders, unspecified.
How does the ICD-11 describe bipolar and related disorders?
o Bipolar type 1 disorder- manic episode are worse (reckless, impulsive)
o Bipolar type 2 disorder
o Cyclothymic disorder- sort of like bipolar- months/period of time where people are disengaged followed by months where participants are calmer. Can and will be noticeable
o Other specified bipolar or related disorders
o Bipolar or related disorders unspecified.
How does DSM-5-TR decrive depressive disorders?
o Major depressive disorder (MDD)
o Disruptive mood dysregulation disorder- easily fragile, may have anxiety.
o Persistent depressive disorder (Dysthymia)
o Premenstrual dysphoric disorder
o Substance/medication- induced depressive disorder.
o Depressive disorder due to another medical condition
How does the DSM-5-TR describe bipolar and related disorders?
o Bipolar type I disorder
o Bipolar type II disorder
o Cyclothymic disorder
o Substance/ Medication-Induced Bipolar Disorder
o Bipolar or Related Disorder Due to Another Medical Condition
o Other Specified Bipolar or Related Disorder
o Bipolar or related disorders, unspecified
What are the signs of major depressive disorder?
At least one of the following symptoms that causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
At least one of the systems is 1) a depressed mood or 2) loss of interest or pleasure.
Symptoms must be present almost every day for two weeks.
1. Depressed mood most of the day
2. Diminished interest or pleasure or most activities.
3. Significant unintentional weight loss or gain.
4. Insomnia or sleeping too much.
5. Agitation or psychomotor retardation noticed by others.
6. Fatigue or loss of energy.
7. Feelings of worthlessness or excessive guilt.
8. Diminished ability to think or concentrate or indecisiveness.
9. Recurrent thoughts of death.
What other syndromes come with depression?
Seasonal affective disorder (SAD)- clinical depression during 2 consecutive winters which resolves in summer.
Psychotic depression
Post-natal depression
Adjustment disorders (‘reactive depression’)
PTSD
What are the broad determinants of depression?
Sociocultural context
Genetics/biomedical factors
Life events/stress/big changes
Conditioning/learning
Cognitive style/outlook/meaning making
Drugs/alcohol
Other illnesses
Personality
Lifer history
Lifestyles
What can depression often be associated with?
Bereavement- especially complex grief
Relationship difficulties/ separation
Problems at work
Problems with family members
Lack of intimacy/intimate relationship
Isolation
Role change/loss of identity
What are theoretical approaches explaining depression?
Biological
Behavioural
Personality factors
Psychodynamic approaches
Attachment theory cognitive models
Interpersonal model.
What is the Biological explanation?
Twin and family studies- modest heritability
Neurotransmitter imbalances or dysregulation (primarily serotonin and, noradrenaline but also cortisol and dopamine).
Other brain or neuropsychological abnormalities
What are the criticism of biological explanation?
Depression is a complex condition and not just caused by chemical imbalance.
Meta analysis found no association between imbalances and depression- patients with imbalances didn’t portray depressive symptoms- suggesting that biological reasonings are not Soley responsible for explaining depression
Support of biological explanation…
Research suggests depression and selective genes such as those which contribute to stress have shown associations
Twin studies- a Swedish study found that lifetime major depression was heritable is study suggests both that the heritability of major depression is higher in women than in men and that some genetic risk factors for major depression are sex-specific in their effect.
What is the behavioural explanation of depression?
Learned helplessness – classical conditioning (Seligman, 1975) the person learns that the efforts they are making is fruitless so not worth making the effort. How can this be helped and can it be changed to a more positive form.
Reduction in positive reinforcers/ increase in negative reinforcers – operant conditioning (Lewinsohn, 1974) depression results from a reduction in response- contingent positive reinforcement in an individual’s environment, meaning a decreased rate of exposure to pleasant events. This reduction can stem from a lower number of reinforcing events. Simultaneously, an increase in aversive/punishing events will also contribute to the development of depressive symptoms.
Social learning theory- learning from others, modelling, observation how we think we should be. Can be vicious cycles.
Formation of “vicious cycles” of behaviour which maintain depression
Criticism of the behavioural explanation…
The social learning theory can be criticised for being reductionist, by focusing mainly on external factors like observational learning and neglecting internal cognitive processes and emotions that may influence behaviour.
Underestimates individual differences.
Learned helplessness- the theory fails to explain why some people learned helplessness after negative events while ithers do not
As well as not being able to explain depressions core symptoms.
Classical conditioning can oversimplify complex human behaviours by reducing them to automatic responses.
Operant conditioning is reductionist and ignores biological factors and doesn’t account for internal motivations and complex behaviours.
what is the psychodynamic explanation for depression?
Psychodynamic theories view depression in terms of inwardly directed anger, loss of self-esteem or self-worth, egotistic or excessive narcissistic or personality demand, or deprivation in mother-child relationship (loss or rejection by a parent). Freud’s (1917) psychoanalytic theory is an example of the psychodynamic approach. Repressed anger at a loss (symbolic or actual loss of a loved one during childhood, for example) is directed inwards, reduces self-esteem and increases vulnerability to further experiences in the future, causing the individual to ‘re-experience’ (symbolic or actual) the loss when encountering similar triggering stimuli during adulthood. The theory argues that people prone to depression have an excessively high interpersonal dependency (i.e. they seek approval and reassurance from others – to be loved, respected, admired, appreciated,etc. and depression arises when they fail to receive it). Those who may depend on others for their sense of self-esteem may therefore remain in a more vulnerable ‘depression-prone’ state.
Compares depression with grief.
Grief: In consciousness; sadness; rage; anger; no loss of self-esteem.
Depression: May not be aware of loss; rage/ anger and disappointment turned inward; loss of self-esteem (feeling helpless, worthless, inadequate)
Both are painful states of mind
‘Loss’ is central to both
Idea of “introjection”
Critiques of psychodynamic explanation in explaining depression…
There is a lack of scientific testability and focus on the past over current issues.
there is large dependencies on subjective interpretation of feelings and how well the theory explains depression and a large lack of empirical evidence with a neglect. of conscious factors that contribute to depression
the theory suggests behaviour is entirely caused by unconscious emotional drives leaving little room for free will undermining individual responsibility and conscious choice.
What is the later development of ‘neo-freudian’ explanation of depression?
Many schools of psychoanalysis and psychodynamic psychotherapy have developed.
Object relations theory- more modern psychodynamic perspective (roots in UK in 1940s and 50s). people and relationships represented internally as ‘objects’.
Depressive vulnerability created by caregivers pushing children towards either excessive independence of excessive reliance on caregiver.
Become depressed when lose important relationship in later life.
Common issue in depression = ‘being deeply angry with someone deeply loved and needed’
What is Attachment theory 1?
Modern theory based partly on some psychodynamic idea developed by john Bowlby.
Attachment: lasting psychological connectedness between human beings.
Child builds internal working models of self and other.
Child depends on primary caregiver to provide a secure caring base- allows child to safely explore but be confident of support.
If receive inadequate care in childhood, then:
Builds model of self as inadequate, unlovable etc.
Builds model of other as unavailable, hostile etc.
Leads to lowering of self-esteem.
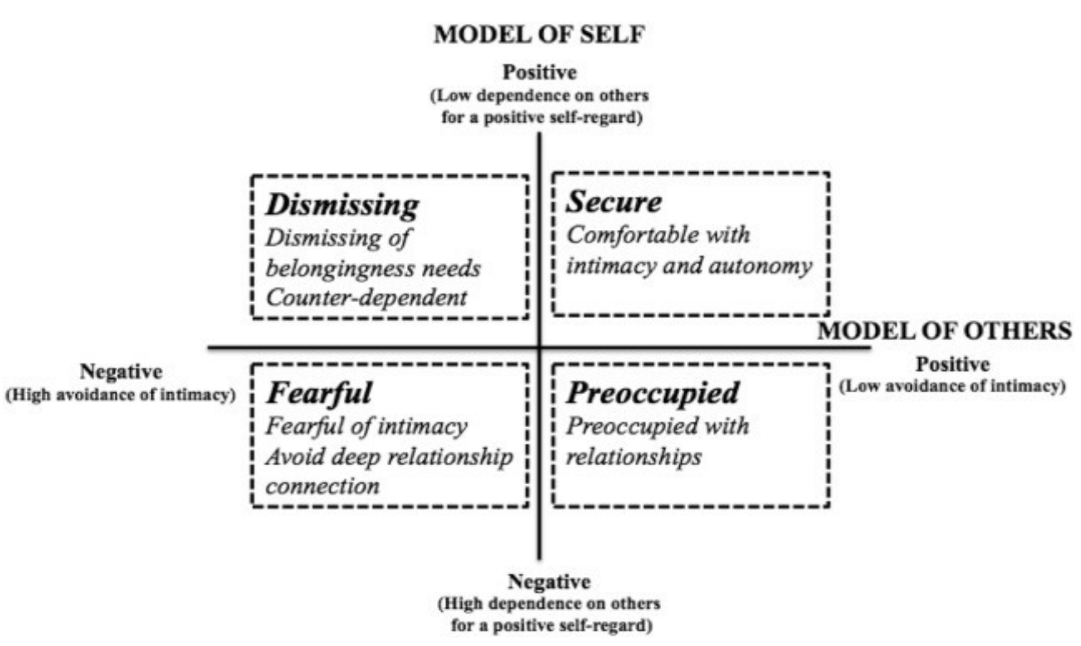
What is attachment styles?
Secure is the best
Dismissing- dismissive of others, don’t need others. May come from deeper issues (being hurt before)
Preoccupied- Negative about self and positive about others, may become over attached- can be abused and explosive.
Fearful- negative of self and others- non trusting lost of anxiety
People can vary overtime and between different people.
What is attachment theory 2?
Child grow to be an adult- if the model of self is negative can grow up depressed.
At times of stress (e.g., loss of close relationship):
Negative internal working models of self and others are still in place and become active.
If feelings of self-worth not strong enough, then these models may generalise to life in general.
Depression may result.
How does the cognitive models explain depression?
How we think how we compute, will affect our mood.
Theory of casual attribution (re-formulated learned helplessness theory) (Abramason, Seligman and Teasadle, 1978)
How the cause of the depression is attributed.
Depression more likely if attribution is: 1) internal (vs external); 2) stable (vs. unstable); 3) global (vs specific)
Cognitive behavioural approach (Beck, 1979)- greatest evidence base.
Original formulation- emotional difficulties due to problems with thinking and behaviour.
Evolved formulation- recognition of socio-cultural context.
Posits that depression is caused by negative thinking patterns, or cognitive biases which develop from core negative beliefs (schemes) and are triggered by stressful events.
Criticisms of cognitive models at explaining depression…
They are correlational rather than causal, focus too narrowly on immediate symptom relief and maintaining factors, may be over simplifying depression by neglecting biological factors and past trauma.
Over simplifying complex human h=behaviour, there is a large reliance artificial laboratory settings leading to low ecological validity.
It suggests emotions are of minimal importance.
What are the assessments of depression?
Importance of comprehensive clinical assessment.
Clinical interview/observation
Psychometric questionnaires, e.g.,
Patient health questionnaire (PHQ-9)
Beck depression inventory (BDI-II)
Hospital anxiety and depression scale (HADS)
Information from others (with consent)
What is the classification of depression?
Onset (sudden/gradual)
Severity (mild, moderate, severe)
Features (melancholic catatonic etc.)
Duration
Course/recurrence (longitudinal, seasonal, rapid cycling etc.)
What are the five core dimensions to consider?
Physiological/sensations/ physical
Emotional/subject feelings
Cognitive/appraisal/ meaning/ thought processes/ motivation.
Behavioural/ activity/ lifestyle.
Social/ interpersonal/ environment.
what is the physiological assessment of depression?
Loss of appetite/ overeating
Loss of weight/weight gain (rapid)
Sleep disturbance (insomnia/oversleeping)
Fatigue/ loss of energy/ lethargy.
Aches/ pains
Marked loss of libido
Slumped posture.
what is the emotional/ affecrive assessment of depression?
Low/depressed mood/ tearful.
Intermittent mania/ hypomania
Emptiness/numbness
Sense of loss
Anger/ resentment
Anxiety
Shame
Guilt
Anhedonia (difficulty seeking or feeling pleasure)
What is the cognitive-motivational assessment of depression?
Negative cognitive triad:
self: worthless, inadequate, defective etc.
world: negative, unsupportive, overwhelming etc.
future: bleak, hopeless etc.
Poor concentration
Forgetfulness
Less sharp/ less creative/ poor decision-making
Things seem pointless
Some ideations about self-harm/ suicide
Negative rumination about symptoms (meta-cognition) §Negative flashforwards
Apathy/ lack of initiative or drive
What is behavioural assessment of depression?
Lowered activity levels
Give up on hobbies/ enjoyable activities
Avoidance
Self-defeating behaviours
Recklessness
Self-harm
Neglect personal care
Hoarding or getting rid of valued things
What is the social-interpersonal assessment of depression?
Withdrawal
Disengagement
Loss of social confidence/skills
Disinhibition
Seek to validate worthlessness
Feeling of not belonging
Rejection