Hematology & Aenmia
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
Plasma comprise what % of blood?
55%
RBCs comprise what % of blood?
45%
Is a deficiency in:
# of RBCs
Quantity or quality of Hgb
Volume of packed RBCs (Hct)
Anemia
Causes of anemia
Decreased RBC production
Blood loss
Increased RBC destruction (hemolysis)
Function of RBCs
Transport O2 from lungs to systemic tissues, and CO2 from tissues to lungs
Normal Hgb
Female 12-16 g/dL
Male: 14-18 g/dL
Normal WBC
5,000-10,000/uL
Normal platelets (plt)
150,000-400,000/uL
Mild anemia is classified as
Hgb 10 to 12 g/dL
Moderate anemia is classified as
Hgb 6 to 10 g/dL
Severe anemia is classified as
Hgb < 6 g/dL
May exist without causing symptoms (asymptomatic). If symptoms develop, it is because the patient has an underlying disease or has a compensatory response to heavy exercise. Symptoms include palpitations, dyspnea, and mild fatigue.
Classified as Hgb 10 to 12 g/dL
Mild anemia
There is an increase in cardiopulmonary symptoms. The patient may have them while resting as well as with activity.
Classified as Hgb 6 to 10 g/dL
Moderate anemia
The patient has many manifestations involving multiple body systems
Classified as Hgb < 6 g/dL
Severe anemia
Normal CBC
Hgb
Female 12-16 g/dL
Male: 14-18 g/dL
WBC
5,000-10,000/uL
Plt
150,000-400,000/uL
S&S of mild anemia
May be asymptomatic
Response to heavy exericse:
Palpitations
Dyspnea
Mild fatigue
S&S of moderate anemia
Fatigue
Palpitations-bounding pulse
Dyspnea
S&S of severe anemia
Pallor
Dizziness
HA/vertigo/impaired cognition
Exhausted/lethargic
Severe palpitations, tachycardia/bounding pulse
Orthopnea, dyspnea at rest
Sensitive to cold
Anorexia
Pallor
Dizziness
HA/vertigo/impaired cognition
Exhausted/lethargic
Severe palpitations, tachycardia/bounding pulse
Orthopnea, dyspnea at rest
Cold sensitivity
Anorexia
What condition do these symtpoms describe?
Severe anemia
Fatigue
Palpitations-bounding pulse
Dyspnea
What condition do these symtpoms describe?
Moderate anemia
May be asymptomatic
Response to heavy exericse:
Palpitations
Dyspnea
Mild fatigue
What condition do these symtpoms describe?
Mild anemia
This morphology describes what anemia?
Normal size and color
MCV 80-100fL, MCH 27-34 pg
Normocytic, normochromic anemia
This morphology describes what anemia?
Small size, pale color
MCV <80 fL, MCH <27 pg
Microcytic, hypochromic anemia
This morphology describes what anemia?
Normochromic (large size, normal color)
MCV >100 fL, MCH >34 pg
Macrocytic (megaloblastic) anemia
This etiology describes what anemia?
Acute blood loss, hemolysis, CKD, chronic disease, cancer, endocrine problems, starvation, aplastic anemia, sickle cell anemia, pregnancy
Normocytic, normochromic anemia
This etiology describes what anemia?
IDA, vitamin B6 deficiency, copper deficiency, thalassemia, lead poisoning
Microcytic, hypochromic anemia
This etiology describes what anemia?
Cobalamin (vitamin B12) deficiency, folic acid deficiency, liver disease (including effects of alcohol use)
Macrocytic (megaloblastic) anemia
What are the causes of normocytic normochromic anemia?
Acute blood loss, hemolysis, CKD, chronic disease, cancer, endocrine problems, starvation, aplastic anemia, sickle cell anemia, pregnancy
What are the causes of microcytic hypochromic anemia?
IDA, vitamin B6 deficiency, copper deficiency, thalassemia, lead poisoning
What are the causes of macrocytic (megaloblastic) anemia?
Cobalamin (vitamin B12) deficiency, folic acid deficiency, liver disease (including effects of alcohol use)
MCV 80-100 fL
MCH 27-34 pg
This indicates which anemia?
Normocytic normochromic anemia
MCV <80 fL
MCH <27 pg
This indicates which anemia?
Microcytic hypochromic anemia
MCV >100 fL
MCH > 34 pg
This indicates which anemia?
Macrocytic (megaloblastic) anemia
Patients who drink alcohol have increased risk of
Macrocytic anemia (liver disease, folic acid, and vit B12 deficiency)
Diagnostic studies for anemia
CBC (Hgb, Hct, WBC, plts)
RBC indices
Mean Corpuscular Volume (MCV)
Mean Corpuscular Hemoglobin (MCH)
Serum ferritin
Serum iron
TIBC
B12
Folate
Schilling test to evaluate B12 absorption
Hct = 3 times of
Hgb
RBC indices (part of diagnostic study of anemia)
Mean Corpuscular Volume (MCV)
Mean Corpuscular Hemoglobin (MCH)
Serum ferritin
Serum iron
Total iron binding capacity (TIBC)
CBC (part of diagnostic study of anemia)
Hgb, Hct, WBC, plts
Nutritional studies for diagnostic study of anemia
B12
Folate
Schilling test to evaluate B12 absorption
Iron
Decreased RBC production can be caused by
IDA
Thalassemia
Sideroblastic (bone marrow RBC production disorder)
Decreased # of RBC precursors can be caused by
Aplastic anemia
Medications & chemicals
Radiation
Nutritional anemias include
IDA
Macrocytic/megaloblastic anemias (B12 or folate deficiency)
Hereditary (intrisnic) disorder that can lead to anemia
Sickle cell idsease
Acute OR chronic blood loss can both lead to anemia. True or false?
True
Management of anemia:
Depends on Hgb & Hct
Stop the bleeding/treat underlying cause
Blood transfusions
Acute interventions for anemia may include
Blood transfusions
Drug therapy (e.g. iron supplements, narcotics for sickle cell crisis)
O2 therapy
Anemic patients with fatigue education
Tell them to alternate rest and activity
Focus on priortizing activities
Accomodate energy levels
Maximize O2 supply for vital functions
Aid to minimize r/o injury from falls
Monitor cardiopulmonary response
Evaluate nutrition needs (B12, folic, iron deficiencies)
Identifying patients correctly to eliminate transufsion errors
2 licensed personnel identificaiton process (transfusion staff and another licensed provider)
Verification of HCP’s order
Verification of consent to receive blood
Verification of blood type w/ transfusion product
Causes of IDA
Chronic blood loss (GI or GU system), or hemolysis
Menstruation
Inadequate dietary iron intake
Inadequate iron absorption in GI tract
GI surgeries, involving bypass of duodenum
Malabsorption syndromes
S&S of IDA
Depneds on age and severity
Few symptoms until HCT < 30
Pallor
Glossitis
Chelities
HA, paresthesia
When do patients with IDA typically manifest symptoms?
Few symptoms until HCT < 30
Pallor
Glossitis
Chelities
HA, paresthesia
Depends on age & severity
History for IDA
Menstrual hx
Onsert and duration of symptoms
Change in stool patterns (black, tarry stools = chronic blood loss/occult bleeding)
Dietary intake
Medication hx
Physical exam for IDA
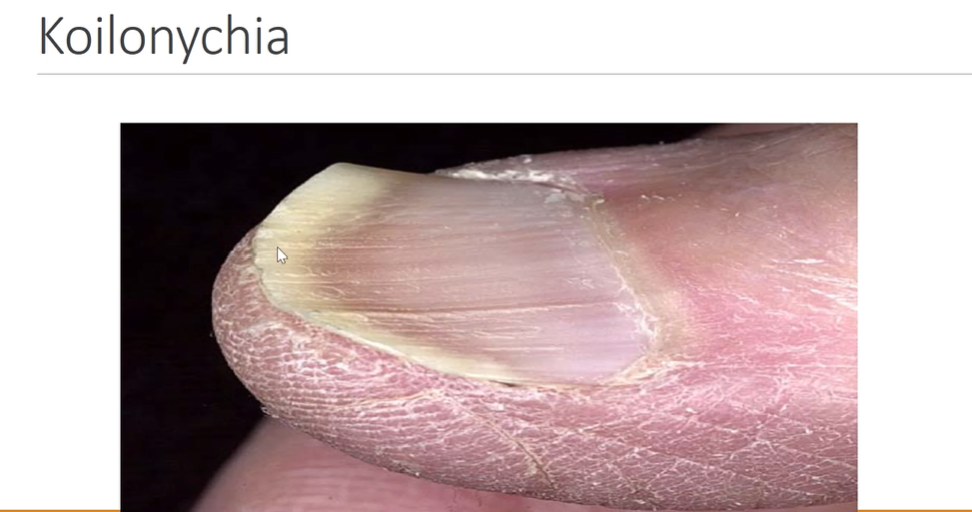
Skin & nails assessment
Assess skin for pallor, jaundice, pruritis
Assess nails for koilonychias (spoon shaped nails)
Tongue/mouth assessment
Examine tongue for atrophic glossitis, burning sensation
Examin corners of mouth for cheilosis (red, cracked skin at corners of mouth)
Palpate abdomen for tenderness
Splenomegaly
Stool assessment
Obtain stool for occult blood

Tongue/mouth assessment for IDA
Examine tongue for atrophic glossitis, burning sensation
Examin corners of mouth for cheilosis (red, cracked skin at corners of mouth)
Skin & nails assessment for IDA
Assess skin for pallor, jaundice, pruritis
Assess nails for koilonychias (spoon shaped nails)
Diagnostic studies for IDA
Labwork: Hgb, HCT, Plts, MCV, MCH, MCHC, reticulocytes, serum iron, TIBC, bilirubin
Stool occult blood test
Endoscopy and colonoscopy
Bone marrow biopsy
Labwork for IDA:
Hgb, HCT, Plts, MCV, MCH, MCHC, reticulocytes, serum iron, TIBC, bilirubin
What does the typical labwork for IDA patient look like?
CBC → eventually low
Serum iron → decreased
TIBC → high
Serum ferritin → low
MCV → low
MCH → low
CBC → eventually low
Serum iron → decreased
TIBC → high
Serum ferritin → low
MCV → low
MCH → low
What do these lab findings indicate?
IDA
Goal for treating IDA
Treat underlying problems, causing blood loss, reduced intake, or poor absorption of iron
Replacd iron via:
Nutrition therapy
Oral iron supplements
Transfusion of packed RBCs
What is the first lab to drop in early IDA?
Serum ferritin
Lab value that measures iron stores; is the first to drop in IDA
Serum ferritin
Lab value that measures circulating iron, carried by transferrin). Drops after serum ferritin in IDA
Serum iron
Lab value that measures ability of cells to bind to iron. Is normally inversely related to serum iron (when serum iron is low, TIBC is high)
TIBC
TIBC is directly proportional to serum iron (TIBC will be high if serum iron is high). True or false?
False
Treatment of IDA
Oral iron therapy (supplements
Teach about foods high in iron
Take iron between meals or one hours before
Take with vitamince (OJ if not DM) improves absorption
May cause constipation (can also cause diarrhea in some)
Correct the cause of bleeding
Iron-rich foods include:
Animal sources
Meat (esp red meat)
Fish
Eggs
Plant sources
Leafy greens
Legumes (beans, lentils, peas)
Whole-grain
Why should you take iron supplements between meals or one hour before?
Iron supplements are absorbed best on an empty stomach because food can significantly interfere with iron absorption (food in stomach binds with iron, decreasing absorption)
Why take iron with vitamin C (OJ)?
Improves iron absorption
What do you need to teach the patient about their stools when they are taking oral iron supplements?
Their stool will be black in color