Hypertension
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Hypertension (HTN)
an office blood pressure of 140/90 mmHg or above
taken at least twice on two separate days
(though 2017 AHA considers 130/90 the cutoff value)
Hypertension Prevalence
in the PH, shows a decreasing trend
32.9% (2013) → 19.2% (2018) for ages 20-59
41.2% (2015) → 35% (2018) for ages ≥ 60
Awareness:
awareness is about 67.8%, of which 75% are treated, and 27% of treated have controlled HTN
of 100% of people with it, only 47% are aware that they have it, 37% are treated, and only 14% have controlled BP
Sympathetic Nervous System Regulation
baroreceptors in the carotid and aortic arch respond to changes in BP
if elevated BP is sustained, the baroreceptors reset at higher levels
this creates sustained elevated BP (the receptors are used to high BP)
Renin-Angiotensin-Aldosterone System (RAAS) Regulation
Renin is produced in the kidney
Angiotensinogen is produced in the liver
Produced Renin cleaves Angiotensinogen into Angiotensin I
ACE converts Angiotensin I to Angiotensin II
Angiotensin II acts on adrenal glands to produce Aldosterone
Primary Hypertension
Primary Hypertension
also essential hypertension
results from unknown pathophysiologic etiology
genetic factors may play a role
cannot be cured, but can be managed
more common
Secondary Hypertension
results from specific cause
may be due to comorbid disease
may be due to drug
renal dysfunction due to CKD is most common cause
can be mitigated and potentially cured
first step should be removal of offending agent
OR correction of underlying comorbid disease
less common
Hypertensive Emergency
type of hypertensive crisis
severe elevations in BP (usually > 180/100)
with presence of acute or ongoing target-organ damage
requires immediate BP lowering
not necessarily to normal range, just to lower target range
goal is to lower BP to prevent or limit further target-organ damage
Hypertensive Urgency
type of hypertensive crisis
accelerated, malignant, or perioperative HTN without symptoms or new/progressive target-organ damage
short-term risk is not as high; BP reduction occurs over several days
Modifiable Risk Factors
can be changed or altered
smoking
diabetes mellitus
dyslipidemia/hypercholesterolemia
obesity
physical inactivity/low fitness
unhealthy diet
Nonmodifiable Risk Factors
cannot or is difficult to change or alter
CKD
Family History
Increased age
Low socioeconomic status
Low educational status
Being male
Obstructive Sleep Apnea
Psychosocial Stress
Hypertension-Mediated Organ Damage
structural or functional alteration of arterial vasculature or the organs it supplies that is caused by elevated BP
Brain:
stroke
dementia
Arteries:
artery damage and narrowing
aneurysm
leg amputation
Heart:
coronary heart disease
heart attack
congestive heart failure
Kidneys:
kidney failure
kidney artery aneurysm
Assessment for Hypertension-Mediated Organ Damage
serum creatinine
eGFR
dipstick urine test
12-lead ECG
MRI
fundoscopy
carotid ultrasound
others
Hypertension Categories and Therapeutic Thresholds
for Filipino adults:
Normal BP: < 120/80 mmHg
Borderline BP: 120-139/80-89 mmHg
Hypertension: ≥140/90 mmHg
Therapeutic Thresholds:
Adults: treat at ≥140/90 mmHg
Elderly (80 and up): ≥150/90 mmHg
elderly has higher threshold due to wear and tear of body and delayed onset of HTN problems
medication may cause more problems and may not be worth it if patient will not reasonably live for long enough for HTN to be a problem
(other guidelines’ categories in ppt)
(AHA has more stringent guidelines focusing on early prevention)
Risk Assessment
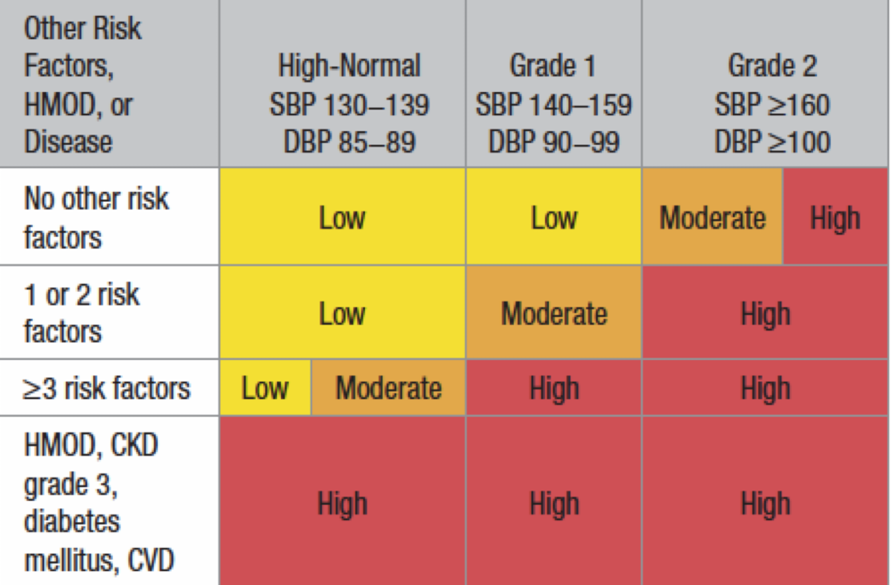
no need to memorize table
Key Trends:
higher # risk factors = higher risk of complications
higher BP = higher risk of complications
presence of organ damage (HMOD) = automatically high-risk for complications
Diagnosis
Diagnosis:
based on elevated office BP readings taken at two separate occasions
a single, markedly high BP reading is sufficient to establish hypertensive crisis
Assessment (Medical History)
Medical History:
Blood Pressure
Risk Factors
Overall Cardiovascular Risk
Signs and Symptoms of HTN or co-existent illness:
Chest Pain
Shortness of Breath (may indicate respiratory problem)
Palpitations
Claudication (extremity pain, may indicate peripheral complications)
Peripheral Edema
Headaches
Blurred Vision
Nocturia
Hematuria
Dizziness
symptoms suggestive of secondary HTN
Assessment (Physical Exam)
Physical Examination:
circulation and heart
pulse rate, rhythm, character
Jugular Vein Pressure (JVP)
may appear distended/bulging or visibly pulsate with heart or lung problem
extra heart sounds
basal crackles
popping sounds at base of lungs, suggesting fluid buildup/edema
other organs/systems
Assessment (Laboratory Exams)
blood tests
urine tests
12-lead ECG (for heart function)
Algorithm for Evaluation of Patient with New-Onset/Uncontrolled Blood Pressure
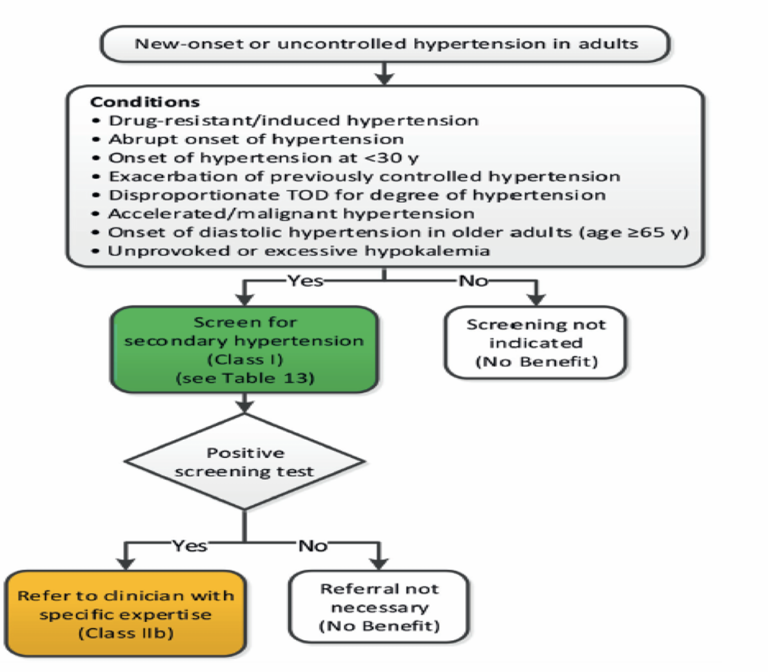
most of the time, patient seeks consultation due to uncontrolled blood pressure due to treatment
screen for possible secondary causes
HTN may remain uncontrolled because underlying condition is not addressed
consider conditions such as malignant hypertension or marked hypokalemia
if these conditions, more serious and targeted investigation is necessary
Office BP Measurement
blood pressure taken inside the clinic
controlled setting, ensures accurate results
most common basis for HTN diagnosis and follow up
diagnosis should be made based on 2 to 3 office visits
at 1 to 4 week intervals
exception: if BP ≥ 180/110 mmHg, with evidence of CKD, diagnosis can be made in one visit (hypertensive crisis)
must be confirmed with out-of-office BP measurement
Interpretation of Office BP Results
< 130/85: remeasure within 3 years (1 year if with risk factors)
130-159/85-99: confirm with out-of-office measurement (if possible), or repeated visits
>160/100: confirm within a few days or weeks
Out-of-Office BP Measurement
BP measured at home, in community pharmacy, or with 24-hour ambulatory blood pressure monitoring (unless performed by a physician)
more reproducible than office measurements
less affected by anxiety due to being observed by professional
better reflect patient’s actual day-to-day BP levels (representative of daily activity)
more closely correlated with HMOD and CV events
may identify white coat and masked hypertension
White Coat and Masked Hypertension
White Coat Hypertension:
elevated BP in the office, normal BP in out of office
seen in 10-30% of cases
intermediate CV risk
Masked Hypertension:
normal BP in office, elevated outside of office
seen in 10-15% of cases
similar CV risk to sustained HTN
masked HTN is worse than white coat HTN
Cardiovascular Risk Comparison
Sustained/Actual HTN and Masked HTN > White Coat HTN > Normotensive Individuals
Medication History Screening
screen patients w/ HTN or at risk for HTN for:
substances which may increase BP
substances that may interfere with BP lowering medications
consider reducing or eliminating substances that raise BP
if substances are required or preferred, treat BP to goal anyway
Substances that Can Increase BP and Management Thereof (Summary)
NSAIDS:
if analgesics are needed, consider alternatives
utilize other routes (topical, local)
Recreational Drugs:
discontinue
Steroids:
can increase BP and induce/worsen other metabolic disorders (ex: DM)
typically do not utilize oral/IV steroids
usually intranasal, topical, inhalation