CT abdomen-pelvis
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
16 Terms
what is the CT abdomen-pelvis
•The CT abdomen-pelvis protocol serves as an outline for an examination of the whole abdomen including the pelvis.
•It is one of the most common CT protocols for any clinical questions related to the abdomen and/or in routine and emergencies.
•It forms also an integral part of trauma and oncologic staging protocols and can be conducted as part of other scans such as CT chest-abdomen-pelvis or can be combined with a CT angiogram.
Non-trauma indications:
•abdominal pain, flank pain, pelvic or inguinal pain
•suspected abdominal or pelvic masses or fluid collections
•primary abdominal tumours or metastatic spread
•infections and inflammatory conditions of the abdomen and pelvis including abscesses
•patients with fever or sepsis of unknown origin
•bowel obstruction
•postoperative follow-up
•pre and posttransplant evaluation
CT abdomen LMP
A conservative approach used by some radiology facilities is to apply a 10-day rule only for examinations with the potential to deliver a high dose to the lower abdomen and pelvis, such as barium enemas and CT of the abdomen or pelvis.
These facilities use a 28-day rule for all other examinations.
How is creatinine affected by intravenous contrast
•Creatinine is a product of the break down of creatinine phosphate within the muscles & is filtered by the kidneys - any renal compromise = Creatinine rises
•Serum creatinine levels can be used to calculate an estimate of kidney function = eGFR (estimated glomerular filtration rate)
•Normal GFR varies according to age, sex, and body size, and declines with age.
•Point-of-care (POC) creatinine devices allow rapid measurement of creatinine levels and calculation of estimated glomerular filtration rate (eGFR).
•The focus of this assessment is POC creatinine testing to assess kidney function before people have intravenous contrast for CT imaging.
•Intravenous iodine-based contrast agents used in CT scans can cause acute kidney injury (AKI), particularly in people who are at high risk and those with known kidney dysfunction.
•If a person has a low eGFR, intravenous hydration can be offered before the scan to reduce the risk of AKI.
•If a person does not have a recent eGFR measurement, their CT scan should be cancelled and rescheduled while a creatinine test is processed in the laboratory.
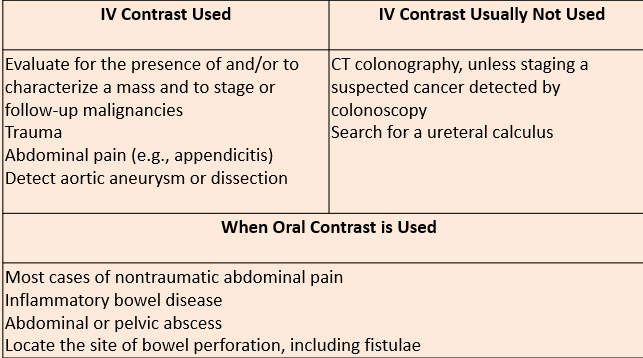
when is IV contrast generally used/not used
what are contrast injection considerations
•Non-contrast (optional) – plays a role (see other lectures CTIVU and CTC)
•Biphasic arterial ± venous acquisition
–contrast volume: 70-100ml (0.1 mL/kg) with 30-40 mL saline chaser at 3 mL/s
–early arterial phase: minimal scan delay (15-25 seconds – upper extremity vein) or bolus tracking: abdominal aorta - immediately
–portal venous phase: 70-90 seconds after contrast injection (upper extremity vein) or 50-70 seconds after bolus tracking
•Single acquisition with a monophasic injection (venous phase):
–contrast volume: 70-100ml (0.1 mL/kg) with 30-40 mL saline chaser at 3 mL/s
–portal venous acquisition: 70-90 seconds after contrast injection (upper extremity vein)
•Single acquisition with a biphasic injection or split bolus
–70 ml contrast media at 3 mL/s
–50 ml contrast media and 30-50 ml saline chaser at 4 mL/s starting 30 sec after contrast injection
–portal venous acquisition: 70-90 seconds after contrast injection (upper extremity vein)
what is the early arterial phase
•The early arterial phase is a contrast-enhanced CT series in which the contrast is still in the arteries and has not reached the organs and other soft tissues.
•The acquisition time depends on the intravenous device (central or peripheral), the concentration of the contrast medium, and the injection rate.
–time from injection through an upper extremity vein: 15-25 seconds
–time from bolus tracking: immediately
•The early arterial phase offers optimal vessel demarcation and allows the detection of vascular pathology (e.g. aortic dissection, aneurysms, tumours of blood vessels)
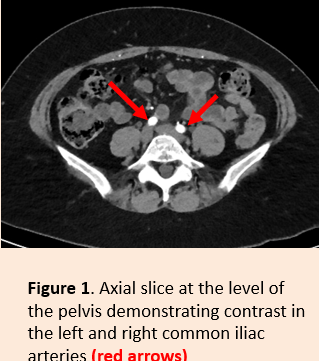
what does the early arterial phase in the pelvis look like
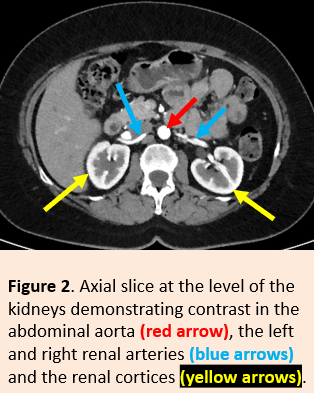
what does the early arterial phase in the kidneys look like
what is the late arterial phase
•The late arterial phase (or early venous portal phase) is a contrast-enhanced CT series in which there is an optimal enhancement of structures that get their blood supply directly from the arterial system.
•The acquisition time depends on the intravenous device (central or peripheral), the concentration of the contrast medium, and the injection rate.
–Time from injection through an upper extremity vein: 30-40 seconds (30 seconds at an injection rate of 4 ml/s)
–Time from bolus tracking: 15-20 seconds
•The late arterial phase offers optimal enhancement of the pancreas, spleen, and kidney outer cortex.
•Allows the detection of:
–pancreatic lesions (adenocarcinoma and hypervascular pancreatic lesions),
–hypervascular liver lesions, and
–hypervascular splenic lesions.
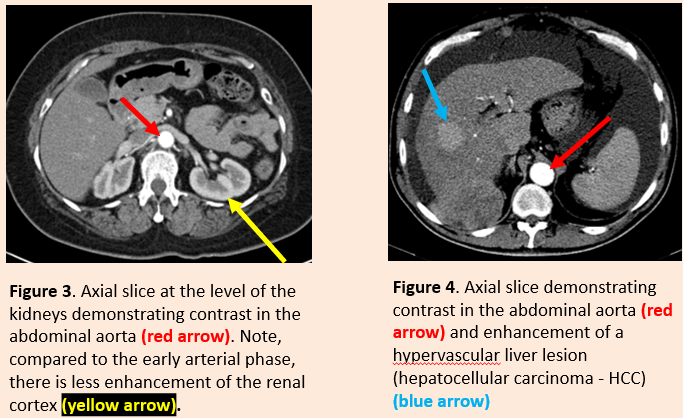
what does the late arterial phase look like
what is the portal venous phase
•The portal venous phase (also known as the late portal phase or hepatic phase) is a contrast-enhanced CT series that has the following characteristics:
–liver parenchyma is at its peak enhancement
–portal vein and hepatic veins are completely enhanced
•The acquisition time depends on the intravenous device (central or peripheral), the concentration of the contrast medium, and the injection rate.
–time from injection through an upper extremity vein: 70-90 seconds, (at an injection rate of 4 ml/s)
–time from bolus tracking: 50-70 seconds
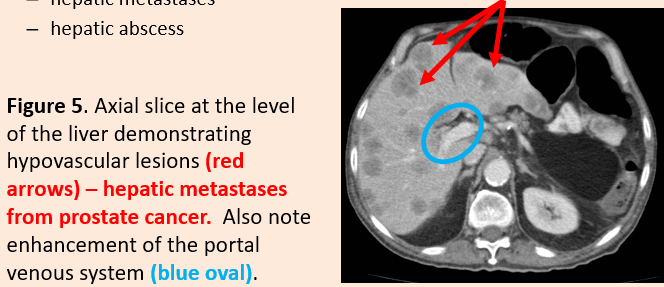
•Offers the best hepatic enhancement for the detection of:
–hypovascular hepatic lesions
–hepatic metastases
–hepatic abscess
what does the portal venous phase look like
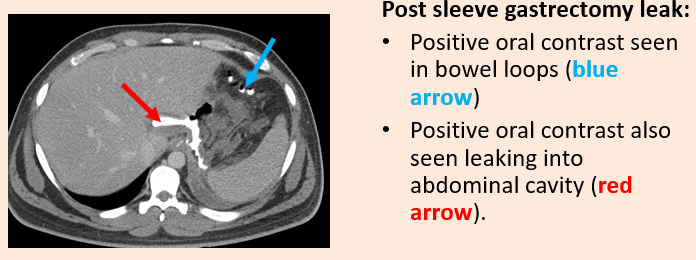
what is positive oral contrast medium
•Enteric (oral) positive contrast media (e.g. gastrografin) can be given to patients before their CT exam to improve its diagnostic accuracy.
•Historically, a combination of oral and intravenous contrast media were always given prior to a CT abdomen.
•Contemporaneously, improved CT scanners mean that oral contrast agents are no longer routinely used but remain in widespread use for a narrower range of indications.
•Water-soluble contrast agents are generally preferred to avoid the risk of peritonitis that may occur when barium sulphate contrast medium leaks into the peritoneal cavity. Diluted 5-10% solution.
Indications: usually/often given when the following is suspected:
•bowel perforation & GI fistulae
•interloop fluid collections
•CT colonography – see later lecture
•Most cases of nontraumatic abdominal pain
•Inflammatory bowel disease
•Abdominal or pelvic abscess
•Locate the site of bowel perforation, including fistulae
what are the contraindications for positive oral contrast media
Contraindications: Oral positive contrast media is usually avoided in the following:
•CT enterography (neutral contrast media may be given) – see later lecture – small bowel imaging
•Suspected mesenteric ischaemia
•Suspected GI bleeding: may obscure the acute blood/contrast leak
•CT abdominal angiography
•Acute blunt trauma
•Urolithiasis (kidney stones)
•Aspiration risk (relative contraindication)
[Note: CT enteric contrast media are most commonly administered by mouth, although may also be given by way of an enteric catheter (e.g. nasoenteric, PEG, etc.), via a stoma (e.g. ileostomy) or per rectum.]
why is timing of oral contrast media important
•The timing of administration of the contrast media is also clearly important.
•If given too long before (or too close to) the time of the CT examination then it may have already passed by (or not yet reached) the area of interest.
•There is a certain art to getting the timing right as speed of bowel transit varies considerably, especially in disease states.
•Dependent upon patient/ward to get timing right.
what is neutral contrast medua
•In some patients, it is helpful to give a neutral contrast agent, e.g. water, to distend the stomach/bowel and make it easier to see the stomach/bowel wall.
•This is particularly helpful if there is a clinical concern of bowel ischaemia.
•Neutral oral agents may also be used for CT enterography (see later lecture – small bowel imaging)