637 Heart Rate Variability and Exercise Testing
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
What is heart rate variability (HRV)? Variability of sinus rhythm vs. arrhythmia? What system controls HRV? What is HR recovery dependent on?
Time measured between one heartbeat to the next heartbeat, relates to recovery time
Measure of variation in R to R intervals = response of heart to stimuli (exercise, stress, emotions)
Sinus rhythm: variability <0.12 sec
Sinus arrhythmia: variability >0.12 sec
Controlled by the autonomic nervous system
PNS - facilitates HR at rest and can slow or stop HR
SNS can suppress PNS or increase PNS reactivity
HR recovery is dependent on PNS reactivation and SNS withdrawal
If a heart rate stays high what does this mean for HRV?
In sympathetic overdrive, low HRV
When does HRV decrease and increase? When does it improve?
HRV decreases with age, heart disease, MI
Yielding progressively higher RHR, prolonged HRR, prolonged SA node conduction time, smaller difference between RHR and intrinsic HR with age and progression of disease
HRV increases with
Greater difference between RHR and intrinsic HR
High variability reflects increased adaptability of the body
Research has shown correlation between greater HRV and reduced stress w/ increased happiness
HRV improves with
Routine exercise and healthy diet (not about reaching max HR)
Tools for managing stress, depression, and anxiety
What does heart disease do to HRV? What does this mean?
Heart disease reduces HRV which means its less adaptable to stress and changes
How does HRV relate to sympathetic and parasympathetic activation?
HRV is LOW in sympathetic activation with increased HR and cardiac output, but HRV is HIGH in parasympathetic activation
Sympathetic activation impairs HR regulator (vagus n.)
As HR increases, what happens to HRV? What is the relevance of this?
HRV reduces as HR increases
Cardiac pathologies should be treated prior to gathering HRV data (murmurs, arrhythmias)
HRV can predict outcomes w/ viral infections i.e. COVID-19 (conditions that keep HR high), long COVID, inflammatory conditions i.e. DM
HRV has relation to executive functioning performance in young and old adults - biomarker for healthy aging
What are factors that impact HRV? How does exercise, day vs. night changes, inflammation and infection, social stress and noise, CO exposure, alcohol and smoking, anxiety, depression, stress, gender, and ethnicity impact HRV?
Physiologic
Exercise lowers HRV in short term; HRV lower during the day, higher during the night (increased PNS activation)
Pathologic
Inflammation and infection reduce HRV
Environmental
Social stress and noise increase HRV; CO exposure reduce HRV
Lifestyle
Alcohol consumption (greater than 1-2 daily), chronic smoking is associated with reduced HRV
Psychologic
Anxiety, depression, and stress is associated with reduced HRV
Genetic
Greater HRV in women vs. men
Greater HRV in afro-americans and euro-americans
How does eustress impact HRV?
Improves HRV, people need social connection and isolation can have a negative impact
What does exercise testing involve? Modes of exercise? Informal testing forms?
Exercise testing involves systematically and progressively increasing O2 demand and evaluating the response to the increased demand
Modes:
Walking up and down stairs
Exercising on a stationary bicycle
Using arm or wheelchair ergometry
Walking or jogging on a treadmill at variable speeds and inclines
Walking a specific distance i.e. 6MWT
Informal testing
12 MWT, Cooper’s 12-min run, pulse recovery test, 1.5 mile run
What are reasons for stress testing?
Unstable angina - emergent!
Determine CAD blockage %
Symptomatic (chest pain, SOB on exertion)
Screen for heart & lung conditions - proactive!
Ventilatory status
Pre-surgical check off
How do clinicians monitor pts during exercise testing? What can it detect?
Continuous monitoring through ECG and periodic monitoring of HR & BP, pt’s sxs reported or observed i.e. RR, SOB, heart & lung sounds, expired gas analysis
Can detect arrhythmias (PAC, PVC, HB, etc.) and ischemia (ST segment abnormality)
*What are indications for exercise/stress testing?
Evaluation of chest pain suggestive of CAD
Evaluation of atypical chest pain
Determination of prognosis and severity of CAD
Evaluation of the effects of medical or surgical therapy or intervention
Evaluation of arrhythmias
Evaluation of HTN w/ activity
Assessment of functional capacity
Screening to provide an exercise prescription
Providing motivation for a lifestyle change to reduce risk of developing CAD
What does endurance exercise testing used to predict and diagnose?
Predict VO2max and diagnose exercise intolerance
How does a maximal test impact RPE and RER? How long does it usually take? Goal? What will the end of test represent? What population is it most appropriate for? Challenging factors?
RPE and RER will steadily increase (consistent with return to daily life)
10-20 min
Goal: increasing intensity
End of test will represent max a body can produce
Males >40 yr old, females have higher % of false negatives
Role of encouragement, interpretation of St segment, use of handrails, strict adherence to protocols
How does a submax test impact RPE and RER? How long does it usually take? Goal? What will the end of test represent? What intensity do you want to work below?
RPE and RER will plateau
30+ min
Goal: steady state (85% of HRmax, if HR increases, intensity will be reduced)
End of test will represent % of max a body can produce
Work below 2-word dyspnea and SOB
How does the use of handrails affect the maximal test?
Changes in posture
+ vent status
Increased SOB
Whats the main difference between maximal and submax test?
Max ramps up quickly, shorter duration, see the max a body can produce, RPE and RER increase steadily, increasing intensity
Submax ramps up slower, longer duration, see the % of max a body can produce, RPE and RER plateau, steady state
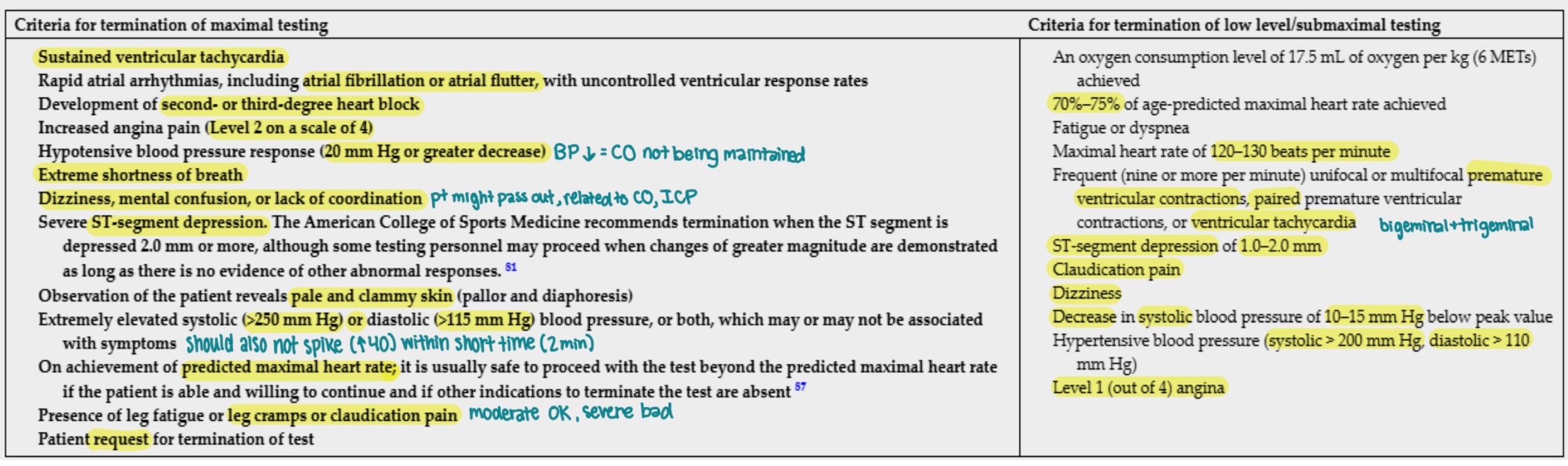
When is low level testing performed? *What are contraindications to low level testing? BP?
Performed after MI or CABG, sometimes as early as 3-4 days after
5 MWT or gait speed test
Contraindications
Unstable angina or angina pectoris at rest
Severe HF (decompensated HF - overt LVF w/ pulmonary rales & S3 heart sounds)
Serious arrhythmias at rest
2nd or 3rd degree HB (signifies decreased CO, backflow, generation of clots)
Disabling MSK abnormalities (NWB status from displaced fx, amp.)
Valvular heart disease
*BP >180/105 mmHg*
Patient refuses to sign consent form
What types of pts are more likely to experience adverse cardiac events with exercise testing?
Pts w/ reduction in systolic BP, HR, angina, and/or increased frequency of arrhythmias during testing
What is the gold standard of exercise testing? Issue with it? What factors do you consider when making an appropriate test selection?
VO2 maximal test
Higher risk of complications
Consider:
Accuracy required? How close to VO2 max does it need to be? (consider home support, athletic needs)
Expected fitness level
Test duration
Level of duration
Localized muscle fatigue (knee buckling)
Below workload of sxs (angina) (walking vs. running provoking pain)
Airway limitations (asthma, acute bronchitis)
Locomotion, balance, cognitive impairments
*What are criteria for termination of maximal vs. low level/submax exercise testing?
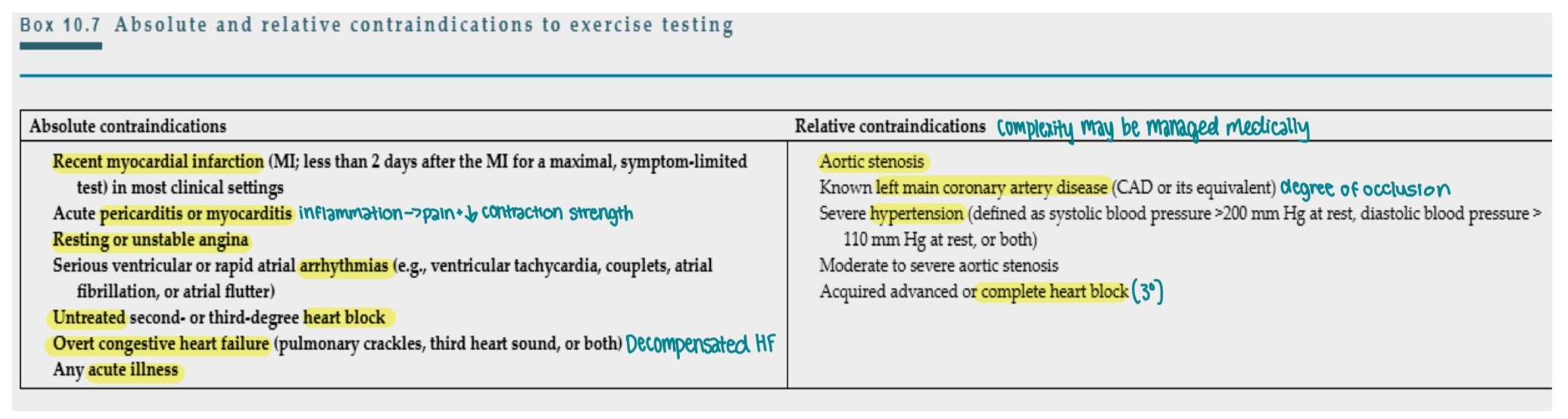
What are absolute vs. relative contraindications for exercise testing?
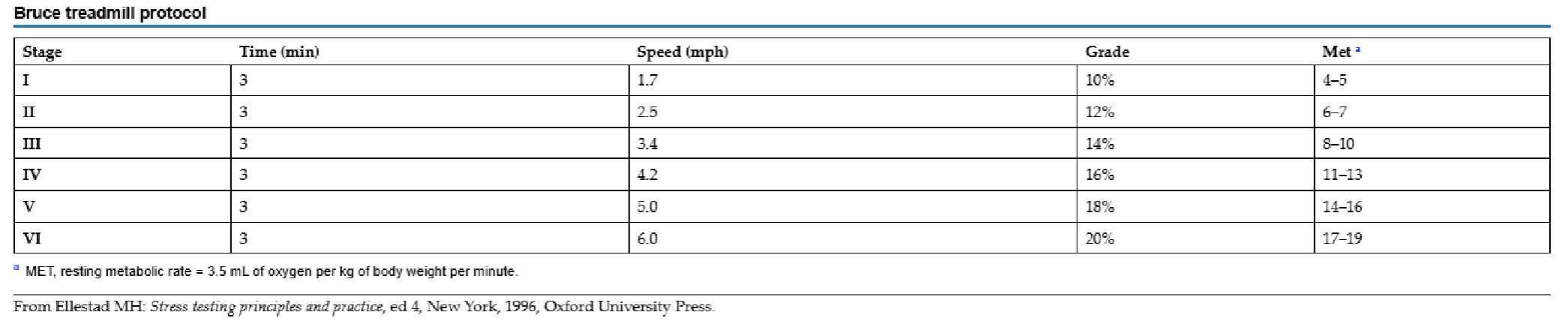
What is the protocol for exercise testing? Bruce treadmill protocol?
12 lead ECG prior to testing, sxs hx, risk factor analysis for CAD, resting BP, HR, and heart and lung auscultation
Bike to treadmill w/ continuous monitoring or ECG, workload increased w/ specific protocol, most tests are sx limited or unitl 85% of APMHR
Treadmill loud, impacts auscultation
Bike challenges muscle groups that are not as trained as muscles used for walking in deconditioned populaiton
Bruce treadmill protocol most commonly used and can calculate functional aerobic impairment
Starting speed 1.7 mph (average time of test 6-12 min for deconditoned pt)
*What is the interpretation of exercise testing results?
Positive >1.0 mm horizontal or down-sloping ST-segment depression
Equivocal >0.5 but <1.0 mm horizontal or downsloping ST-segment depression or more than 1.5 mm upsloping depression
Negative <0.5 mm horizontal or downsloping St segment depression
What does it mean if an ST segment depression occurs early in the exercise test vs. at the peak of exercise?
an indicate more severe coronary blockage, ischemia
What is heart rate recovery (HRR) in exercise testing? What is it predictive of?
Difference in peak HR and HR after 1 minute
Predictive of mortality
What can ventilatory gas analysis identify? What does it measure? When can a patient not continue w/ activity/exercise with dyspnea?
Can identify ventilatory, cardiac, and metabolic limitations of a patient
Measures volume of expired air and concentration of O2 and CO2 in expired air
Dyspnea occurs w/ minute ventilation (VE) divided by maximal voluntary ventilation (MVV) is greater than 50%; if ratio > 90% pt will not be able to continue
What does radioactive nuclide perfusion imaging do? What are the two common perfusion trackers? What are limiting factors?
Agents taken up by myocardium based on coronary blood flow or restricitons
Thallium and technetium
Helpful for female pts but cost and skill of interpreter are limiting factors
When is a pharmacological stress test warranted?
Submax test wouldn’t reach threshold
What is the adenosine or dipyridamole walk protocol?
Combined low level treadmill exercise during infusion can reduce risk of adverse events and effects (flushing, nausea, and headache) w/ exercise testing while increasing diagnostic accuracy
What is ergonovine stimulation?
Coronary artery spasm performed in cardiac catheterization lab can cause sx during a spasm if narrowing is present, relieved by vasodilators (diagnostic if sxs reduce)
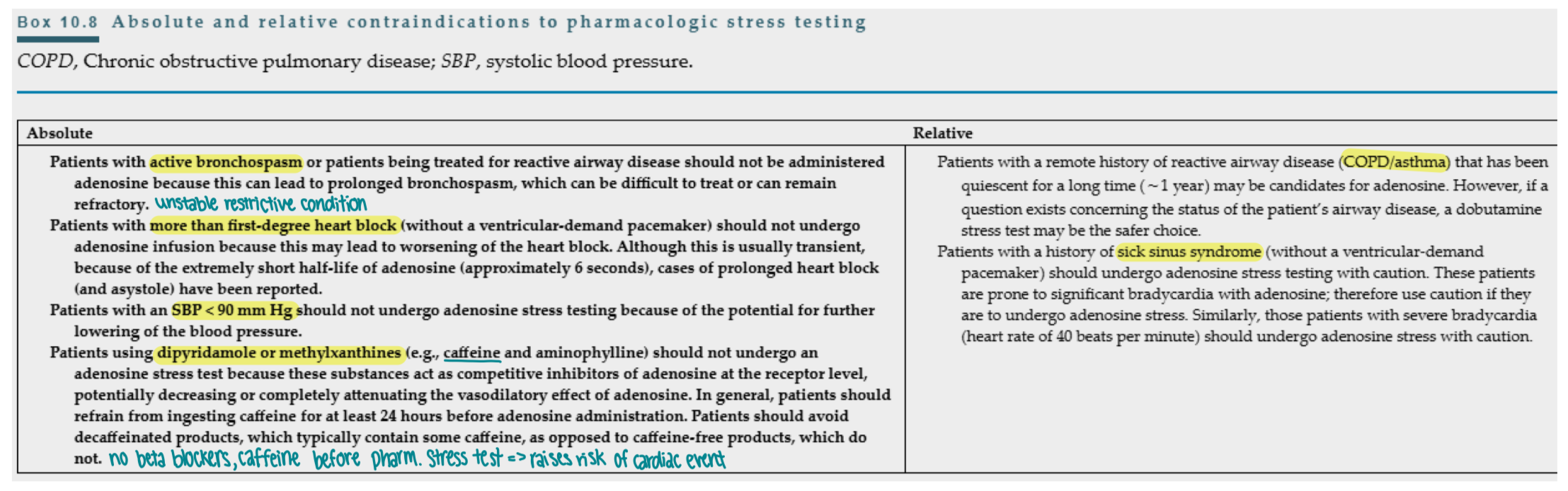
What are absolute and relative contraindications to pharmacologic stress testing?
What is included in the evaluation for exercise testing?
Establish safety for exercise participation
Receive MD referral
Physical exam
MSK, neuro, cardio, pulm
Auscultation
Peripheral vascular status
Measures: resting ECG, HR, BP, pulse ox, PFT
Functional mobility
What are the steps for the ACSM model?
Determine RF for CV disease
HTN, DM, pre-diabetes, kidney disease, UTI/KI hx, low levels of PA, obesity, hyperlipidemia, smoking, sleep apnea
Symptomatic
Fluid retention (figure 8 edema, daily weight), dyspnea, chest pain, heart skipping a beat, palpitation, difficulty swallowing, unexpected and intense fatigue, family hx
Vital signs
High BP, high resting HR
ACSM determines max, submax, or low level test
What is the cutoff value for hemoglobin as a red flag for OOB activities?
less than 8mg
What are the normal values of the cardiac enzymes?
Troponin <0.3 ng/mL
CK-MB <5%
What is a normal BNP value?
< 100 pg/mL
What are the normal lipid levels?
Total cholesterol <200 mg/dL
LDL <100 mg/dL
HDL >40 mg/dL male, >50 mg/dL female
Triglycerides <150 mg/dL