HSCI 211 Part 1
1/83
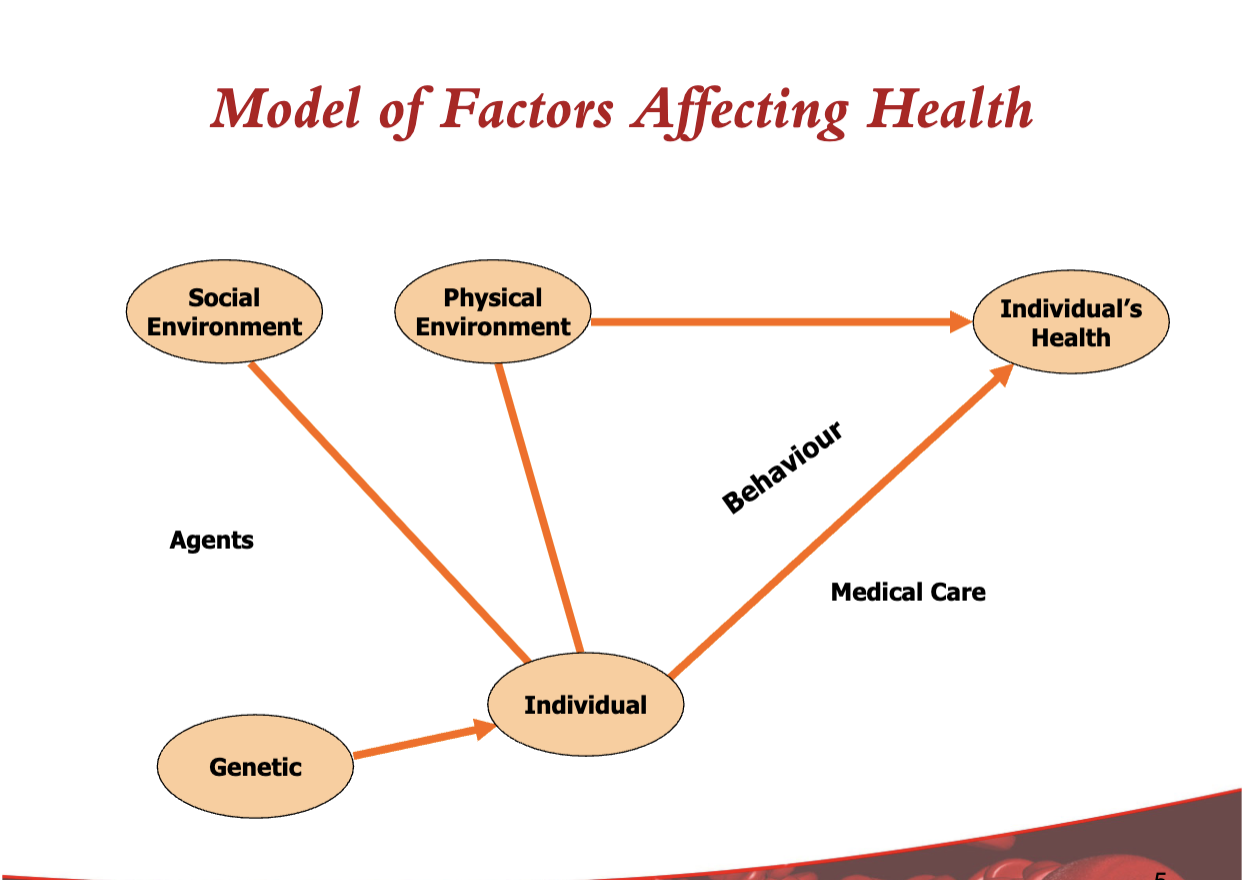
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
What does chronic mean?
prolonged, long-lasting, long-term, often but not necessarily implying incurable.
what does chronic disease mean?
Any disease that is long-lasting or permanent.
often refers to an illness episode greater than 6 weeks.
what are transmissible agents?
bacteria, virus, etc. that can be spread from one host to another, causing illness.
It is communicable.
What is chronic disease control?
usually refers to conditions not caused by transmissible agents.
therefore it is a non-communicable disease.
doesn’t travel from one person to another.
what is incidence?
the number of new cases in a specific time period.
risk of developing it.
What is prevalence?
the number of existing cases at a given time.
includes new and old cases showing the burden/extent of the disease.
What are the causes of chronic disease?
They are complex
simple: baking a cake.
complicated: sending a rocket to the moon (difficult but there are sequences of events that get us there).
complex: raising a child.
what is epidemiology?
the study of the distribution of disease and its determinants.
from the word epidemic
what are the two level of analysis epidemiology?
compare individuals
compare populations
What is compare individuals?
can learn about the disease and how to help these individuals.
what is compare populations?
it is comparing groups of individuals
you can see if there are some underlying conditions (determinants) in the whole population that affect this ”condition”.
what is the epidemiologic transition: the stages?
Age of pestilence and famine
there are high death rates and birth rates
receding pandemics
low death rates, but high birth rates.
degenerative and chronic disease
low death rates and low birth rates
what are early health improvements?
significant reduction in mortality from infectious disease (mostly in young people - infants and children)
improvements in water and sanitation (England and Wales mid-19th century)
immunization (early 20th century)
Antibiotics (mid 20th century)
what are the population pyramid shapes?
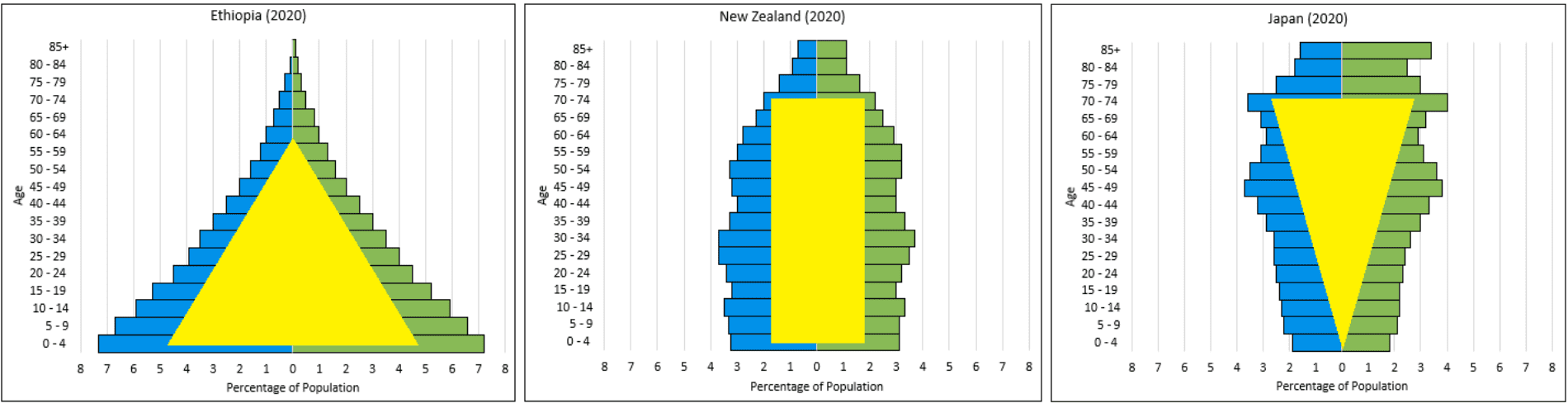
what are the disease patterns: developed countries
low birth rates
rectangular population pyramid
(a stable population with slow or no growth)
predominantly chronic disease, which are decreasing.
These diseases are becoming less deadly due to better prevention, treatment, and healthcare access.
what are the disease patterns: high mortality developing countries?
high death rates
high birth rates
population pyramid is triangular
(a rapidly growing, young population, typical of developing countries, with a wide base of many children, a rapid decrease in numbers in older age groups (high death rates/low life expectancy), and a narrow top, indicating fewer elderly people.)
high burden of infectious disease - particularly in children
what are the disease patterns: low mortality developing countries
lower death rates
high birth rates
population pyramid is becoming rectangular
(stable)
double burden of disease (infectious and chronic)
what is population health?
the health outcomes of a group of individuals, including the distribution of such outcomes within the group.
what are the goals of population health?
to maintain and improve the health status of the entire population
to reduce the inequities in health status between population groups.
what are some population health questions?
How can we tell that Vancouver/Canada has a health problem? How can we make that “diagnosis”? (do we have to look at other groups)
What should Vancouver/Canada do about it? (“prescription”) How do we decide?
How is this improvement implemented? Who is involved?
How can we tell if Vancouver/Canada is getting better?
what are the steps in addressing a health problem?
examination
diagnosis
prescription (deciding on the intervention/treatment) or policy development
communication of the decision
service provision
providing rehabilitation or health services.
what has fuelled the epidemic of chronic disease?
the globalization of risk
(chronic diseases are spreading worldwide)
the transmission of unhealthy behaviours has proceeded with great rapidity to developing countries.
countermeasure are absent- both at a policy level and a sophisticated population/public health infrastructure.
(developing countries don’t have strong systems to fight these problems.)
What is the globalization of risk?
governments have underdeveloped:
policy responses
health and public health systems
economic development is usually the priority even before people - uneven wealth distribution
political and geographic boundaries cannot cope with modern communications where ideas and culture rapidly transfer
demands a global response
regulate international trade
share and disseminate interventions
policies on recruiting professionals.
does where you live matter?
Yes, where you live matters because exposure to health risks, government regulation, public health infrastructure, and inequality vary by location, shaping how globalized health risks affect populations.
Which of the following is not correct regarding the epidemiologic transition?
a. The epidemiologic transition indicates that populations will transition to higher mortality from chronic diseases.
b. Increased cardiovascular disease rates are associated with increased urbanization.
c. The globalization of risk infers that populations around the world will, over time, come to face the same risk exposures.
d. Developing countries are associated with low birth rates and low mortality rates.
d. Developing countries are associated with low birth rates and low mortality rates.
birth rates are high while mortality rates high or lower.
what are the types of prevention?
Primordial
primary
secondary
tertiary
what is primordial prevention?
actions or measures that inhibit the emergence and establishment of environmental, economic, social and behavioural conditions, cultural patterns of living, etc.
Known to increase the risk of disease.
what is primary prevention?
protection of health by personal or communal efforts, such as enhancing nutritional status, immunizing against communicable diseases and eliminating environmental risks.
alteration of susceptibility or reduction of exposures of susceptible individuals.
what is secondary prevention?
a set of measures available to individuals and communities for the early detection and prompt intervention to control disease and minimize disability.
early detection and treatment of disease.
what is tertiary prevention?
measures aimed at softening the impact of long-term disease and disability by eliminating or reducing impairment, disability and handicap; by minimizing suffering and maximizing potential years of useful life.
alleviation of disability resulting from disease and attempts to restore normal functioning.
what is a risk factor
presence of a behaviour or physiological parameter that increases the chances of having heart disease
no single factor causes heart disease
a risk factor must be:
associated with a disease - greater exposure, greater risk
makes sense in a biological way
reducing risk factor reduces disease
what are the cardiovascular disease risk factors?
non-modifiable
age
sex
family history
modifiable
cholesterol (blood lipids)
blood pressure
diabetes
smoking
sedentary behaviour
poor nutrition
obesity
stress/depression
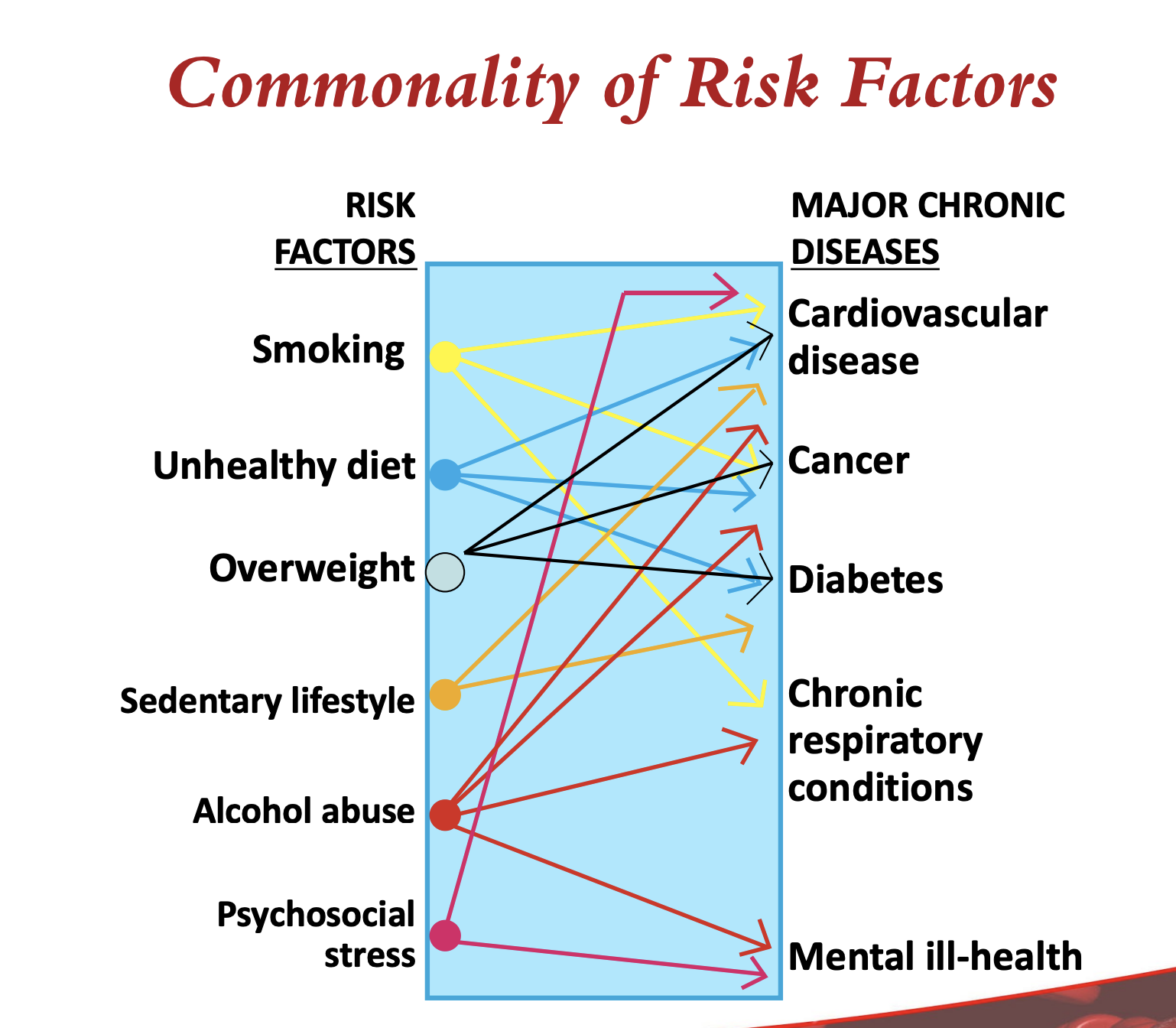
is there a commonality of risk factors?
there is a major commonality of risk factors leading to many major chronic diseases.
According to Sir Geoffrey Rose, what was the dominant health strategy in his time?
a clinical strategy - physician strategy
In Rose’s time, when did people typically receive medical intervention?
After they became sick and were already patients.
At what stage of disease did intervention usually occur in Rose’s time?
When the disease was entrenched and often well advanced.
How important was prevention in Rose’s time?
Prevention was not an important concept.
What does it mean that “patients are sometimes created” in Rose’s strategy?
Conditions like high blood pressure label people as patients even before symptoms.
What were public health strategies mainly focused on during Rose’s time?
Education and targeting individuals who were considered at risk.
What is the concept of normal?
Normal refers to those who fall below an action level and make up most of the population within the distribution curve.
What role does the distribution curve play in defining “normal”?
It shows that most people fall within a certain range, which is considered normal.
what else does normal represent?
represents what is common for that population.
common characteristics are therefore assumed to be acceptable or normal within the population.
what were Rose’s questions?
Why do some individuals have hypertension?
Why do some populations have more hypertension?
What causes the case?
What causes the incidence in a population?
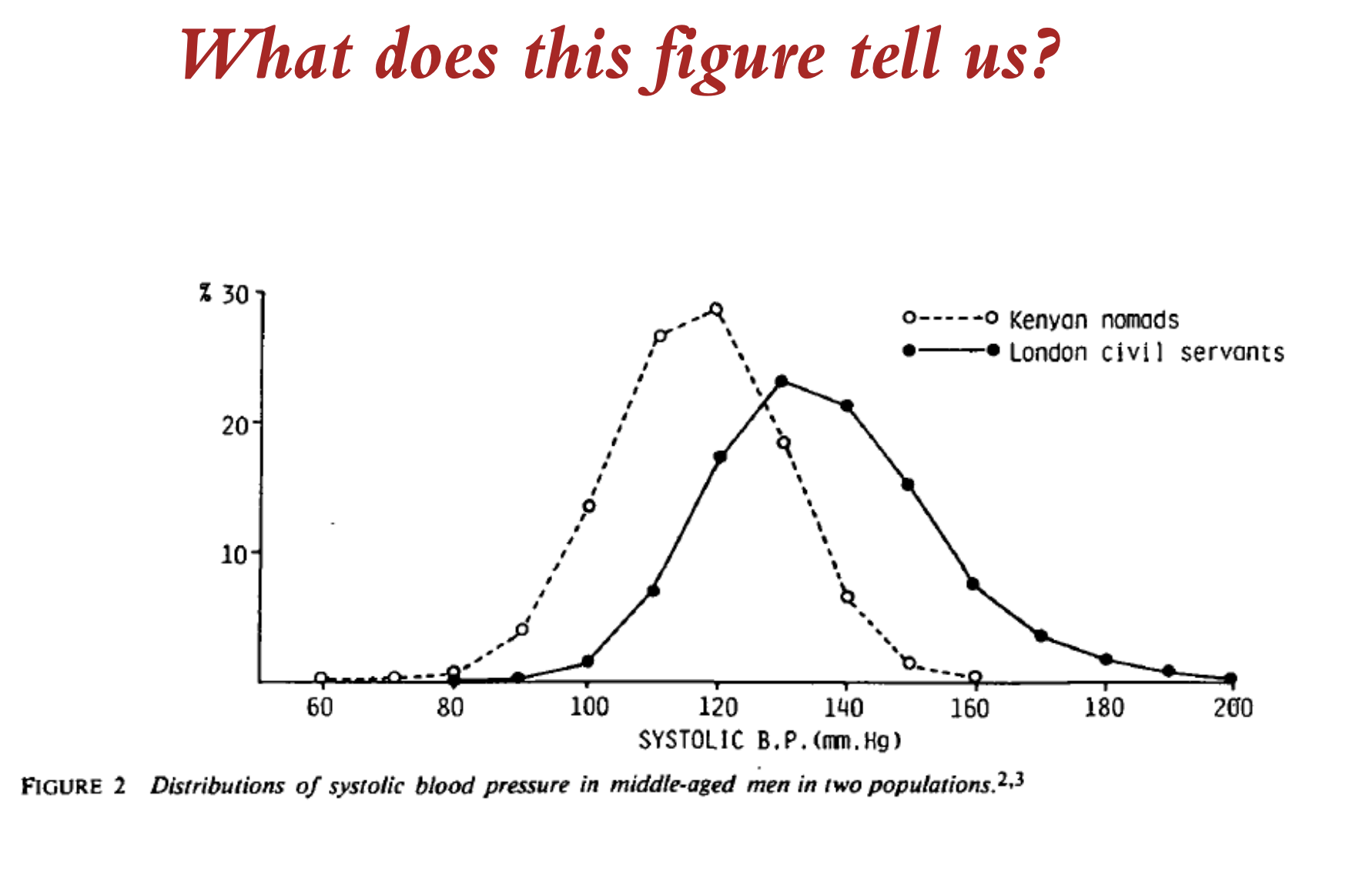
what does this figure tell us?
the distribution of systolic BP in two populations
What can we see in the figure?
In both populations if you only ask what is the cause of the cases then the answer will be much the same – genetics, environment, behaviour
Looked at in isolation the greater question is obscured – Why is there much more elevated BP in London and much less in Kenya?
Some mass influence is operating at a population level
Thus a very narrow clinical focus that looks only at the patient (individual or many individuals) misses the significance of the cause of incidence in a population
What is ‘normal’ is not the same for both populations.
what can we conclude from the figure?
We need to be able to observe at population levels and not just individual levels
To find the determinants of incidence and prevalence rates, we need to study the characteristics of populations, not characteristics of individuals.
Accepted normal values may not be normal and they may not be okay
Curves of risk can be shifted
what is teh concept of risk?
High Risk (HR) – the relative risk of death is high due to the presence of the risk factor or the disease process
There are far fewer people in the HR group – the majority are not in the HR group
The absolute risk – while the actual # of deaths is high in the HR group it accounts for very few of the population deaths due to this disease or risk factor
A large number of people exposed to a lesser or moderate risk leads to the majority of cases in population
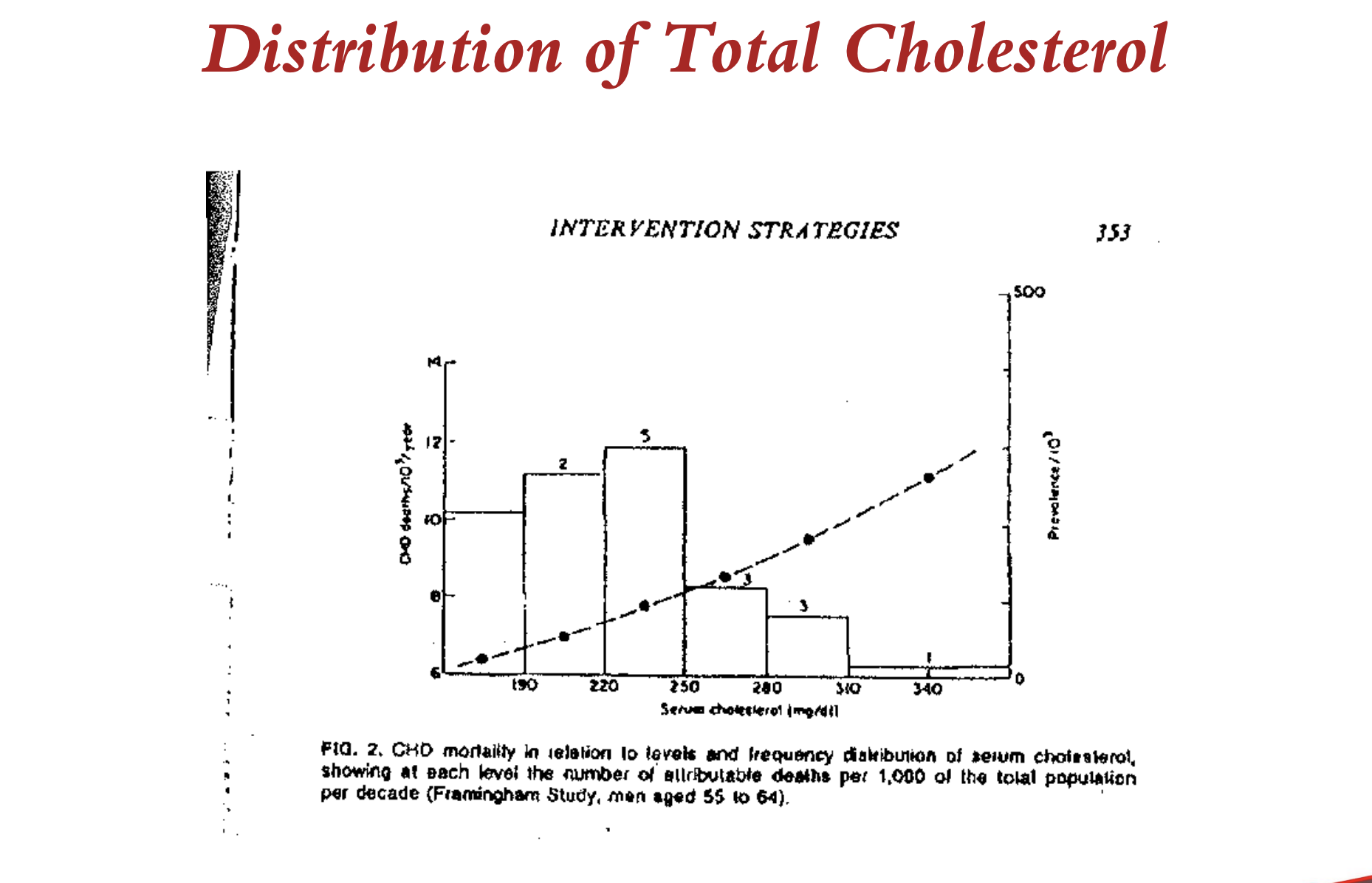
what do we learn from this cholesterol distribution curve?
Most of the excess deaths occur in the population in the middle of the curve at moderate values
There is high mortality at the high levels but there are far fewer people
In a population a large number of people at smaller risk will give rise to more cases of disease than a small number of people at high risk
What is the case for a population strategy?
If our health system focuses only on those who are at high risk or are sick; if we employ only clinical strategies we will miss the majority that contribute most to the overall mortality
A population preventive strategy that seeks to move the entire population distribution curve to the left is essential
Therefore a community (society) that wishes to make an impact on a disease or condition must employ a two pronged strategy – a high risk, clinical intervention accompanied by a population strategy to influence the segment that accounts for the majority of the cases
What is the population prevention strategy?
Control the determinants of incidence
Lower mean levels of risk factors
Shift the distribution of exposure in a more favourable direction
The mechanisms – mass environmental controls and alter social norms of behaviour
what are the advantages of a population strategy?
Large potential for the population
Behaviourally appropriate
What are the limitations of a population strategy?
A small benefit to each participating individual – this is the ‘prevention paradox’
Poor subject motivation
Poor physician motivation
Benefit-risk ratio problematic to demonstrate- potentially costly
See obstacles in: Fineberg et al. JAMA 2013.
What is said about interventions?
“an intervention which brings much benfit to the population offers little benefit to each participating individual”
What is the population approach?
Both populations and high risk groups
Creates environments supportive of health
Focuses on health promotion and disease prevention
Works through partnerships and coalitions
Includes intersectoral and interdisciplinary groups and organizations
Uses healthy public policy development and community mobilization as major tools.
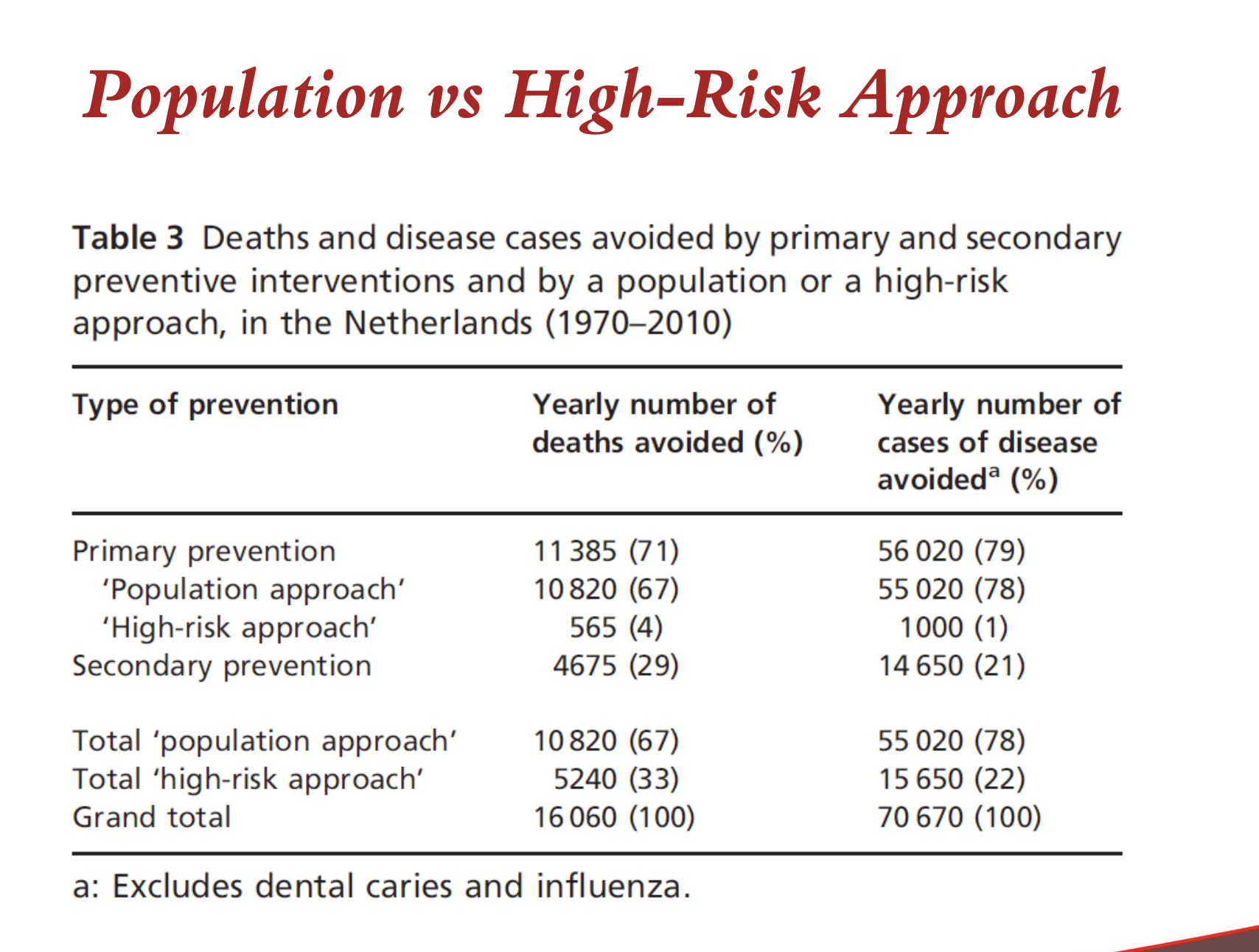
what does this figure tell us?
total population approach’s yearly number of deaths avoided number doubles.
What did Rose lead us to an understanding of?
Observing populations to understand cause of incidence and prevalence is essential
Normal is not necessarily okay
Risk distribution at a population level can be improved (move the curve)
Most cases do not arise from the high risk group
To improve health need a population health strategy to complement a high risk strategy
What can we conclude?
Since most cases arise in the middle of the curve
Since population curves can potentially shift
Since small changes which occur over an entire population produce great population benefits (though small individual benefits)
…a population health approach is essential if risk is to be reduced and consequently morbidity and mortality
Why is it important to compare populations with respect to health, disease and disease risk?
a. Different populations have different risk exposures and therefore may present with different risk factor levels.
b. It is not important as ‘normal’ is based on the population in which you are studying.
c. Answers a and d.
d. We can learn that ‘normal’ in one population, is not ‘normal’ in another.
c. Answers a and d.
lecture question: On a global scale, how does where you live affect the health of the population?
On a global scale, where you live determines the types of health challenges a population faces based on their stage in the epidemiologic transition. Developed countries generally experience a high prevalence of chronic diseases, whereas high-mortality developing countries face a heavy burden of infectious diseases, particularly among children.
The health of a population is also affected by the following factors related to location:
• The Double Burden of Disease: Many developing countries now face both infectious and chronic diseases due to the rapid globalization of risk and the adoption of unhealthy behaviours from other cultures.
• Urbanisation and Diet: Living in urban areas is associated with increased rates of cardiovascular disease and significant changes in dietary patterns, such as increased energy intake from animal sources and fats.
• Environmental and Social Determinants: Geographic location exposes people to different risk determinants; for example, the Ni-Hon-San study demonstrated that cardiovascular disease rates for the same ethnic group varied significantly depending on whether they lived in Japan, Hawaii, or San Francisco.
• Regional Norms: What is considered "normal" for a physiological parameter, such as blood pressure, changes between populations, meaning a healthy level in one region (like Kenyan nomads) may not be the same as in another (like London civil servants).
lecture question: Why is it important to look at different populations to determine what is ‘normal’?
It is important to look at different populations to determine what is ‘normal’ because what is considered "normal" in one population is often not the same in another.
The sources highlight several key reasons for this approach:
• "Normal" is not necessarily healthy: In a public health context, "normal" often refers to what is common or average within a specific distribution curve. However, comparing different groups reveals that these accepted normal values may not be healthy or "okay" in an absolute sense.
• Identifying Mass Influences: Looking only at individuals misses the significance of the cause of incidence in a population. For example, the Rose study compared systolic blood pressure in Kenyan nomads and London civil servants; it found that while the causes for an individual's high blood pressure (like genetics) might be similar in both groups, a "mass influence" was operating at the population level to make the London average much higher.
• Different Risk Exposures: Different populations face different risk factor levels and environmental determinants. To find the true determinants of disease prevalence, it is essential to study the characteristics of the population as a whole rather than just the characteristics of individuals.
In summary, studying multiple populations allows researchers to understand how to shift the entire distribution of exposure in a more favourable direction, rather than just treating "sick individuals" who fall at the high-risk end of a single population's curve.
lecture question: Explain the trend in global disease changes. What may account for this?
The global trend in disease is defined by the epidemiologic transition, which is the shift from an age of infectious "pestilence and famine" to one dominated by degenerative and chronic diseases.
The sources identify several key patterns and causes for this change:
• The Double Burden of Disease: While developed countries primarily face chronic diseases, many developing nations now experience a "double burden," dealing with infectious diseases and chronic illnesses simultaneously.
• Globalization of Risk: The rapid transmission of unhealthy behaviours from developed to developing cultures has fueled a chronic disease epidemic. This includes urbanisation, which is directly associated with increased rates of cardiovascular disease.
• Dietary Shifts: Changes in global diet, particularly in urban areas, have led to increased energy intake from fats and animal sources.
• Lack of Infrastructure: Many governments have prioritized economic development over health, leaving them with underdeveloped public health systems and policy responses to combat these rising risks.
Projections indicate that through 2030, global deaths from cancers, stroke, and ischaemic heart disease will continue to rise, while deaths from infectious diseases like malaria and tuberculosis are expected to decline.
lecture question: What does the ‘commonality of risk factors’ mean and how is it relevant to prevention efforts?
Commonality of risk factors refers to the fact that a specific core group of behaviours—smoking, unhealthy diet, being overweight, sedentary lifestyle, alcohol abuse, and psychosocial stress—collectively contribute to the development of several major chronic illnesses, such as cardiovascular disease, cancer, and diabetes.
This concept is vital to prevention efforts for the following reasons:
• Efficiency: Because these major diseases share the same roots, health interventions targeting a single common risk factor (like diet or smoking) can simultaneously reduce the prevalence of multiple conditions.
• Shifting the Distribution: It supports a population prevention strategy that aims to move the entire distribution of exposure in a favourable direction. Since the majority of disease cases in a population arise from the large number of people at moderate or low risk rather than just those at high risk, addressing shared factors across the whole community is essential.
• Superior Outcomes: Data indicates that a population-wide approach to primary prevention is significantly more effective than a high-risk clinical approach, potentially avoiding 67% of yearly deaths and 78% of disease cases.
• Policy Focus: It encourages the use of healthy public policy and the creation of environments supportive of health, rather than relying solely on treating individuals once they have already become sick.
Does our environment impact our health?
Yes, our environment has a big impact on our health.
Do our communities impact our health?
Yes, our communities impact our health.
What is the model of factors affecting health?