PSCY 103H Health psychology Final Exam Study Guide
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
Chapter 9 – Cardiovascular Disease
coronary arteries
supply blood to the heart
atherosclerosis
- the formation of plaque restricts or partially blocks the blood flow in the artery
arteriosclerosis
the loss of elasticity (hardening) of the arteries
ischemia
restriction of blood flow
myocardial infarctions
- heart attack; death of myocardial tissue
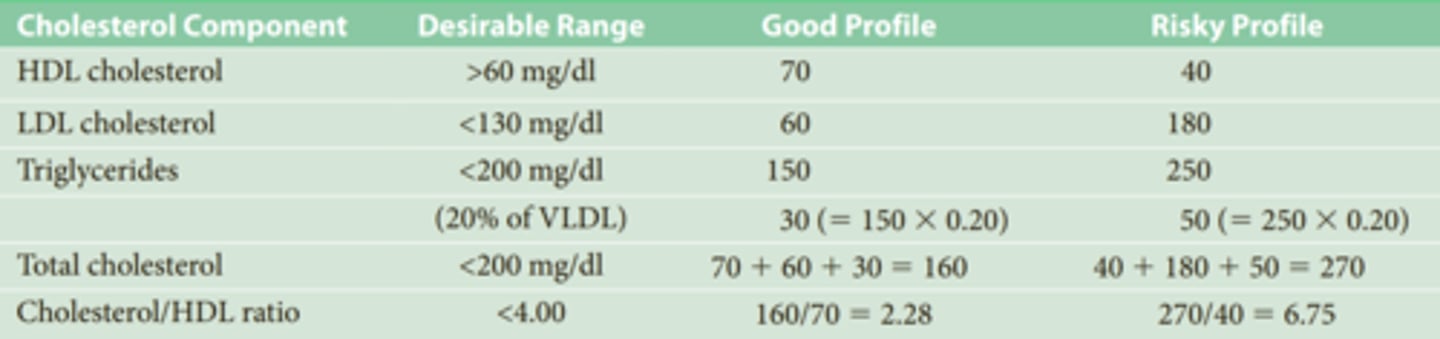
3. What are high and low density cholesterol and how are they related to heart disease?
•HDL - high-density lipoprotein (“good cholesterol”) – protects the heart
•LDL - low-density lipoprotein (“bad cholesterol”) – risk factor for heart
HDL actually seems to offer some protection against CVD, whereas LDL seems to promote atherosclerosis
2. What are the strongest predictors of heart attacks and stroke?
Advancing age is the primary risk factor for CVD
Hypertension (high blood pressure) and cholesterol
Risk factors:
•Smoking
•Type A personality (hostility/anger)
•Suppressed worse than expressed
• Men more than women
•Poor marriages (lack of social support)
•African Americans (racism stress)
4. What kinds of foods offer protection against heart disease?
•Fruits, veggies, fish, chocolate
5. What is Type A personality and what part of Type A personality puts people at the greater risk for heart disease?
Hostile, competitive, concerned with numbers and the acquisition of objects, and possessed of an exaggerated sense of time urgency.
Hostility appeared to be the component of Type A that was risky.
Anger is an unpleasant emotion accompanied by physiological arousal, whereas hostility is a negative attitude toward others.

6. How are marital status and gender (whether a person is male or female) related to heart disease?
Married men were almost half as likely to die as unmarried men. For women, the benefits depended on marital communication and quality, with poor communication increasing heart disease risk.
• In general, Men are more at risk than women.
•Poor marriages increase risk (lack of social support)
7. What racial / ethnic groups have higher rates of heart disease and why?
In the United States
African Americans have more than a 30% greater risk for cardiovascular death than European Americans,
The increased risk for African Americans may be related to social, economic, or behavioral factors rather than to any biological basis (racism stress)
Native Americans, Asian Americans, and Hispanic Americans have lower rates. These discrepancies are most likely due to behavioral and psychosocial factors rather than to biology.
An examination of survival differences between African Americans and European Americans showed that controlling for socioeconomic factors erased the difference in survival rates, which suggests that social and economic factors create the disparity
8. Why are anti-inflammatory drugs like aspirin related to lower risk of heart disease?
Any factor that reduces inflammation may reduce the risk for CVD. For example, aspirin—an anti-inflammatory pain reliever—lowers the risk of heart attack. Thus, the findings about the risks from inflammation explain why taking aspirin lowers the risk of heart attack. Thins the blood.
9. How have health psychologists contributed to heart health?
Psychology’s main contribution to cardiovascular health involves changing unhealthy behaviors before these behaviors lead to heart disease.
After Diagnosis:
•Cardiac rehabilitation: a program that aims to change their lifestyle and lower risk for a subsequent (and possibly even more serious) event. In addition to survival, the goals of cardiac rehabilitation programs are to help patients deal with psychological reactions to their diagnosis, to return to normal activities as soon as possible, and to change to a healthier lifestyle.
Chapter 11 – Chronic Illness
10. What is the difference between heart patients who do and do not participate in cardiac rehabilitation?
Cardiac rehabilitation is:
-associated with a decrease in anxiety and depression after diagnosis
-associated with a 34% reduction in cardiac mortality and 29% reduction in the recurrence of heart attack
1. What percentage of people at different ages develop Alzheimer's disease?
-for those under age 75, about 9%
-by age 85, almost 50% of individuals exhibit signs of Alzheimer’s disease.
2. What is asthma?
•an inflammatory disease that causes constriction of the bronchial tubes, preventing air from passing freely
•7% of Americans have asthma
3. What is diabetes?
•a disorder caused by insulin deficiency
•Diabetes increases risk for cardiovascular problems, including CVD as well as renal disease and infectious diseases
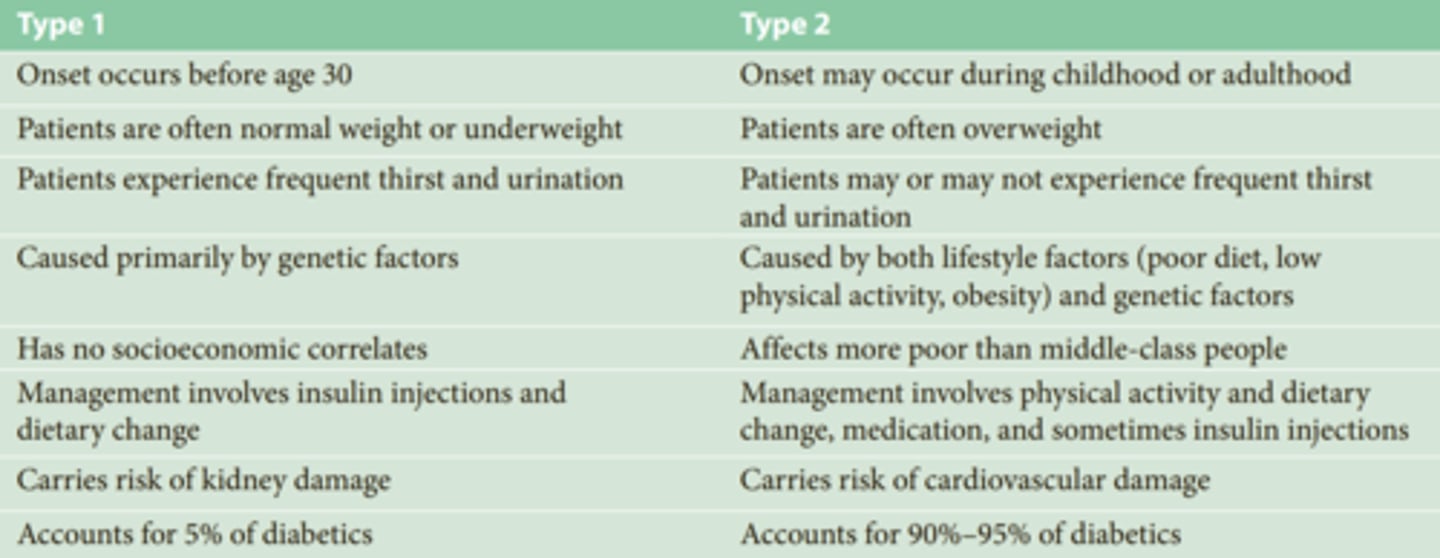
4. What are the differences between Type 1 and Type 2 diabetes and why are they no longer called “juvenile-onset diabetes” and “adult-onset diabetes”?
• Insulin-dependent (Type 1) - autoimmune disorder; occurs usually before age of 30; cannot produce insulin; no cure
•Caused primarily by genetic factors
•Has no socioeconomic correlates
•Accounts for 5% of diabetics
•Non-insulin-dependent (Type 2) - more common
•Onset may occur during childhood or adulthood
•Patients are often overweight, caused by genetic factors and lifestyle factors such as poor diet, low physical activity
•Increasingly appears among children and adolescents, which is why it is no longer called "adult-onset diabetes"
Accounts for 90-95% of diabetics
5. What are the differences in the risk for Type 1 and Type 2 diabetes between ethnic groups?
Type 1 diabetes: Caused primarily by genetic factors. Has no socioeconomic correlates.
Type 2 diabetes: African Americans, Hispanic Americans, and Native Americans are at higher risk than European Americans, and being overweight is a risk for all groups.
7. What is the leading cause of death among people with Type 1 and Type 2 diabetes?
Type 2 diabetes is more likely to cause circulatory problems, leaving these individuals prone to cardiovascular problems, which is their leading cause of death.
both women and men with Type 2 diabetes are at dramatically increased risk for death from all causes, but especially from cardiovascular disease.
6. How do the rates of Type 2 diabetes vary between Pima Indian groups in Mexico vs. the United States? Why?
• Rate of diabetes was 38% in adult U.S. Pima Indians, and 6.9% in adult Mexican Pima Indians
• Also much higher rates of obesity
• Pima Indians are thought to have a “thrifty gene” that increases the risk of diabetes.
• Mexican Pima Indians farm and grow most of their own food, plowing with the aid of oxen or mules and planting and harvesting their crops by hand.
• U.S. Pima Indians have low levels of occupational physical activity
• Even with genetic predisposition, rates of diabetes are largely influenced by the environment and are preventable.
8. What are the risk factors for asthma? (5)
•Children have the highest rates
•Risk factors:
•More common in developed countries
•More common in urban areas
•More common for African Americans
•A sedentary lifestyle
•obesity
9. What are the main risk groups for HIV infection in the United States?
•Ethnic minorities are particularly at risk; African Americans have the highest percentage of racial groups in the period from 2009-2013
•Men who engage in male-to-male sexual contact
•Injection drug users
•Heterosexual contact without protection
•Children born to HIV+ mothers

10. What are the four different HIV/AIDS epidemics?
1. male–male sexual contact: In the early years of AIDS, men who had sex with men made up the majority of AIDS cases in North America and Western Europe. Male–male sexual contact is still the leading source of HIV infection in the United States. This mode of transmission declined during the 1990s but has increased slightly during the past few years; it now accounts for more than half of HIV transmissions in the United States
2. injection drug use: Injection drug use is the second most frequent source of HIV infection in the United States and accounts for about 32% of HIV cases among women in the United States.
3. heterosexual contact: Heterosexual contact is the leading source of HIV infection in Africa, but in the United States, heterosexual sex accounts for about 30% of cases. African Americans and Hispanic Americans are disproportionately represented among those infected through heterosexual contact, and women from these two ethnic backgrounds are in greater danger than men from heterosexual contact
4. transmission from mother to baby: This transmission tends to occur during the birth process. Breastfeeding can also transmit the virus. Children infected with HIV during the birth process suffer from a variety of developmental disabilities.
11. What are the chances of an HIV infected mother infecting her child during birth and what can be done to reduce the chances?
Transmission during the birth process is likely unless the HIV-positive mother undergoes antiretroviral therapy.
Early prenatal care can reduce the risk of transmission from mother to child to about 1%.
12. What are the most important behaviors that can protect people from contracting the HIV virus? (3)
1. Limiting the number of sex partners
2. using condoms
3. avoiding shared needles
are three behaviors that will protect the largest number of people from HIV infection
Although some risks are specific to certain professions, most people infected with HIV acquired the virus through sexual behavior or by sharing contaminated needles. People can protect themselves against HIV infection by changing those behaviors that are high risks for acquiring the infection—namely, having unprotected sexual contact or sharing needles with an infected person.
Chapter 14 – Eating & Weight
Leptin
protein hormone secreted by adipose (fat) cells; tells us when we need food
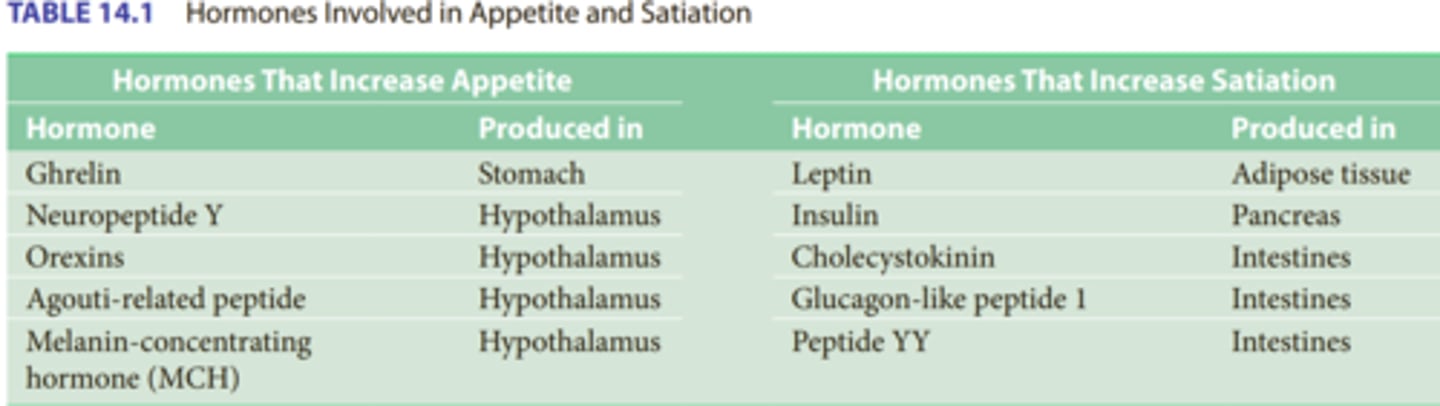
Insulin
A protein hormone synthesized in the pancreas that regulates blood sugar levels by facilitating the uptake of glucose into tissues
Tells the hypothalamus when we have eaten enough food
Ghrelin
A hormone secreted by an empty stomach sends hunger signals to the brain.
Stimulates appetite and decreases metabolism
CCK
Produced by the small intestine when you eat and tells the brain you're full, suppressing appetite.
Orexin
hunger-triggering hormone secreted by the hypothalamus.
Neuropeptide Y (NPY)
Neurotransmitter found in several brain areas, most notably the hypothalamus, that stimulates eating behavior and reduces metabolism, promoting positive energy balance and weight gain
1. What two things must be balanced for your body to maintain its current weight? How do biological and environmental forces affect this balance?
calories eaten and calories expended from body metabolism and physical exercise
Biological factors:
• Very high Heritability of body weight: 60-80%
• There are over 200 genes identified that contribute in some way - genes related to how much you fidget, metabolism, appetite, etc
• Metabolic rates differ from person to person
• As weight fluctuates, hormones stimulate changes in metabolism and appetite
• Body is preparing for scarcity of food.
• A woman who drops from 200 to 130 lbs has to eat fewer calories to maintain that weight than a woman whose weight was steady at 130 (set point).
Environmental factors:
• Portion size increases
• Americans consume about 200 calories more per day than 30years ago
• Fast food items are 2-5x larger than in the 1980s
• New editions of cookbooks have larger portions for same recipes –43.7% increase in Joy of Cooking.
Portion sizes in the US are much larger than other countries. Fast food has grown in popularity and there is more variety.
2. What was Key's study of experimental starvation and what did he find?
Participants Volunteered to go on a severely restricted diet for 6 months instead of going to war (WWII).
Showed that too much weight loss leads to irritability, aggression, and preoccupation with food
3. What was Sim's study of experimental overeating and what did he find?
-Prisoner volunteers challenged to gain 25% of body weight by consuming 7000 calories per day for 6 months
-Showed that too much eating leads people to become uninterested in eating
4. What is BMI, what is a healthy range of BMI, and what is considered overweight and obese?
body weight in kilograms (kg) divided by height in meters squared (m2 )—that is, BMI = kg/m2
Healthy: 18.5-24.9
Overweight: 25-29.9
Obese: 30-34.9
5. What is the setpoint model and how is it related to weight?
Posits that people have a set weight that their body attempts to naturally maintain.
This may be why it is more difficult for some people to lose weight than others.
6. What is the positive incentive model and how is it related to weight?
Holds that the positive reinforcement of eating has important consequences for weight maintenance. This view suggests that people have several types of motivation to eat, including personal pleasure and social context as well as food deprivation and hormone production
The personal pleasure factors revolve around the pleasures from the type and taste of food.
The social context of eating includes the cultural background of the person eating as well as the surroundings, the presence of others, and whether or not they are eating.
Biological factors include the length of time since eating and blood glucose and ghrelin levels.
some proponents of the positive incentive theory take an evolutionary view, contending that humans have an evolved tendency to eat in the presence of food. The scarcity of food has built up animals that survived when they lay on fat, making eating and the selection of food an important evolved ability.
7. What is the relationship between weight and health?
Being slightly overweight is not much of a health risk, but increasing overweight increases risks, and being obese places a person at an elevated risk for health problems and premature death.
U-shaped relationship has appeared between weight and poor health; that is, the very thinnest and the very heaviest people seem to be at greatest risk for all-cause mortality

8. What are the most effective strategies for maintaining weight loss for a year or more?
1. Eating low calorie, low fat diet (not low carb)
2. Exercise
3. Frequent self-monitoring
maintaining the reduced weight levels is a matter of permanent changes in basic eating habits and activity levels:
Exercising, eating fewer fatty and sweet foods, increasing consumption of fruits and vegetables, and cutting down on portion size.
Behavior Modification Programs
formal weight reduction interventions with posttreatment programs
For example, a comparison of two follow-up interventions in dieters who had completed a 6-month weight loss program included three groups of dieters. One group received no follow-up, one received an intervention that involved brief personal contact on a monthly basis, and another consisted of an interactive, technology-based intervention. The personal follow-up was more effective, but both interventions produced dieters who weighed less than before they started the program. Thus, the follow-up need not be intensive or complex; simple procedures can be effective. For example, people who lost weight and weighed themselves daily were less likely to regain the lost weight than those who did not step on the scales so often
9. What are the advantages and disadvantages of low carbohydrate and low fat diets?
Both approaches showed success. Despite warnings from nutritionists about the dangers of low-carbohydrate diet plans, people who follow these diets have not experienced unfavorable changes in cholesterol levels or risks for cardiovascular disease.
In one study comparing Slimfast, Atkins, and Weight Watchers, all diets fared better than the control group for short-term weight loss
• Atkins had more initial weight loss but was no more effective at the end.
All of the diets produced significant weight loss compared to individuals who did not diet, but long-term weight loss is modest—in the 10- to 12-pound range
Restricting carbohydrates (such at the Atkins diet):
lower drop-out rates
Restricting fat (LEARN diet):
Higher drop-out rates
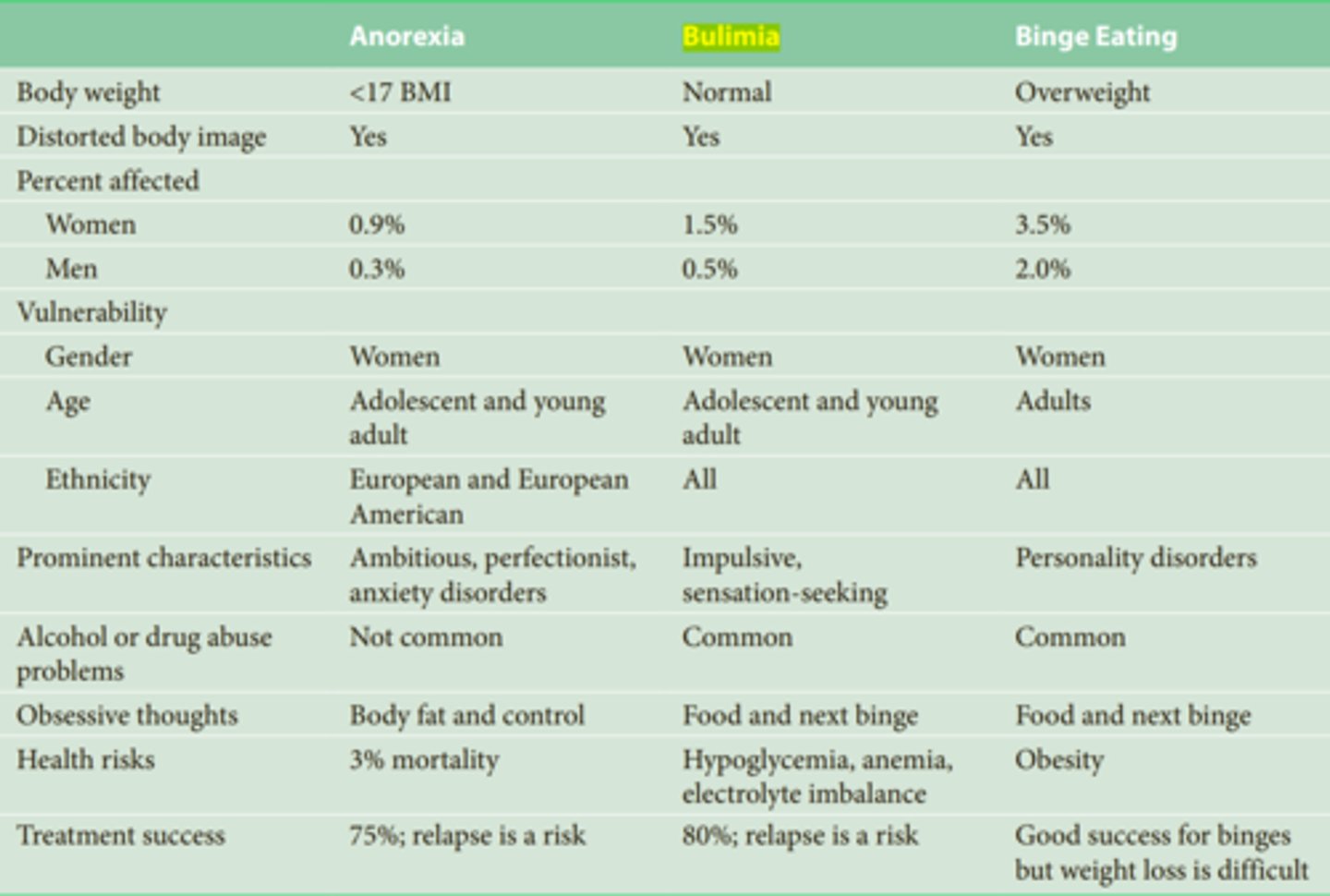
10. What are the differences between the diagnoses of anorexia, bulimia, and binge eating disorder?
Anorexia:
-Intentional starvation typically due to a distorted self-image
-Must be less than 85% of normal weight in order to be diagnosed. (Restricting type and binge-purge type)
Bulimia:
-Repeated binging and purging.
-No certain weight requirement to be diagnosed
binge eating disorder:
To be diagnosed with this disorder, people must exhibit frequent binge eating episodes (an average of at least once a week for at least 3 months) with feelings of a lack of control, and they must experience distress over this behavior.
11. What are the differences between different eating disorders in the motivation for changing their eating habits and the amount of guilt they feel for their behavior?
Anorexia:
Obsess over body fat and control
distorted self-image
Bulimia:
Obsess over Food and next binge.
body dissatisfaction
lack of impulse control
usually accompanied by guilt
-Risk factors: childhood sexual abuse, childhood physical abuse, or post-traumatic stress, recent sexual assault
Binge eating disorder:
Obsess over Food and next binge.
the same type of out-of-control eating that is symptomatic of bulimia, but without any form of compensation.

12. What are the health hazards of anorexia, bulimia, and binge eating disorder?
Anorexia:
3% mortality
Bulimia:
Hypoglycemia, anemia, electrolyte imbalance, damaged teeth, damage in the mouth and esophagus
Binge eating disorder:
Obesity

Chapter 13 – Alcohol & Other Drugs
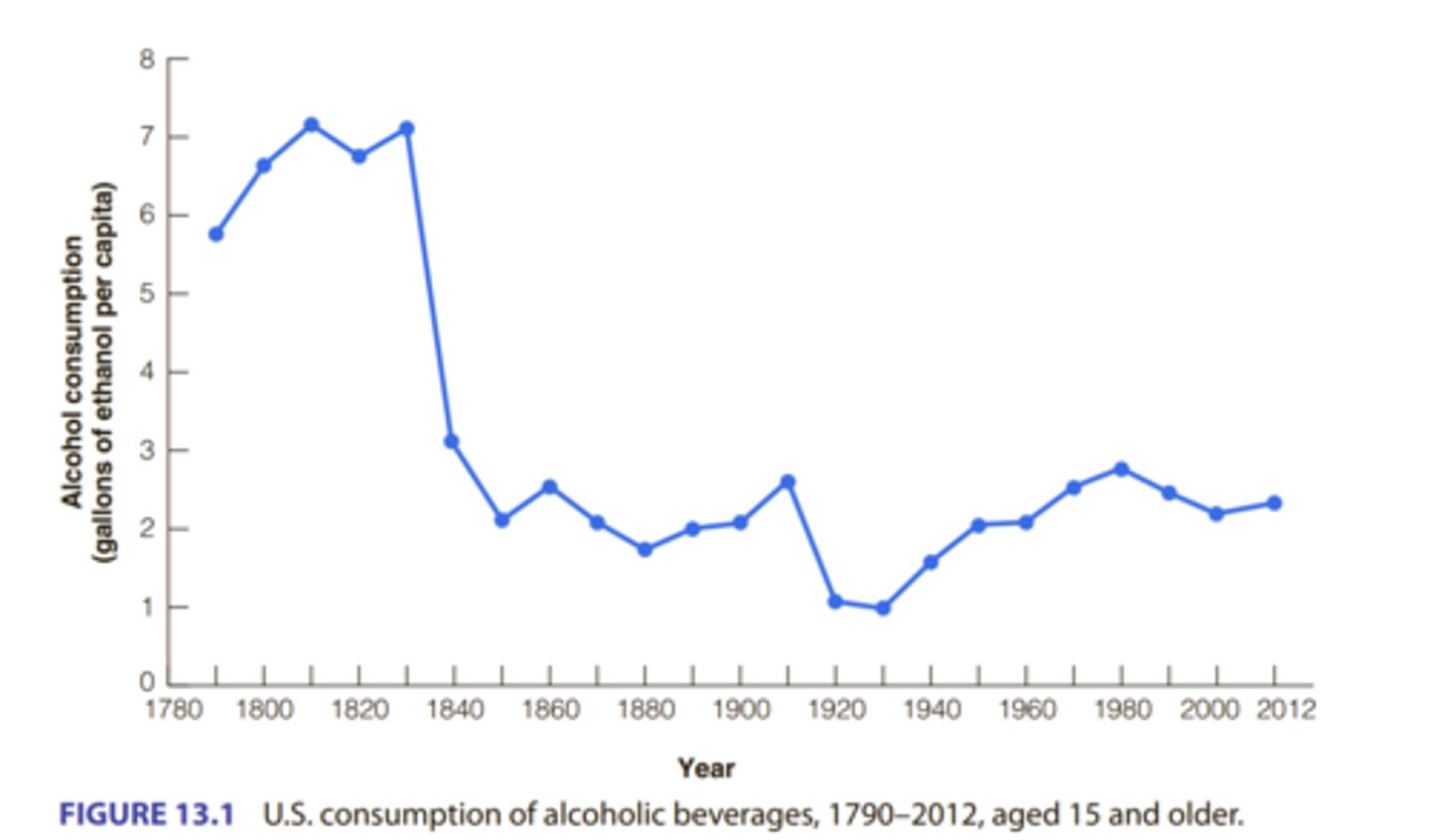
1. How have drinking habits developed through history? What is temperance? What is prohibition?
In colonial America, drinking was much more common than it is today
.• Partially because water and milk were not always purified
.• Early Puritans objected to drunkenness, not drinking.
Temperance: the moderate use of alcohol.
prohibition: the total abstinence from alcohol.
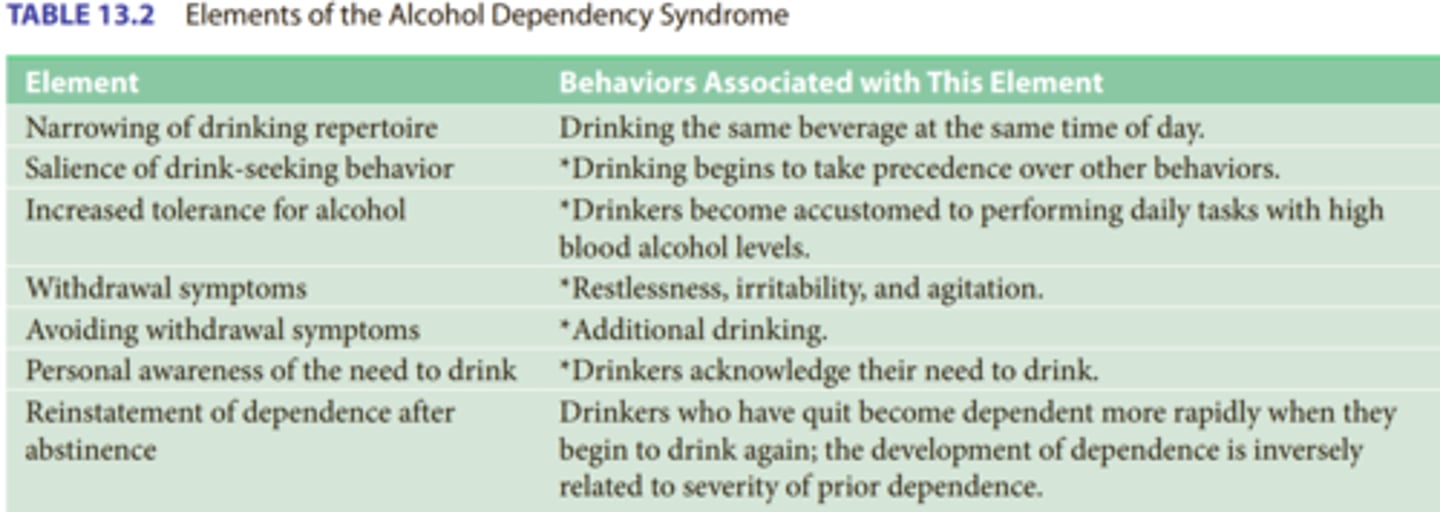
3. What do the terms tolerance and dependence refer to with regard to drinking and drug use?
Tolerance is a term applied to the effects of a drug when, with continued use, more and more of the drug is required to produce the same effect
Dependence occurs when a drug becomes so incorporated into the functioning of the body’s cells that it becomes necessary for “normal” functioning.
What are the differences between age, gender, and ethnic groups in levels of drinking, heavy drinking, and binge drinking?
Age Differences in Drinking
Adults aged 25 to 44 have the highest rates of drinking, but young adults aged 18 to 24 have the highest rates of binge drinking and heavy drinking. More than a third of drinkers aged 18 to 24 are binge drinkers, but they may age into more moderate drinkers.
Gender Differences in Drinking
Men are more likely than women to be current drinkers (57% to 48%), binge drinkers (30% to 16%), and heavy drinkers (9% to 3%). These percentages suggest that men have more problems with binge and heavy drinking than women.
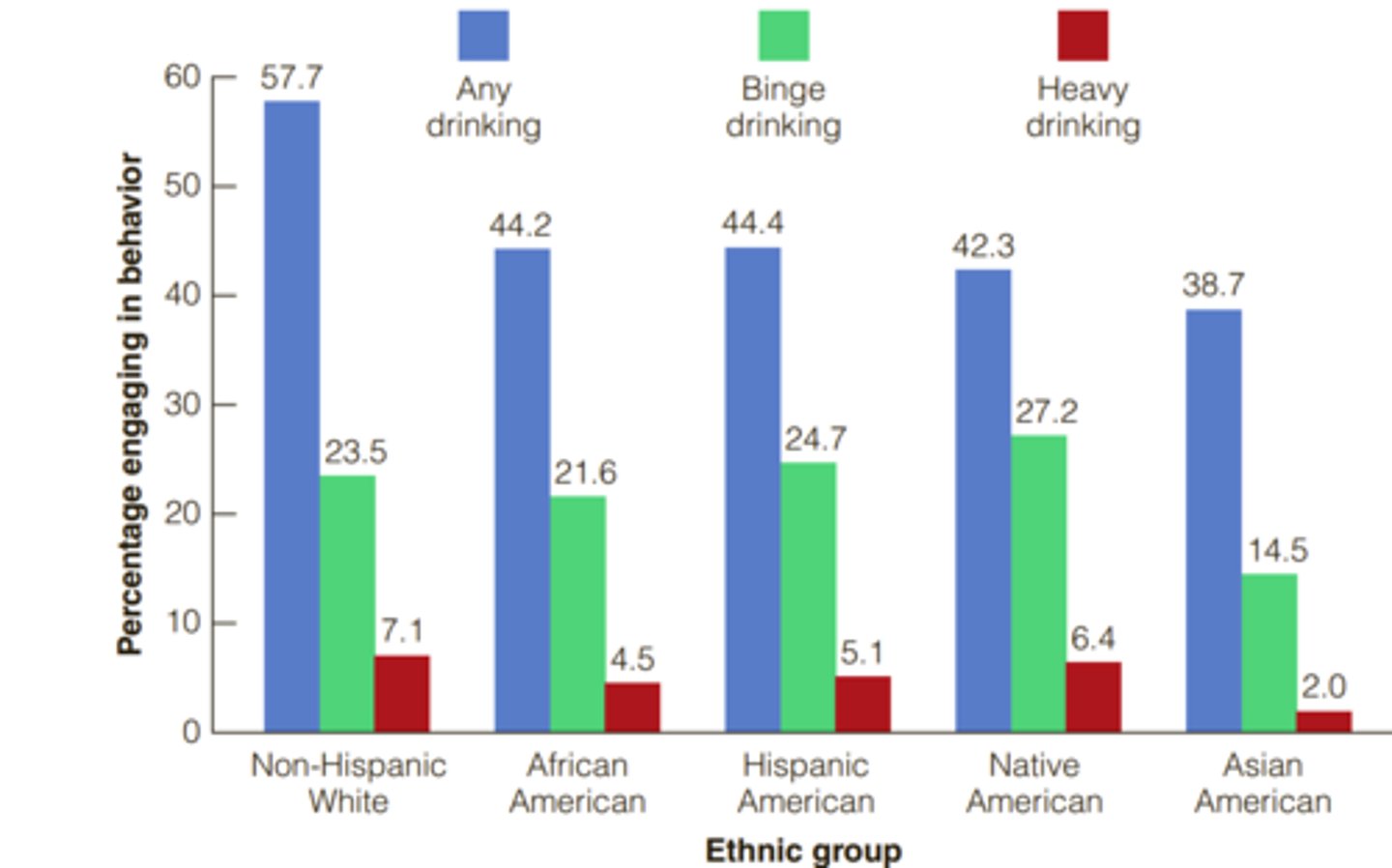
Ethnic Differences in Drinking
(percent that have consumed alcohol in the last month)
1) European Americans: 57.7%
2) Hispanic Americans: 44.4%
3) African Americans: 44.2%
4) Native Americans: 42.3%
5) Asian Americans: 38.7%
(percent that are binge drinkers (5+ drinks at once))
1) Native Americans: 27%
2) Hispanic Americans: 24.7%
3) European Americans: 23.5%
4) African Americans: 21.6%
5) Asian Americans: 14.5%
(percent that are heavy drinkers (14+ for men and 7+ for women per week))
1) European Americans: 7.1%
2) Native Americans: 6.4%
3) Hispanic Americans: 5.1%
4) African Americans: 4.5%
5) Asian Americans: 2%
4. What is the relationship between the amount of alcohol consumed and mortality?
f several early studies reported a U-shaped or J-shaped relationship between alcohol consumption and mortality. That is, research indicated that people who did not drink and those who drank heavily died earlier than those who drank at low-to-moderate levels. This advantage appeared first among men, but additional research showed that this advantage applies to women.
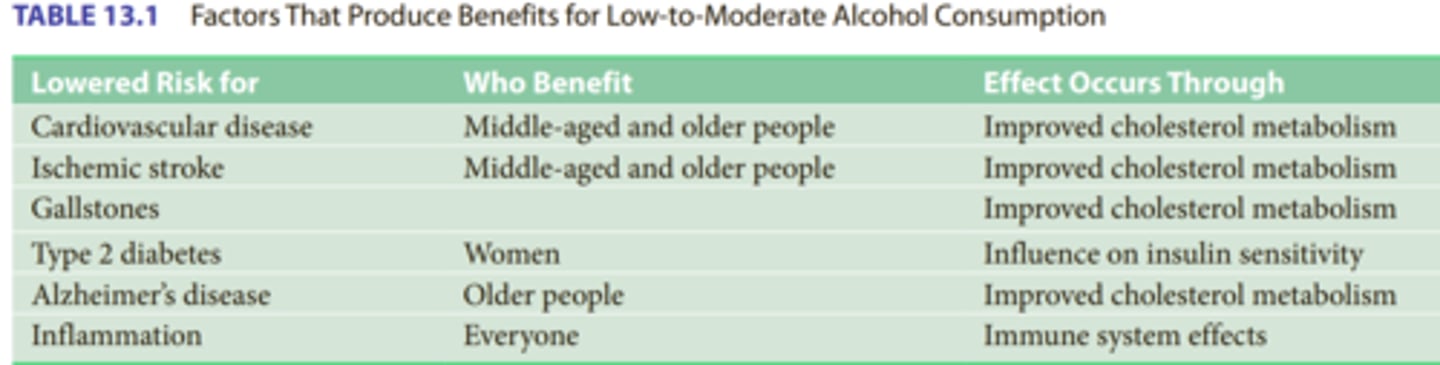
5. How is alcohol use related to heart disease and what is the difference between the effects of different kinds of alcohol?
Alcohol intake has a causal relationship to changes in cholesterol that are beneficial and lower the risk of cardiovascular disease.
Low-to-moderate levels of alcohol seem to be beneficial in decreasing the risk for diseases that result from restriction of blood flow through arteries.
-Wine is high in antioxidants, which also reduce the risk of CVD.
disease model
E. M. Jellinek described several different types of alcoholism and their characteristics. However, this model casts alcoholism as an incurable disease, which is too simplistic, even with the different varieties that Jellinek described.
This view became increasingly popular beginning in the late 1930s and early 1940s.
Tension reduction model
holds that people drink alcohol because of its tension-reducing effects. This hypothesis has much intuitive appeal because alcohol is a sedative drug that leads to relaxation and slowed reactions. Despite its consistency with popular belief, experimental studies have furnished limited support for the tension reduction hypothesis.
social learning model of drinking
conceptualizes drinking as a learned behavior acquired in the same manner as other behaviors. People begin to drink for at least three reasons. First, the taste of alcohol and its immediate effects may bring pleasure (positive reinforcement); second, drinking may allow a person to escape from an unpleasant situation (negative reinforcement); and third, the person may learn to drink through observing others (modeling).

. What is the main goal of Alcoholics Anonymous and what does it assume about people's ability to control their drinking?
To adhere to the AA doctrine, a person must maintain total abstinence from alcohol.
Those who are in need of joining AA can never drink again; problem drinkers are addicted to alcohol and have no power to resist it. According to AA, alcoholics never recover but are always in the process of recovering. They will be alcoholics for life, even if they never take another drink
8. What have studies of controlled drinking found?
A large-scale study in Germany found that tension reduction is one of the effects that drinkers expect. Thus, tension reduction is one of many effects that may occur as a result of drinking, but expectancy may be more important than alcohol in these effects.

9. What drugs are classified as stimulants, depressants, and hallucinogens?
stimulants
Tobacco, caffeine, nicotine, amphetamines, and cocaine.
depressants
Barbiturates, Tranquilizers, Opiates, Alcohol
hallucinogens
Ecstasy (MDMA), LSD
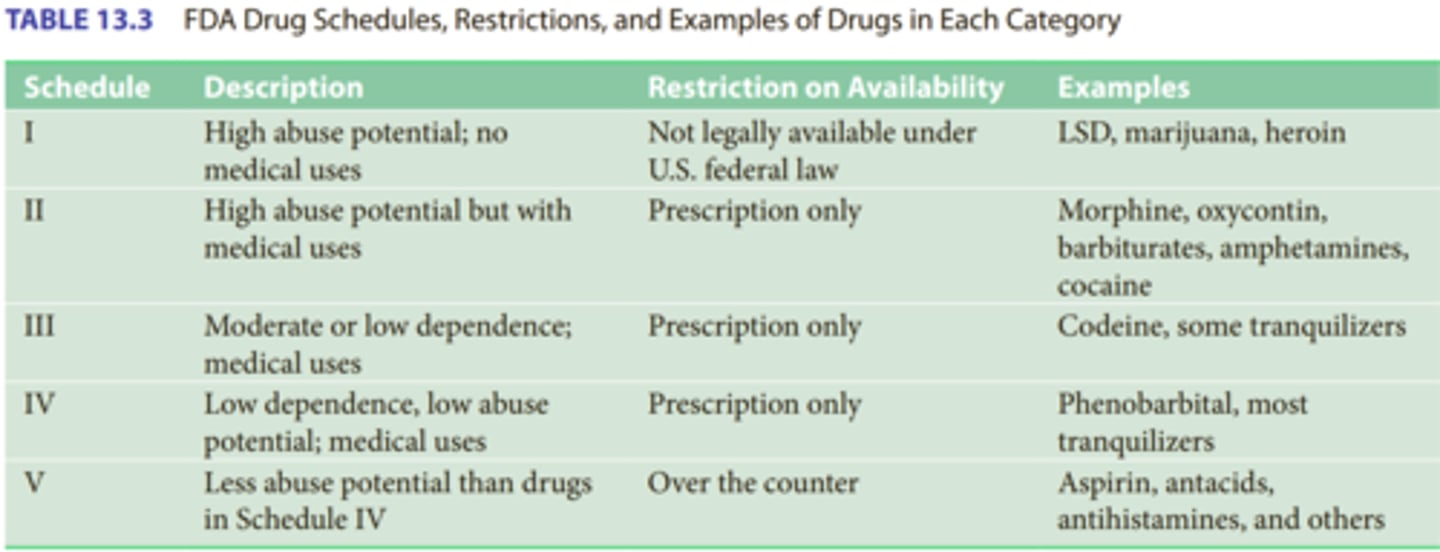
10. What do the five different "Schedules" of drug classifications by the Food and Drug Administration refer to?
The FDA classifies drugs into five categories based on their potential for abuse and their potential medical benefits. (Higher number, less potential for abuse)
11. How might positive and negative reinforcement be related to drinking and drug use?
Drinking and drug use bring pleasure (positive reinforcement) and may allow a person to escape from an unpleasant situation or remove a negative state (negative reinforcement).
12. What neurotransmitter(s) may be most involved in the effects of several drugs?
Several neurotransmitters are involved in drug actions, including GABA, glutamate, serotonin, and norepinephrine, but the neurotransmitter dopamine is especially important.
13. What are the standard servings for beer, wine and hard alcohol (i.e. what is a standard drink?)
Beer: 12 oz
Malt liquor: 8-9 oz
wine: 5 oz
hard alcohol: 1.5 oz

Chapter 10 – Cancer
1. What is cancer?
Group of disease characterized by the occurrence of new cells that grow and spread beyond control
Neoplastic cells have almost unlimited growth, deprive the host of nutrients, and provide no compensatory benefits. All cancers exhibit this characteristic.
2. What is the difference between benign and malignant tumors and how are they related to metastasis?
• Benign – remain localized; usually less threatening
• Malignant – spreads; usually more dangerous because they can invade and destroy surrounding tissue.
• metastasis the spread of malignancy from one part of the body to another by way of the blood or lymph systems.
Malignant Growths
1. Carcinomas – cancers of the epithelial tissue
2. Sarcomas – cancers of the connective tissues (bone, muscles, cartilage)
3. Leukemias – cancers of the blood
4. Lymphomas – cancers of the lymphatic tissue; less common
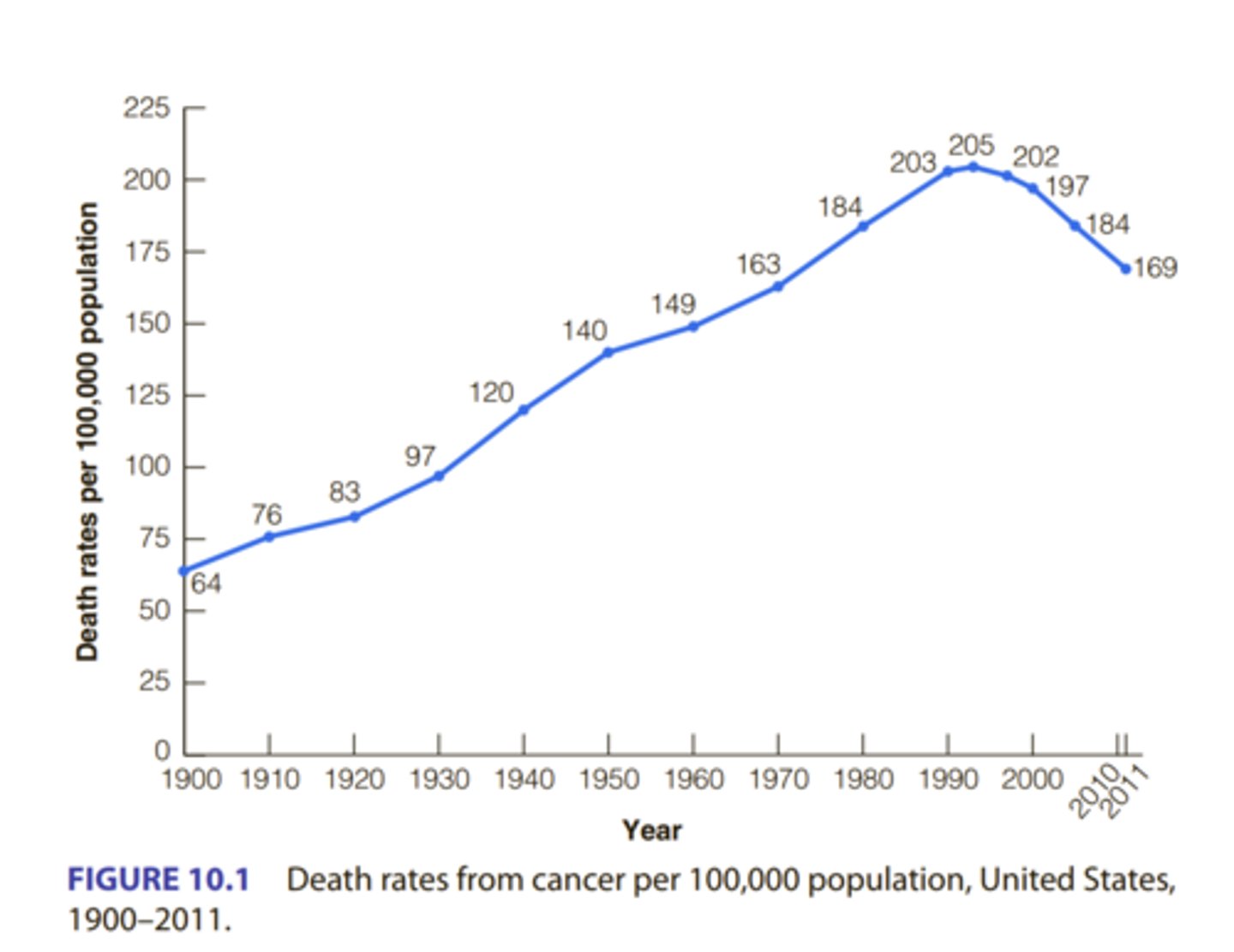
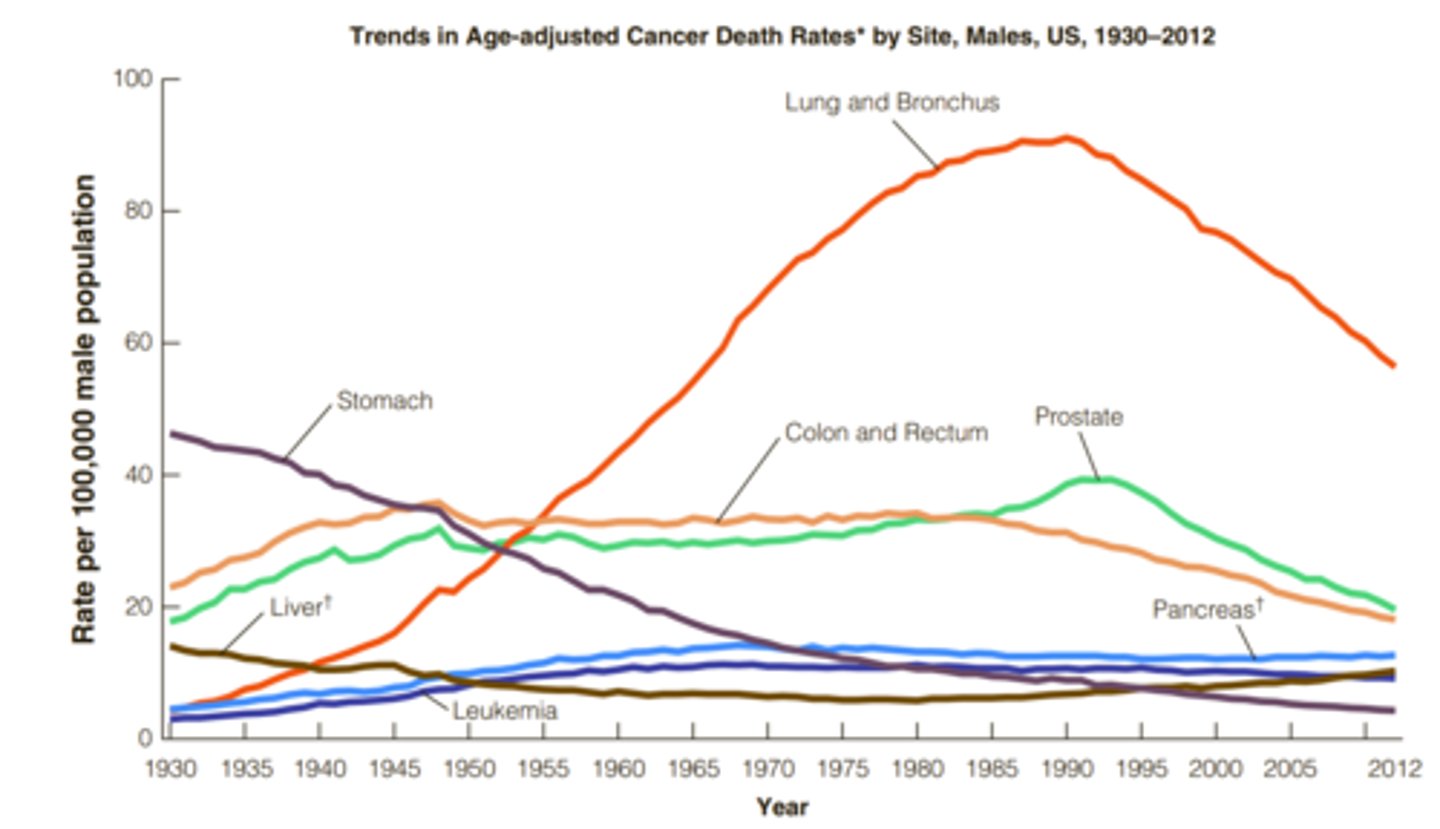
3. What are the biggest reasons for declining death rates due to cancer?
Death rates from cancer declined in the 1990s due to:
• Early detection and treatment
• Lifestyle factors (better diets, less smoking) – large role in decline
• The decrease is significant—more than 22% for men and more than 15% for women since 1990
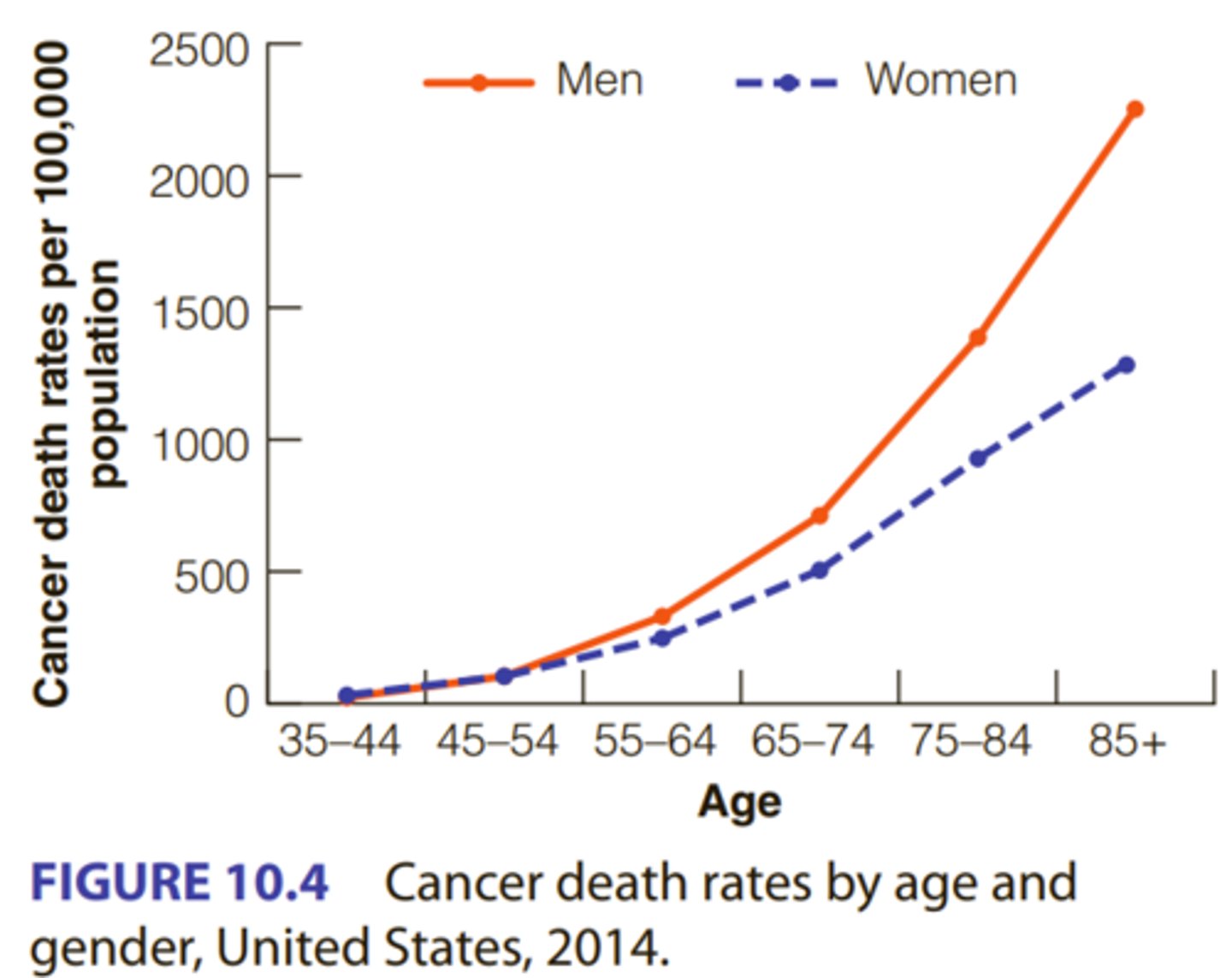
4. What are the strongest inherent (3) and behavioral (6) risk factors for cancer?
INHERENT RISK FACTORS
• Advancing age: The strongest risk factor for cancer.
• genes play a fairly minor role in the development of cancer; environmental and behavioral factors are much more important.
• Ethnic background: African Americans have a greater incidence of most cancers, and mortality is higher. However, Hispanic Americans, Asian Americans, and Native Americans have lower rates than either African Americans or European Americans for all cancer sites combined, as well as for the four most common cancers
• Family history: women whose mothers received a breast cancer diagnosis before age 40 were more than twice as likely to develop breast cancer.
• Women with the BRCA 2 mutation may be at a greater risk of alcohol-induced breast cancer compared with women without the BRCA 2 mutation.
BEHAVIORAL RISK FACTORS
• Smoking: The single largest risk for cancer mortality worldwide.
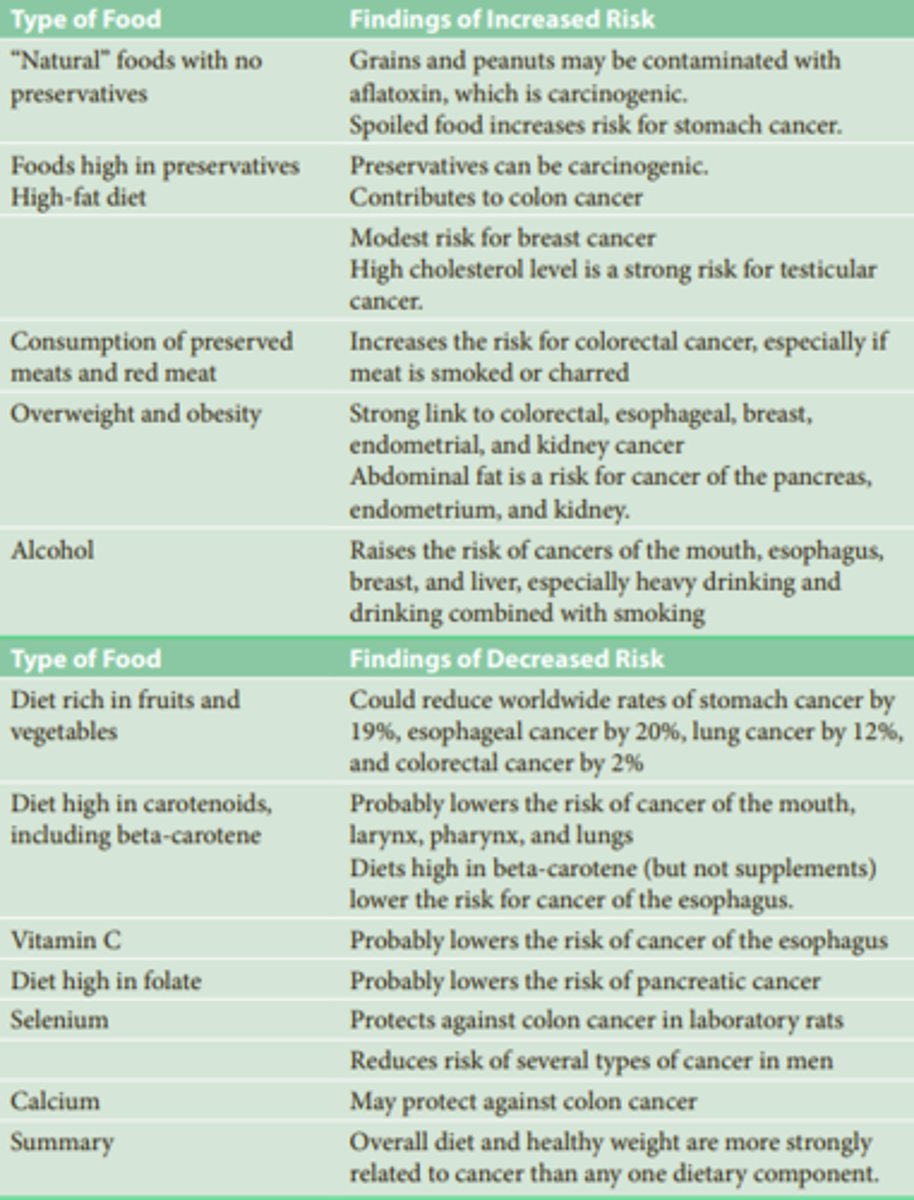
• Diet: preserved, charred, smoked red meats, and salt-cured or heavily salted meats raise risks.
Beta-carotene, found in carrots and sweet potatoes, lowers the risk of cancers, as does a diet rich in vitamin C.
• Alcohol: Low risk on its own. Smoking and drinking can have a synergistic effect, multiplying the chances of developing cancer.
• Sedentary Lifestyle
• UV light exposure: Light-skinned, fair-haired, blue-eyed individuals are more likely than dark-skinned people to develop skin cancer.
• Sexual behavior
ENVIRONMENTAL RISK FACTORS
Exposure to radiation and asbestos and to pollutants: pesticides, herbicides, motor exhaust, and other chemicals.
Working in a nuclear power plant
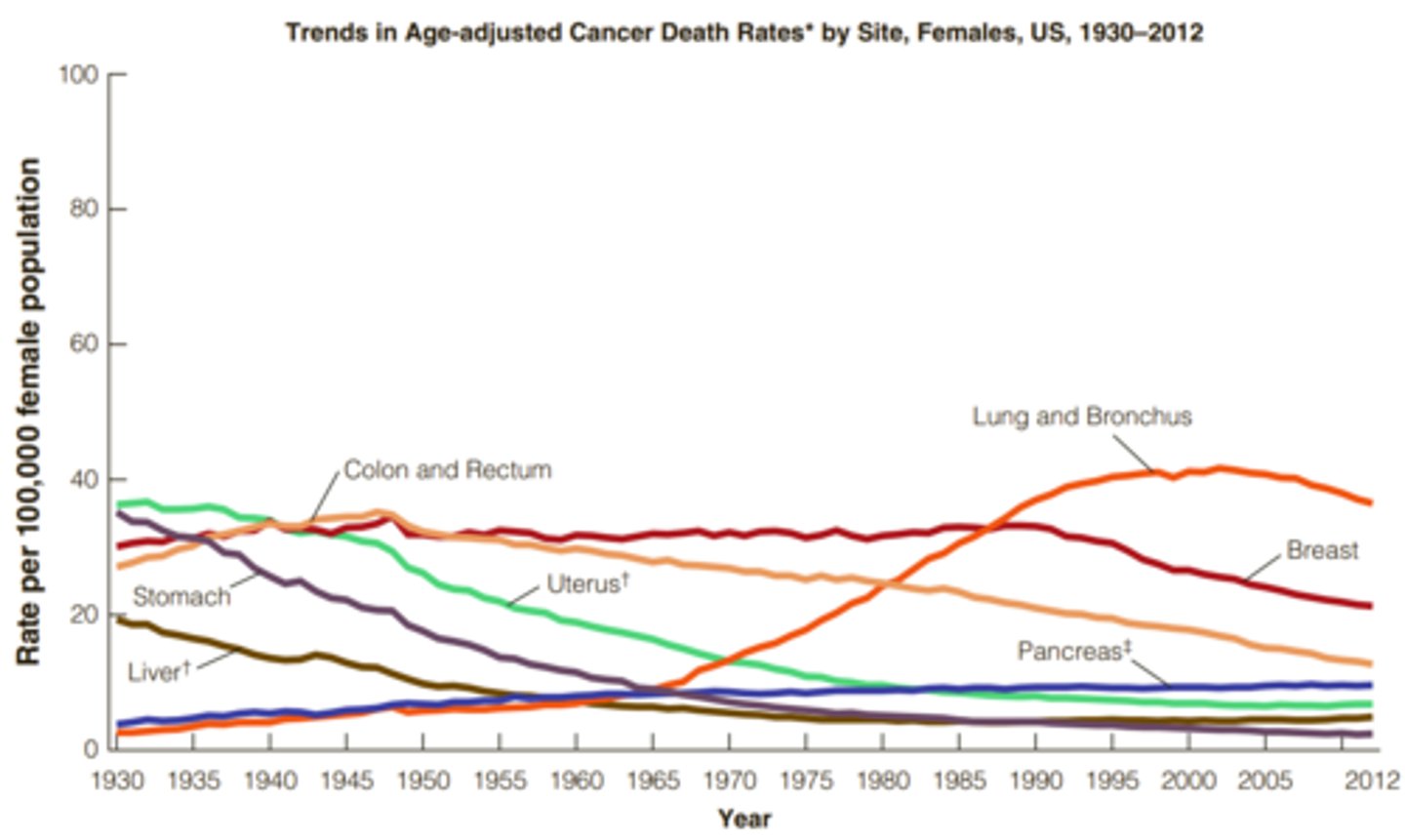
5. What is the most common and what is the most deadly cancer for women?
Most common: Breast
Most deadly: Lung
In general, incidence rates for the four leading cancers— lung, breast, prostate, and colorectal—are declining, especially for men.
-lung cancer continues to show a slight increase among women but a continuing decline among men.
Melanoma, a potentially fatal form of skin cancer, is increasing among both men and women. Cancer of the esophagus is increasing among men yet falling among women.
. What is the most common and what is the most deadly cancer for men?
Most common: Prostate
Most deadly: Lung
In general, incidence rates for the four leading cancers— lung, breast, prostate, and colorectal—are declining, especially for men.
-lung cancer continues to show a slight increase among women but a continuing decline among men.
-Melanoma, a potentially fatal form of skin cancer, is increasing among both men and women. Cancer of the esophagus is increasing among men yet falling among women
7. What factors may account for the different cancer death rates across ethnic backgrounds?
Differences are most likely due to behavioral and psychosocial factors, not biological
• African Americans have a greater incidence of most cancers and greater mortality
• Diagnoses for African Americans tend to come at a later stage, which means lower survival rates
• Native Americans, Asian Americans, and Hispanic Americans have lower rates than either African Americans or European Americans for all cancer sites combined, as well as for the four most common cancers. These discrepancies are most likely due to behavioral and psychosocial factors rather than to biology.
• An examination of survival differences between African Americans and European Americans showed that controlling for socioeconomic factors erased the difference in survival rates, which suggests that social and economic factors create the disparity
• Asian Americans generally have lower total cancer death rates than other ethnic groups, but much higher mortality rate for stomach and liver cancer
• Stomach cancer is highly correlated with diet and chronic H. pylori bacterial infection.
• Liver cancer highly correlated with infection and hepatitis C infection
8. What are the risk factors for cervical cancer?
• HPV increases risk for cervical and oral cancer
About 70% of cervical cancers caused by HPV types 16and 18
9. What behavioral factors are most important for preventing cancer?
Quit/don't start Smoking
maintaining a healthy diet
limiting drinking (probably only a weak risk factor for cancer. Nevertheless, it has a synergistic effect with cigarette smoking; when the two are combined, the total relative risk is much greater than the risks of the two factors added together).
staying physically active
wear sunblock (avoid excessive UV light exposure).
HPV vaccine, condoms, limit number of sex partners)
0. What are the main treatments for cancer and what are their side effects?
surgery, radiation, chemotherapy
• All of these treatments can have negative side effects such as fear and anxiety, loss of hair, fatigue, and depression
11. How have health psychologists been most involved in treating people with cancer?
Psychologists have used both individual and group techniques to help cancer patients cope with their diagnosis.
Therapists can use cognitive behavioral methods to assist cancer patients in coping with some of the negative aspects of cancer treatments and adjusting to their disease, thus increasing the quality of life for cancer patients, but no evidence exists that psychosocial factors can increase survival time. Psychological interventions mainly focus on improving the quality rather than the quantity of a cancer patient’s life.
Chapter 15 – Exercise
1. What are the different types of physical activity?
1. Isometric: Contracting muscle against an immovable object
Example: pushing against a solid wall
Benefit: can improve muscle strength – especially helpful for older people in preserving independent living.
2. Isotonic: Contraction of muscles and movement of joints
Example: lifting weights
Benefit: can improve muscle strength and endurance
3. Isokinetic: Moving muscles and joints against resistance
Example: using specialized equipment that adjusts the amount of resistance according to the amount of force applied
Benefit: important in physical rehabilitation
4. Anaerobic: Short, intensive bursts of energy with no increase in oxygen use
Example: short-distance running
Benefit: can improve speed and endurance
5. Aerobic: Exercise that involves increased oxygen use
Example: jogging, cycling
Benefit: works out both the respiratory system and cardiovascular system
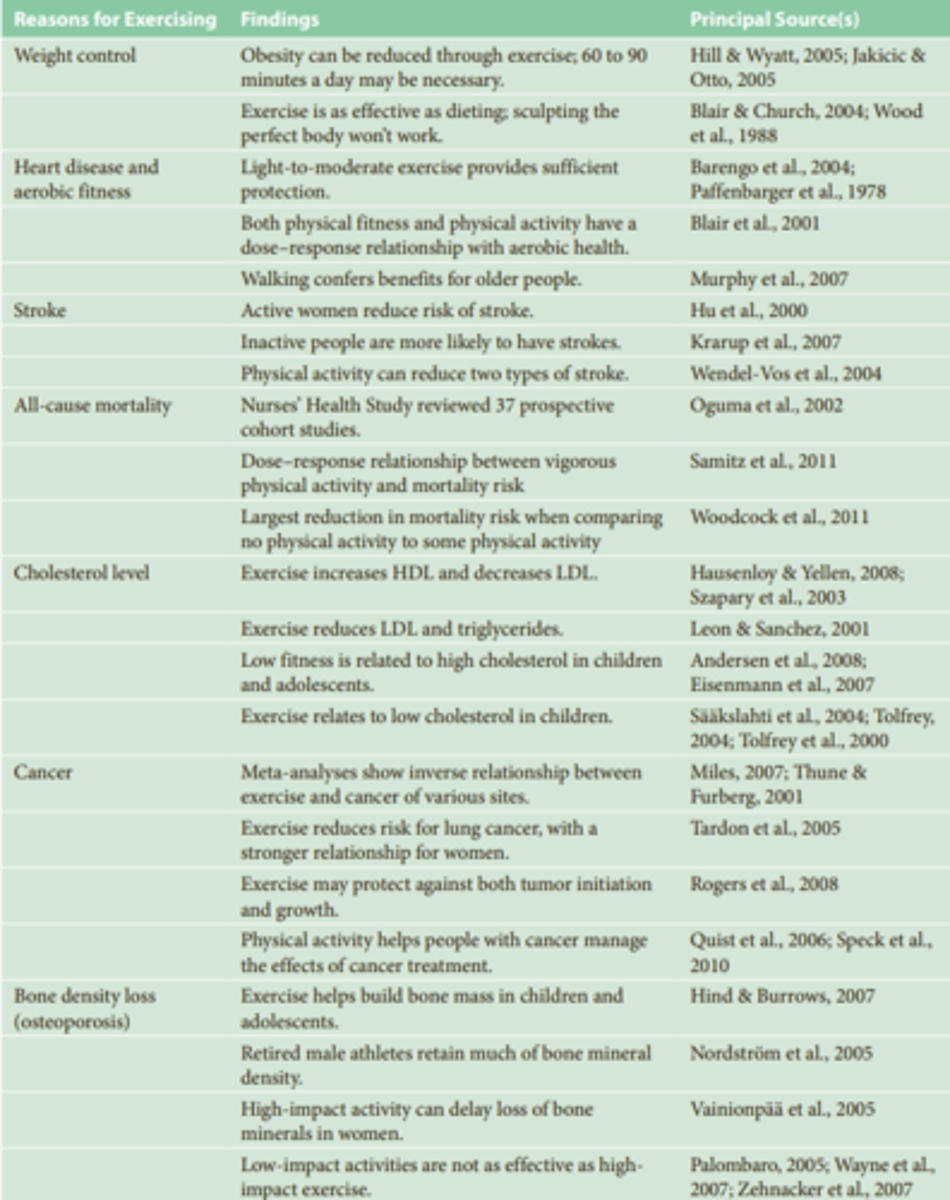
2. What are the reasons for exercising? (6) How does the research support these reasons?
1. Physical Fitness
Organic fitness is the capacity for action and movement that is determined by inherent characteristics of the body. These organic factors include genetic endowment, age, and health limitations.
Dynamic fitness arises through physical activity, whereas organic fitness does not. A person can have a good level of organic fitness and yet be “out of shape” and perform poorly.
2. Increasing muscle strength
3. Increasing muscle endurance
-4. Increasing flexibility
5. Increasing aerobic fitness, which helps lower heart disease risk.
-men who expended at least 2,000 kcal per week (equivalent of jogging 20 miles) could expect an average increase in longevity of about 2 years
6. Weight Control.
-In one study, dieters (who didn't exercise) lost both fat and lean tissue, whereas the runners (who didn't diet) lost only fat tissue and retained more lean muscle tissue.
Aerobic fitness can lead to a lowering of resting heart rate, a lowering of resting blood pressure, and an increase in the efficiency of the cardiovascular system.
Overall, studies show that physical activity reduces CVD risk by 35% and a 33% reduction in risk of death due to all causes.
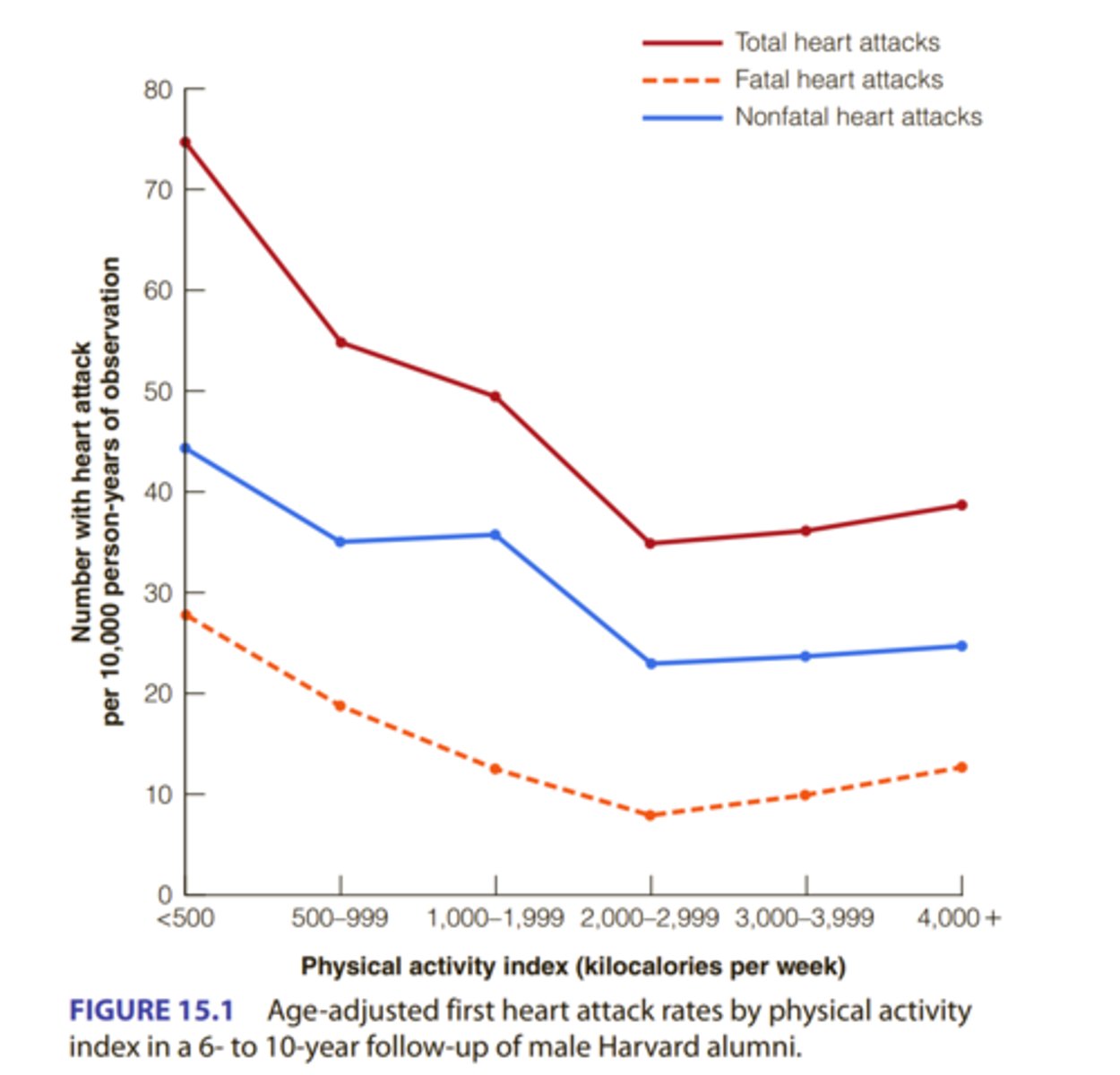
3. Describe the research that supports the link between physical activity and improved cardiovascular health.
Overall, studies show that physical activity reduces CVD risk by 35%
Four research studies:
-1953 - physically active bus drivers had lower rates of heart disease
-1963 - physically active postal workers had lower rates of coronary heart disease
-1970 - coronary heart disease rates lower for physically active longshoremen
-1970 - the least active Harvard alumni had an increased risk of heart attack compared to most physically active
-men who expended at least 2,000 kcal per week (the equivalent of jogging 20 miles) could expect an average increase in longevity of about 2 years
Women and Men Benefit Equally: while earliest studies only had men as participants, later studies indicate that women benefit as much as men from physical activity
4. What are some other physical health benefits of physical activity?
CHOLESTEROL
Research indicates that aerobic exercise can raise HDL levels without raising LDL levels. This results in a more favorable ratio of total cholesterol to HDL and a possible protection against heart disease
PROTECTION AGAINST CANCER
Physical activity offers protection against certain types of cancer, with the strongest evidence for colorectal and breast cancer.
PREVENTION OF BONE DENSITY LOSS
Exercise also protects against osteoporosis, a disorder characterized by a reduction in bone density due to calcium loss that results in brittle bones.
CONTROL OF DIABETES
prevention of Type 2 diabetes, for the management of this condition, and for reduction in mortality risk among diabetics.
Exercise is also an important component in managing Type 1 diabetes.
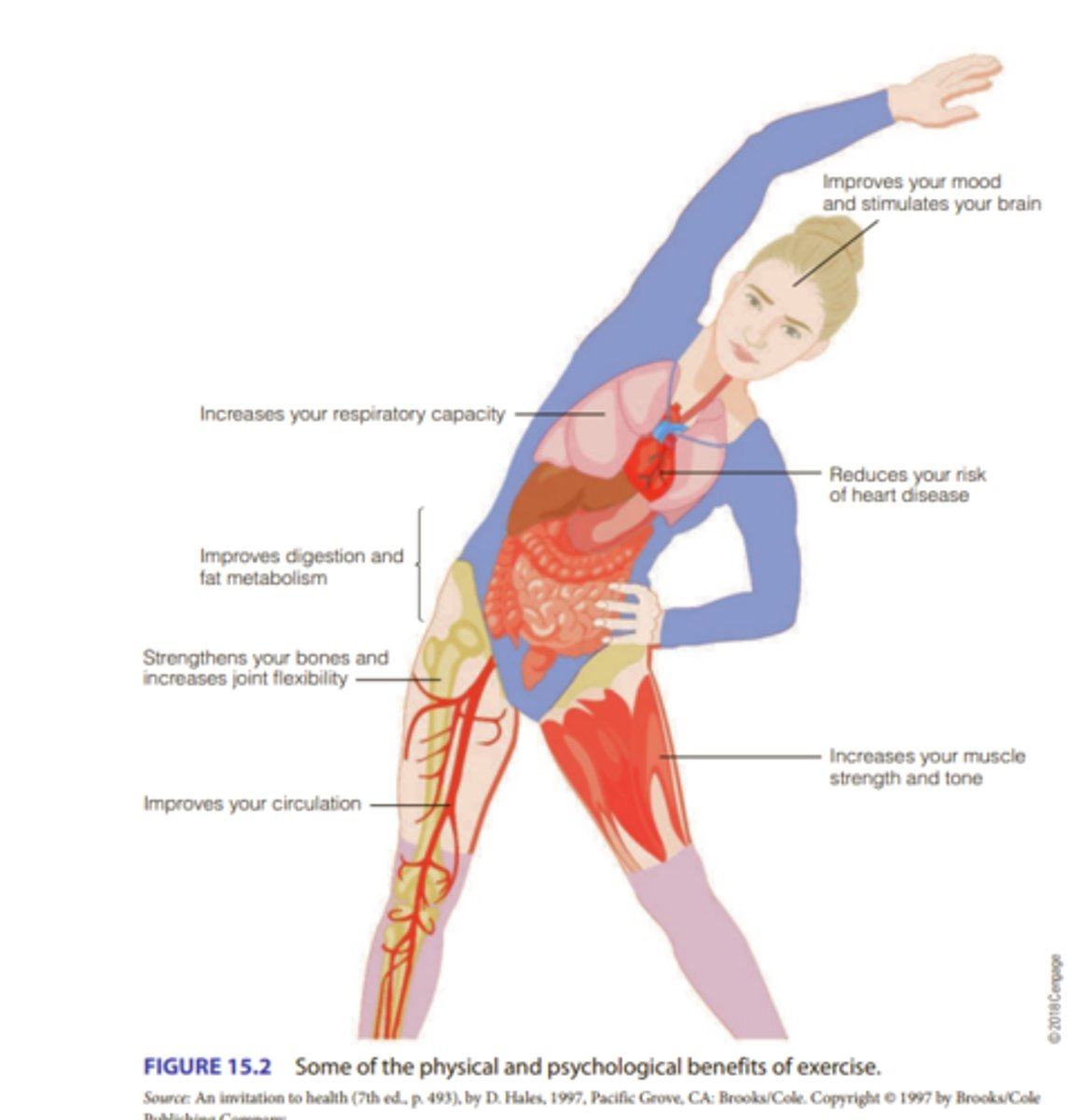
5. What are the mental health benefits of physical activity?
Individuals who exercise are less depressed than those who don’t Physical activity can help reduce state anxiety
Physical activity can also help people deal with stress
STRESS
exercise decreases stress on both a psychological and a physiological level.
DEPRESSION
Aerobic exercise is more effective than no treatment. Physical activity may be at least as effective as psychotherapy. Aerobic and nonaerobic exercise seem to be equally effective in treating depression.
ANXIETY
Exercise is less effective in reducing trait anxiety – a more or less constant personality characteristic. However, it is more effective in reducing state anxiety – a temporary condition aroused by a specific situation.
COGNITIVE FUNCTIONING
Physical activity can improve attention, processing speed, memory, and executive functioning in adults. Physically fit children show better memory performance and greater volume of the hippocampus
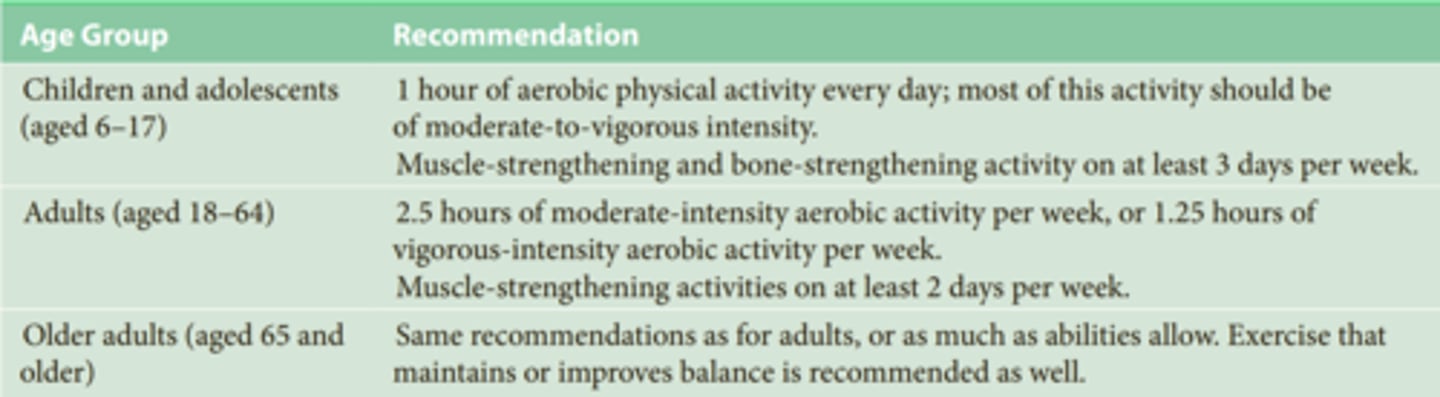
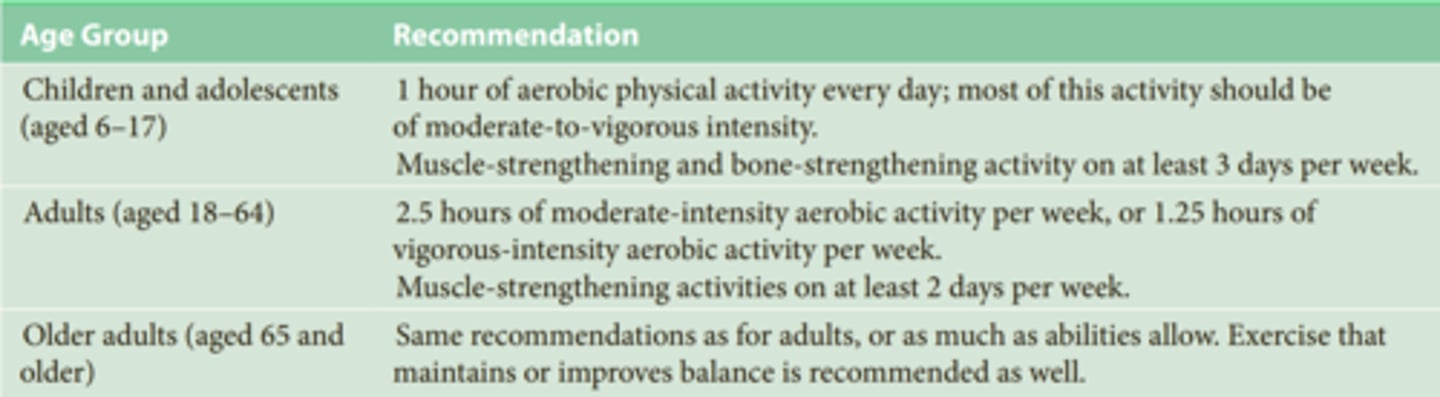
6. What are the differences in exercise recommendations for children/adolescents compared to adults and older adults?
Children and adolescents (aged 6–17)
1 hour of aerobic physical activity every day; most of this activity should be of moderate-to-vigorous intensity. Muscle-strengthening and bone-strengthening activity on at least 3 days per week.
Adults (aged 18–64)
2.5 hours of moderate-intensity aerobic activity per week, or 1.25 hours of vigorous-intensity aerobic activity per week. Muscle-strengthening activities on at least 2 days per week.
Older adults (aged 65 and older)
Same recommendations as for adults, or as much as abilities allow. Exercise that maintains or improves balance is recommended as well.
7. Can physical activity be hazardous? How?
HAZARDS OF PHYSICAL ACTIVITY
Exercise Addiction
● showing strong emotional attachment to exercise
● continuing to exercise while injured
● allowing their activity to take precedence over other aspects of their lives
Injuries from Physical Activity: Injury is more common among infrequent exercisers.
Wearing appropriate clothing decreases the risks of injury during exercise.
Death During Exercise: Nearly all exercise-related deaths from sudden heart attack are attributable to preexisting conditions.
8. How much is enough but not too much?
A healthy adult under age 65 should participate in 30 minutes of moderately vigorous activity five times a week or 20 minutes of vigorous activity three times a week. In addition, people should engage in 8 to 10 strength training exercises for 12 repetitions at least twice a week. These experts described this level of exercise as adequate to protect against chronic disease, including CVD. The moderately vigorous activity recommendations reflect the evidence that less intense exercise produces health benefits and that vigorous exercise is not necessary.
moderate exercise may be superior to more intense activity for some cardiovascular risk factors
However, moderately vigorous activity three times a week will not prompt weight loss or maintain weight loss; those goals require more lengthy and more intense exercise (Garber et al., 2011). Therefore, how much is enough depends on the health goals.
9. What are effective interventions for improving physical activity?
• Informational interventions: increase public awareness of the importance of physical activity and its benefits.
• Behavioral and social interventions:
- Behavioral: teach people skills so they can adopt and maintain physical activity.
- Social: “Buddy systems”/social support are effective ways to increase exercise.
• Environmental interventions: enhance access to places for physical activity (e.g., sidewalks, parks, playgrounds).
Chapter 16 – Future Challenges
1. What do the terms "well-year," "health expectancy," and "health disparity" refer to?
“Well-year”: a completely well year; void of ill-being or health-related problems
● Life expectancy is increasing, but well-years are decreasing in the US
“health expectancy”: the number of years a person is free from disability
“health disparity”: health differences that are linked with social, economic, and/or environmental disadvantages (race/ethnicity, education, income, gender, sexual orientation, disability, geographic location)
● Most documented: racial and ethnic disparities
● Education and SES disparities also play a large role.
African Americans and Native Americans experience great disadvantages compared with Asian Americans and European Americans. Some Hispanics experience health advantages and others disadvantages

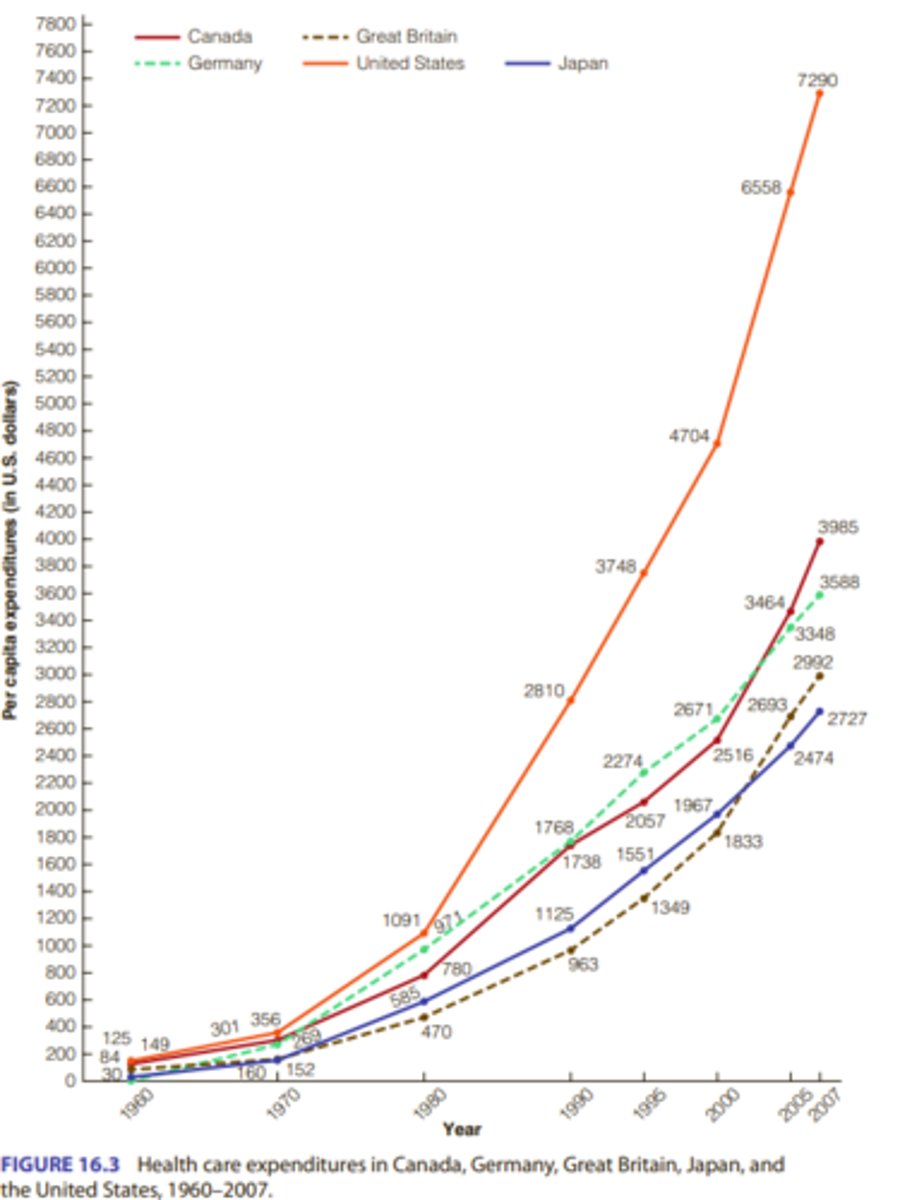
2. Where does the United States rank in health expectancy and health care costs among the countries of the world?
The US has lower health expectancy than any other nation of comparable wealth and level of development

Where does the United States rank in health care costs among the countries of the world?
The US has higher healthcare expenditures than other industrialized countries such as Canada, Great Britain, Germany, and Japan.
3. How do ethnic groups within the United States compare on health expectancy and life expectancy?
• African Americans have a shorter life and lower health expectancy than European Americans
• African Americans also have higher infant mortality rates, homicide deaths, rates of CVD, cancer mortality, diabetes rates
• some causes:
• Inadequate medical treatment and access to medical care• Limited health literacy
• Discrimination in medical treatments
• Native Americans also have a shorter life expectancy than European Americans
• Native Americans also have higher infant mortality rates, mortality rates, and higher rates of infectious illness than European Americans
• Low economic status, lack of access to medical care, and poor health literacy may also explain these disparities.
• Hispanics do not show poorer health rates as much as African Americans do
• However, Hispanics are more likely to develop diabetes, obesity and hypertension compared to European Americans
• Asian Americans have longest life expectancy and best health of any ethnic group in the US
• Asian Americans have lower infant mortality, longer life expectancy, fewer lung and breast cancer deaths, and lower CVD rates than other ethnic groups.
4. What is the difference between primary and secondary prevention?
• Primary prevention: avoids the development of a disease: Immunizations, Lifestyle changes (diet, exercise, stress management, alcohol and drug use, risky behavior, happiness and positive emotions)
• Secondary prevention: aims at early disease detection, thereby increasing opportunities for interventions to prevent the progression of the disease and emergence of symptoms (regular physical exams and cancer screening, cholesterol, and blood pressure testing).
About 70% of the cost of medical care is spent on 10% of the population, whereas healthy people (about 50% of the population) account for about 3% of medical care expenditures. These statistics highlight the importance of maintaining and promoting health as a way to contain medical care costs. Thus, health psychologists can have a role in reducing medical care costs because unhealthy behaviors contribute to the chronic diseases that generate the majority of expenses