Mitral Valve Prolapse + Flail leaflets
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
MVP definition
Posterior displacement of any porIon of the MV leaflets beyond the MV annular plane during ventricular systole
other names for MVP
Barlow Syndrome
Floppy Valve Syndrome
Systolic Click-Murmur Syndrome
MVP classifications
Classic
Non-classic
Secondary (functional)
echocardiographic types
Classic MVP = primary myxomatous
Increased thickening of MV leaflets
Causes of classic MVP
Fibrosis
Mitral annular dilatation
Chordal redundancy/lengthening
Fibrin deposits
Classic mitral valve prolapse can be ____ or ______
Familial or Nonfamilial
Non-classical MVP
No thickening or plumping of leaflets
Systolic superior displacement of MV leaflets
Non-classical MVP is characterized by:
Mid-systolic click
Displacement of leaflets >2 mm
Valve thickness <5mm (no thickening)
MR absent or minimal
Secondary (functional) MVP
reduction/alteration of the LV size/shape
causes normal MV leaflets to move past the MV annulus
causes of secondary/functional MVP
CAD
RHD
dilated or hypertrophic CM
Left-to-right shunting
ASD
Severe TR
Ebstein’s anomaly
Primary pulmonary hypertension
Pericardial effusion
echocardiographic types of MVP
mid to late systolic
holosystolic
signs and symptoms of MVP
★ AsymptomaIc with normal, asthenic phenotype (appearance)
PalpitaIons – most common presenIng symptom
Chest pain – atypical
Dyspnea, exercise intolerance
Presyncope/syncope
Neuropsychiatric symptoms (anxiety, panic alacks)
Cerebrovascular symptoms of TIA, CVA, amaurosis fugax
Heart failure due to significant MR
Complications of MVP
★ MR – progressive
• InfecIve endocardiIs (MVP is leading cause)
• Embolic events due to fibrin emboli
• Ruptured chordae tendinae with acute MR
• Arrhythmias due to conducIon defects – SVT most common
• Heart failure
• Pulmonary hypertension
• Acute pulmonary edema
• Sudden death (rare) due to ventricular arrhythmias
auscultation for MVP
mid to late systolic click
due to sudden tensing of chordae
with or without late systolic murmur due to associated MR
accentuated S1
EKG findings for MVP
Normal
inverted/biphasic T waves in leads II, III, aVF
Non specific ST changes
Arrhythmias – SVT, PVC
ConducIon disturbances – first degree A-V block, WPW
LAE with M
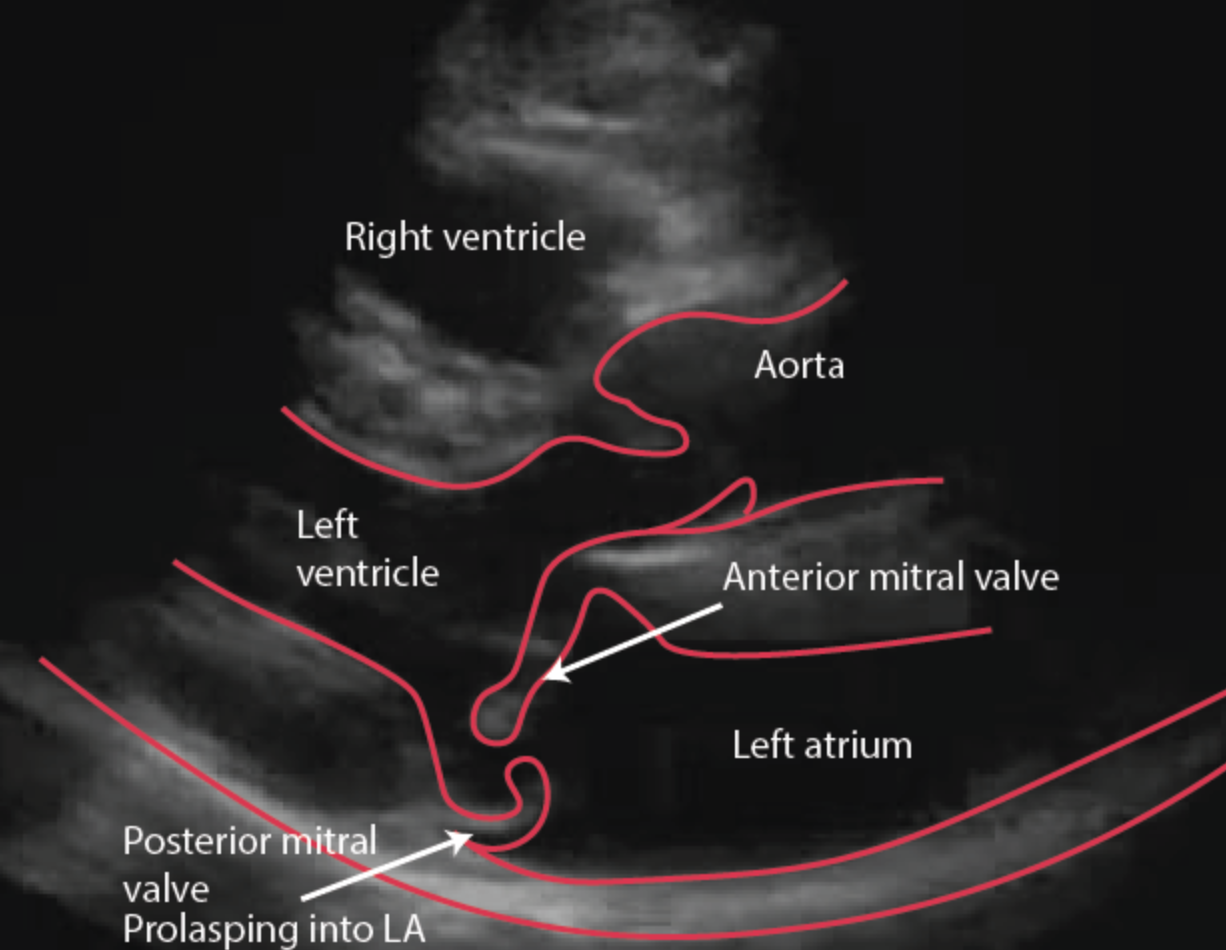
what is the 2D view of choice for MVP?
PLAX
Echo findings - 2D PLAX
criteria for diagnosis of MVP
Diffuse leaflet thickening > 5 mm myxomatous appearance (classic MVP)
Scalloped appearance of the involved MV leaflet in PSAX
ElongatIon of the chordae
LAE (MR)
LV volume overload palern (LV dilatatIon and hyperkinesis)
Criteria for diagnosis of MVP - anterior leaflet
any porIon of the leaflet protrudes beyond the annular plane
≥ 2 mm in PLAX
≥ 1 cm (10 mm)
Criteria for diagnosis of MVP - posterior leaflet
any portion of the leaflet protruding > 2 mm beyond the annular plane with visualization of the various scallops in different
views:
− PLAX and AP 3-Ch for A2 & P2
− AP 4-Ch and AP 5-Ch for A3 & P1
− AP 2-Ch for A1 & P3
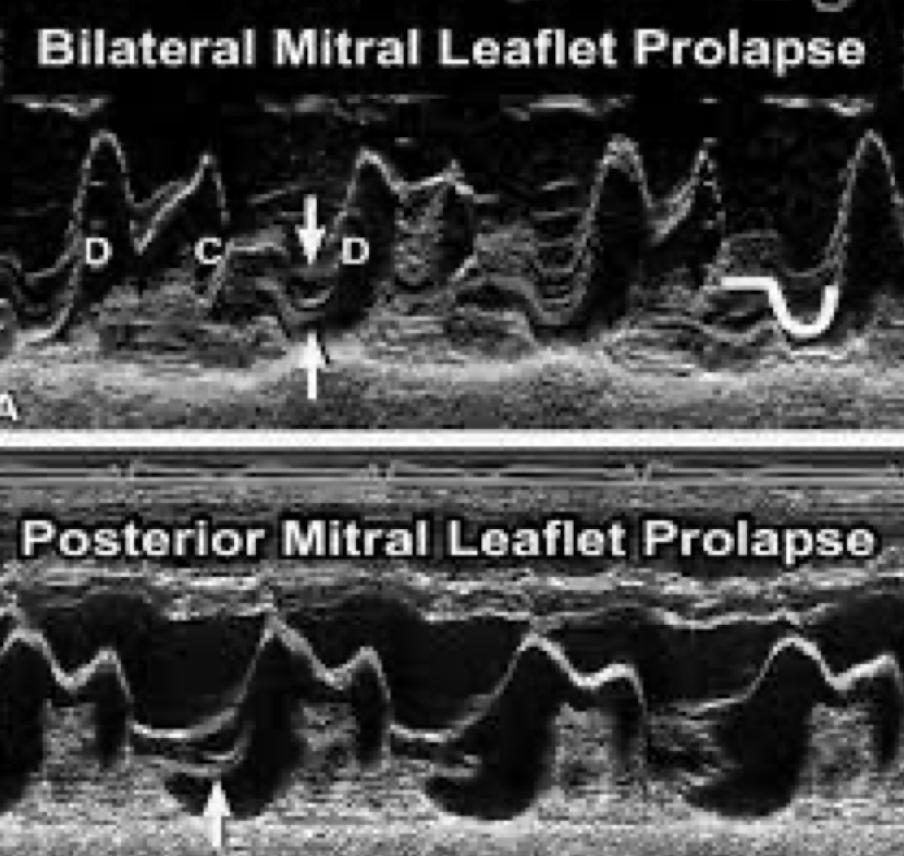
M-mode findings
mid to late systolic “sagging” back of the anterior, posterior or both MV leaflets > 2 mm from the C-D points
holosystolic (pansystolic) “sagging” back of the anterior, posterior or both MV leaflets from ≥ 3 mm from the C-D points of the MV
Doppler findings
in occurrence of severe MR in MVP
DilatIon of the mitral annulus between 14 – 18 cm (N = 9 cm)
Rupture of chordae tendineae with or without mitral annular dilataIon
Treatment for MVP
None for asymptomatIc patients, good hydration to prevent volume depletion
Antibiotoic prophylaxis before minor surgical and dental procedures
CessatIon of stimulants: caffeine, alcohol
InvestIgatIon of arrhythmias/conductIon disturbances: EP study, Holter monitor, exercise stress test
Beta-blockers, antiarrhythmics
AntIcoagulatIon (LAE)
ASA therapy for TIA, CVA patients
MV replacement – TEE evaluation necessary pre and post operation
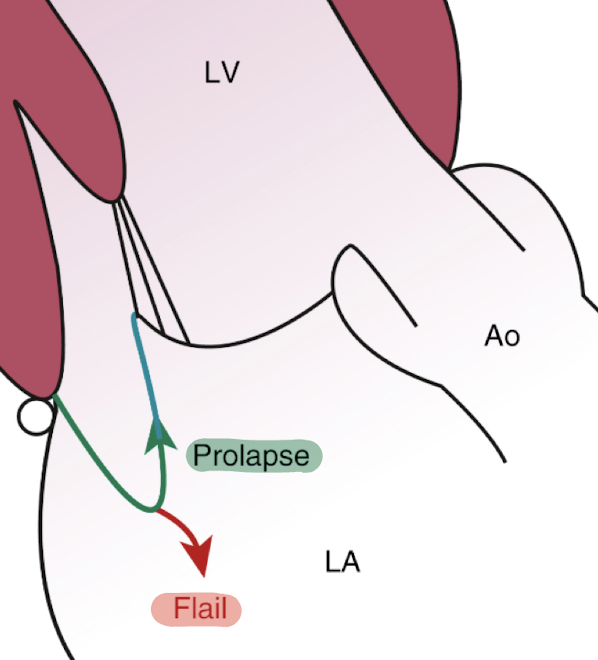
Flail MV leaflets
a severe form of mitral valve prolapse where a leaflet segment ruptures and swings backward into the left atrium during systole
difference between flail and prolapse
Prolapse - leaflet protrudes into LA, but is still attached to chordae
Flail - not attached to chordae, “flailing” around LA
rupture of several isolated chordae → _____
absent MR
rupture of entire PM or PM head → _____
acute severe MR
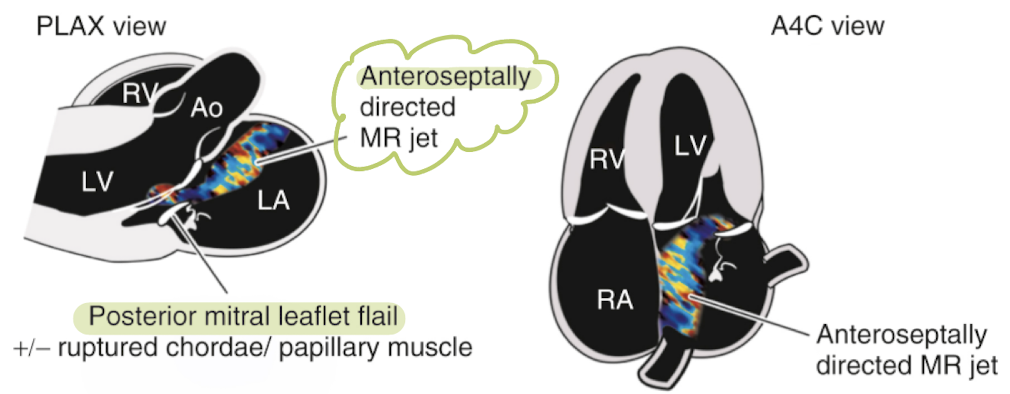
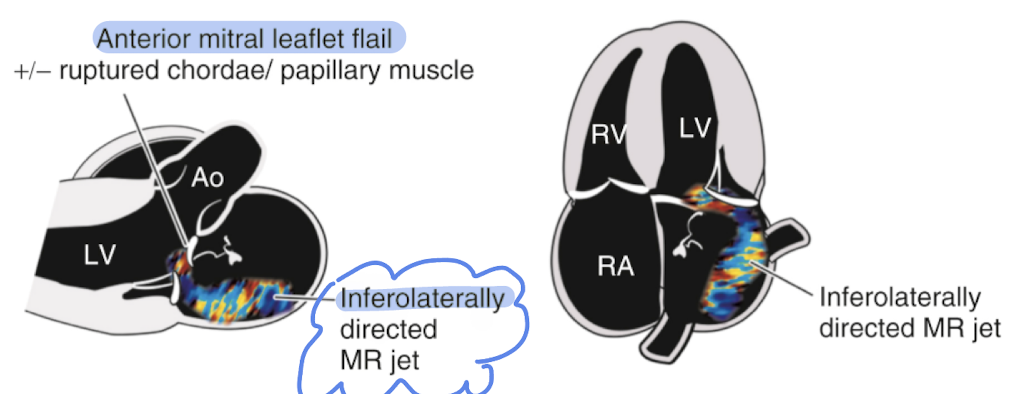
MR jet with flail leaflet will be ____ with an orientation ____ in direction to defect leaflet
eccentric
opposite
ruptured posterior chordae + flail posterior leaflet → _____ jet
anteroseptal MR
ruptured anterior chordae + flail anterior leaflet → _____ jet
postero / inferolateral MR
CW appearance of flail leaflets
Due to the eccentric jet, the MR spectral signal may have an atypical appearance due to the CW cursor intersecting the jet partially.
This may result in varying density and velocity of the signal, mimicking _______
less than a holosystolic jet
if there are parts of the flail portions that oscillate in the regurgitation flow stream, they result in a “______” appearance of the spectral signal associated with a “_____” sound
tiger stripe
whistling
Surgical repair of flail leaflets
Partial flail: placing of annuloplasty ring + resection of flail portion
Placement of prosthetic chordae
Chordal shortening procedures
TranslocatIon of chordae from one leaflet to another
carpentier’s functional classification of MR is based on…
the opening and closing motion of both leaflets
Based on leaflet motion, there are 3 types of functional mitral regurgitation
type I MR
type II MR
type III MR
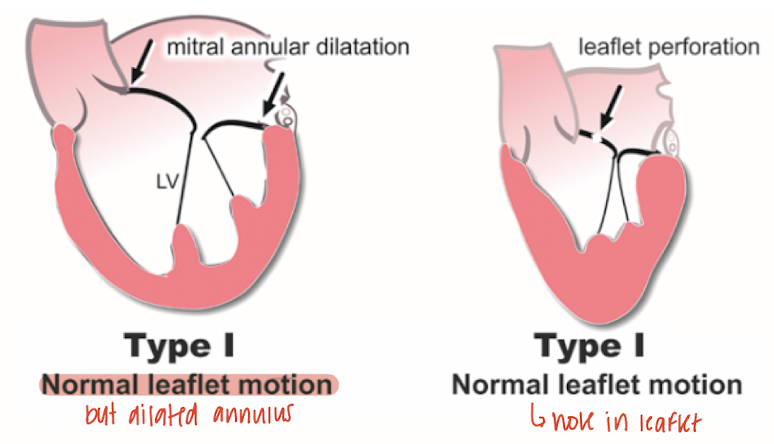
type I MR
MR occurs despite normal leaflet motion
cause: annular dilatation (dilated CM) or leaflet perforation (sequelae of endocarditis)
MR jet is central
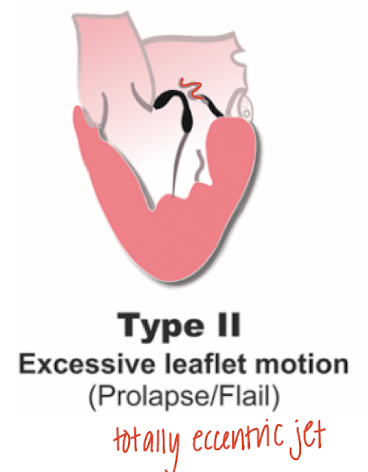
type II MR
Occurs because of leaflet prolapse due to simple elongation of the leaflet or flail leaflet due to chordal /PM rupture
MR jet is eccentric
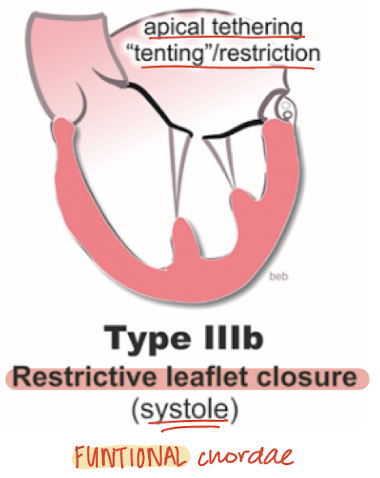
type III MR - a
Restricted leaflet motion (in systole and diastole)
Valvular/subvalvular thickening
MAC due to aging, sequelae of RHD
MR jet can be eccentric/central

type III MR - b
Restricted leaflet motion (in systole)
Displacement of PM (elongation associated with dilated CM), chordae apical tethering
MR jet is central